Myocardial infarction in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the detailed answer:
Myocardial Infarction - Comprehensive Review
1. Definition
Myocardial infarction (MI) is necrosis of cardiac muscle resulting from sustained ischemia. The 2018 joint task force of U.S. and European Cardiology groups defines it as "the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
- Robbins & Kumar Basic Pathology calls it "necrosis of the heart muscle resulting from ischemia"
- Roughly 800,000 individuals in the United States experience an MI each year - nearly one MI every 40 seconds - causing almost 400,000 deaths annually
- ~605,000 new AMIs per year in the U.S. (Harrison's, 22nd Ed.)
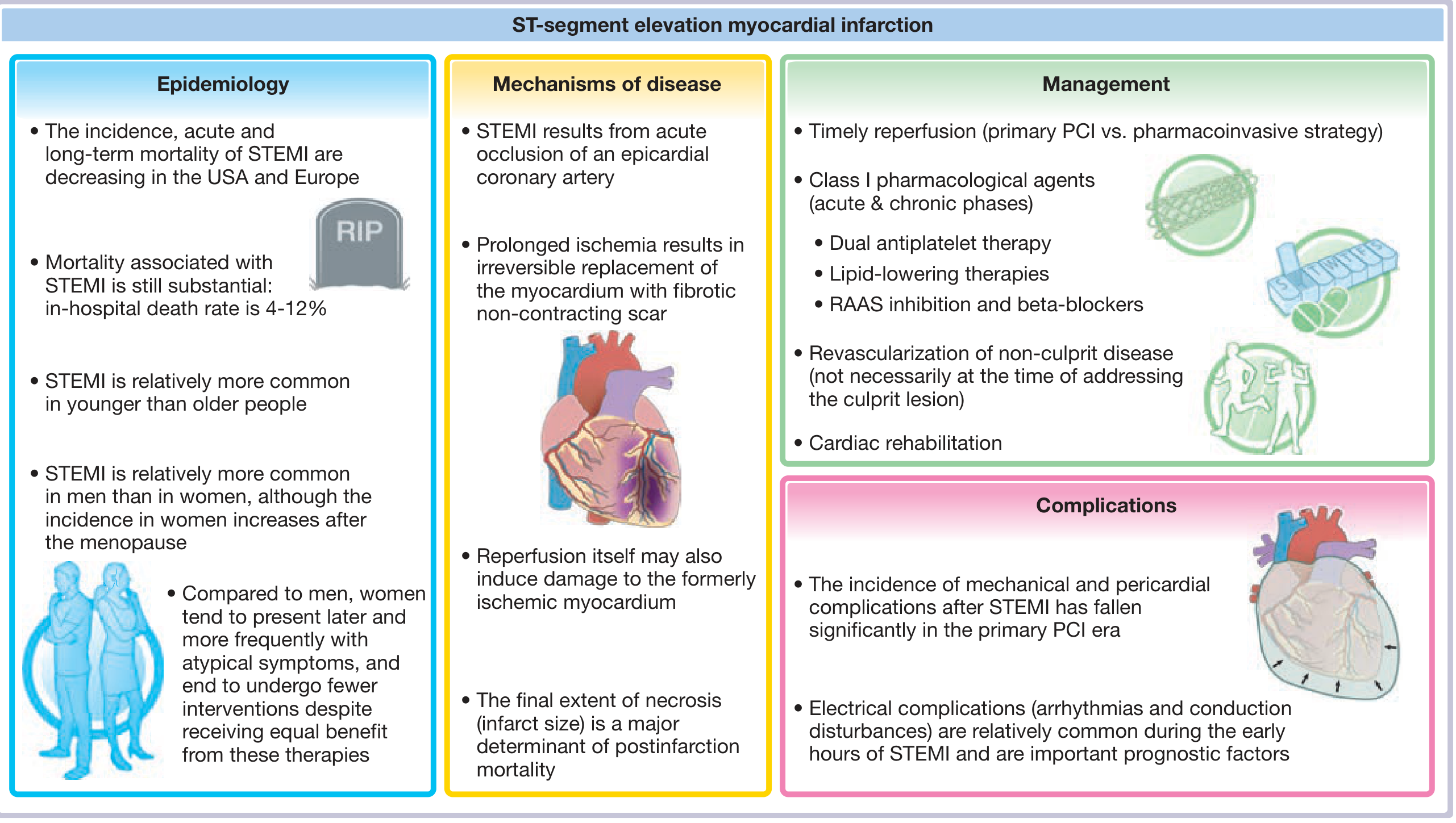
2. Epidemiology
| Feature | Detail |
|---|---|
| Age | ~10% occur before age 40; 45% before age 65 |
| Sex | Men > women during reproductive years; gap narrows after menopause |
| Menopause | Declining estrogen accelerates CAD; IHD is the #1 cause of death in older women |
| In-hospital mortality | STEMI ~9%; NSTEMI ~6%; overall <7% with modern treatment |
| Out-of-hospital STEMI | ~1/3 die before reaching hospital, usually from arrhythmia within 1 hour |
| 1-year mortality post-AMI | ~15%; ~4x higher in patients >75 years |
3. Classification
By ECG Pattern
- STEMI (ST-Elevation MI): Complete occlusion; full-thickness (transmural) risk; requires immediate reperfusion
- NSTEMI (Non-ST-Elevation MI): Incomplete occlusion; subendocardial/non-transmural; elevated troponins without ST elevation
- Unstable Angina (UA): Plaque disruption with ischemia but no troponin elevation
By Depth
- Transmural infarction: Full thickness necrosis; corresponds to STEMI pattern
- Subendocardial infarction: Limited to inner 1/3 of myocardium; most susceptible due to highest intramural compressive pressure and furthest from epicardial vessels
Universal Classification (ESC/ACC Types)
| Type | Mechanism |
|---|---|
| Type 1 | Spontaneous MI from plaque rupture/erosion with thrombosis |
| Type 2 | Ischemia due to supply/demand mismatch (e.g., spasm, anemia, tachycardia) |
| Type 3 | Sudden cardiac death before biomarkers can be obtained |
| Type 4 | PCI-related MI |
| Type 5 | CABG-related MI |
4. Etiology and Risk Factors
Primary cause (>90%): Atherosclerotic coronary artery disease
The remaining ~10% include:
- Coronary vasospasm (Prinzmetal angina; cocaine/ephedrine use)
- Embolism - from mural thrombus in AF, infective endocarditis vegetations, prosthetic valves, or paradoxical emboli via PFO
- Vasculitis of small intramyocardial arterioles
- Amyloid deposition in vessel walls
- Sickle cell disease (stasis)
- Aortic stenosis with marked hypertrophy
- Dissection of a coronary artery
- Profound hypotension/shock
Modifiable risk factors (accelerate atherosclerosis):
- Cigarette smoking
- Hypertension
- Hyperlipidemia (especially LDL elevation)
- Diabetes mellitus
- Obesity
- Physical inactivity
Non-modifiable: Age, male sex, family history
5. Pathogenesis
Step-by-Step Sequence (Typical STEMI)
-
Plaque disruption: An atheromatous plaque is eroded or ruptured by endothelial injury, intraplaque hemorrhage, or mechanical forces - exposing subendothelial collagen and necrotic plaque contents to blood. Plaques most prone to rupture have a rich lipid core and thin fibrous cap.
-
Platelet activation: Platelets adhere, aggregate, and are activated - releasing thromboxane A2, ADP, and serotonin - causing further platelet aggregation and vasospasm.
-
Coagulation cascade: Tissue factor exposure activates coagulation, adding to the growing thrombus. The glycoprotein IIb/IIIa receptor converts to a high-affinity state for fibrinogen, enabling platelet cross-linking and aggregation.
-
Complete occlusion: Within minutes, the thrombus can evolve to completely occlude the coronary artery lumen.
Evidence: Angiography within 4 hours of MI onset demonstrates coronary thrombosis in ~90% of cases. At 12-24 hours, only 60% show thrombus (some clear spontaneously).
Cellular Response to Ischemia
| Time After Occlusion | Event |
|---|---|
| Seconds | Aerobic metabolism ceases; creatine phosphate and ATP production fails; lactic acid accumulates |
| ~1 minute | Myocardial contractility ceases (before cell death) |
| Minutes | Ultrastructural changes: myofibrillar relaxation, glycogen depletion, mitochondrial swelling |
| 20-30 min | Irreversible necrosis begins (if flow <10% of normal) |
| 6-12 hours | Necrosis becomes complete |
| Hours to days | Sarcolemmal disruption - intracellular proteins leak into circulation (basis of biomarkers) |
Key: Cardiac muscle requires ~1.3 mL O2/100g/min just to stay alive. If ≥15-30% of normal resting coronary flow is preserved, the muscle will not die. The central core of a large infarct often has near-zero collateral flow and dies.
Why Subendocardium First?
The subendocardial region is most vulnerable because:
- It is the last zone to receive blood from epicardial vessels
- It experiences the highest intramural compressive pressure during systole
- It has the highest oxygen consumption
With prolonged ischemia, a wavefront of cell death moves centripetally from the subendocardium outward toward the epicardium.
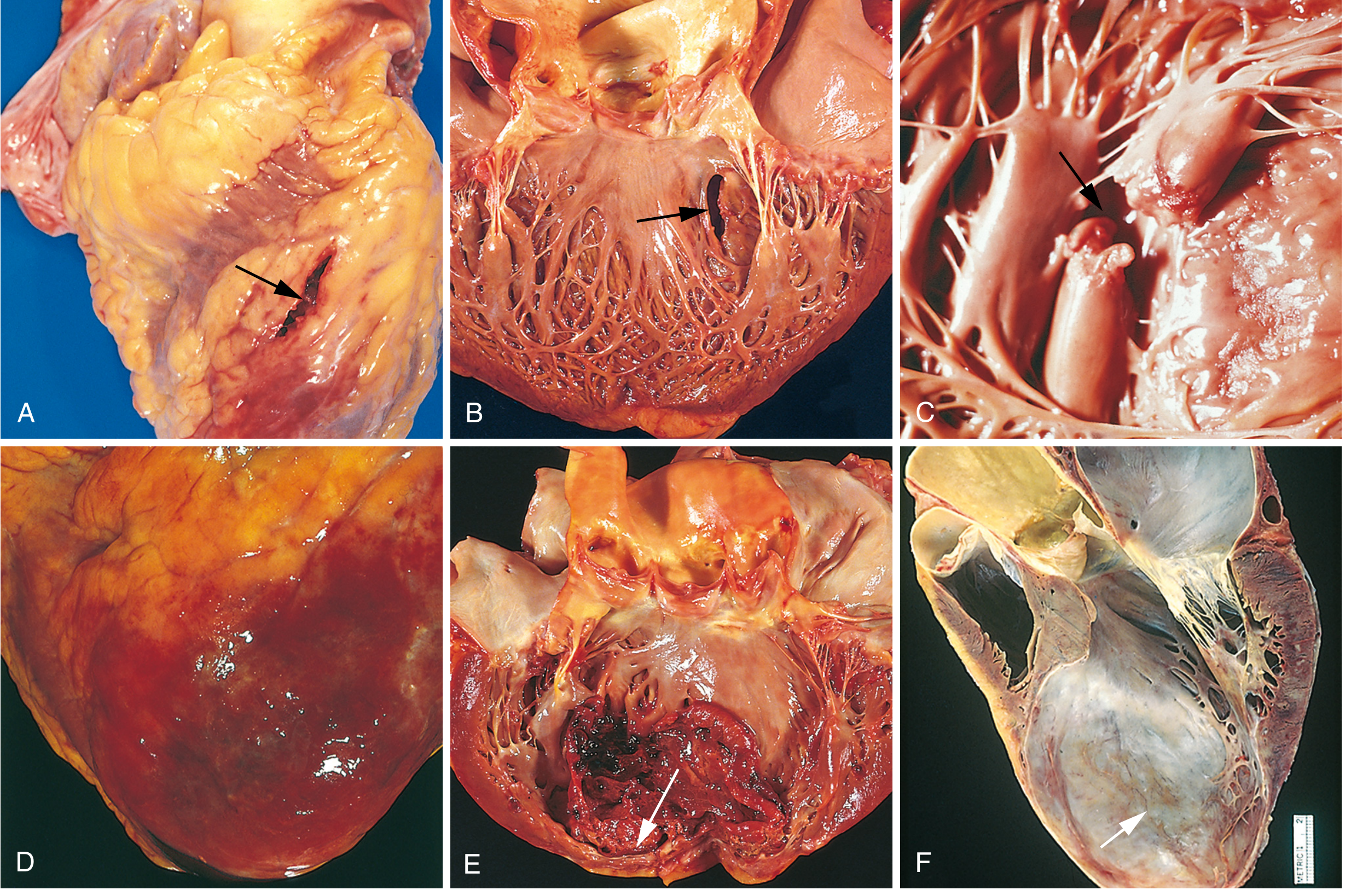
6. Morphological Changes (Gross and Microscopic)
Gross Pathology
| Time | Gross Appearance |
|---|---|
| 0-12 hours | Usually normal; may stain negative with TTC (triphenyl tetrazolium chloride) |
| 12-24 hours | Subtle pale/yellow area; hyperemia |
| 1-3 days | Yellow-tan, soft, increasingly well-demarcated; surrounding hyperemic rim |
| 3-7 days | Yellow-tan, soft center; maximal softening (highest rupture risk) |
| 1-2 weeks | Yellow-tan center, red-gray vascularized margins |
| 2-8 weeks | Progressively gray-white |
| >2 months | Dense white fibrous scar |
Microscopic Pathology
| Time | Microscopic Changes |
|---|---|
| 0-0.5 hr | Reversible: wavy fibers, glycogen depletion, mitochondrial swelling |
| 0.5-4 hr | Coagulation necrosis begins; "contraction bands" in reperfused areas |
| 4-12 hr | Early coagulative necrosis; pyknotic nuclei; edema; hemorrhage |
| 12-24 hr | Coagulative necrosis with loss of nuclei; neutrophil infiltration begins |
| 1-3 days | Dense neutrophil infiltration; myofiber "ghosts" (outlines without nuclei) |
| 3-7 days | Macrophage infiltration; phagocytosis of dead cells; granulation tissue at margins |
| 1-3 weeks | Vascular granulation tissue; collagen deposition begins |
| >3 weeks | Dense fibrous scar forms |
7. Clinical Features
Symptoms
| Feature | Details |
|---|---|
| Chest pain | Severe, crushing, pressure-like; classically substernal; radiation to left arm, jaw, shoulder, or back |
| Duration | >20 minutes (vs. stable angina which resolves in <20 min) |
| Associated symptoms | Diaphoresis, nausea/vomiting, dyspnea, lightheadedness, sense of impending doom |
| Silent MI | Common in diabetics, elderly, and women; no chest pain; presents with dyspnea or fatigue |
Atypical presentations (more common in women, diabetics, elderly):
- Epigastric pain / indigestion
- Back or jaw pain without chest pain
- Exertional dyspnea
- Syncope or palpitations
Physical Examination
- Pallor, diaphoresis, anxiety
- Tachycardia or bradycardia (inferior MI with vagal activation)
- Hypotension (cardiogenic shock) or hypertension (pain/catecholamine surge)
- S4 gallop (reduced LV compliance)
- S3 gallop (large infarct with LV dysfunction)
- Mitral regurgitation murmur (papillary muscle dysfunction)
- Pericardial friction rub (Dressler syndrome or early fibrinous pericarditis)
- Jugular venous distension (right ventricular infarction)
8. Diagnosis
ECG Changes
The ECG is the pivotal diagnostic and triage tool - distinguishing STEMI from NSTEMI.
Three major ECG abnormalities in acute MI (Ganong's Physiology):
| Defect in Infarcted Cells | Current Flow | ECG Change (in leads over infarct) |
|---|---|---|
| Rapid repolarization | Out of infarct | ST segment elevation |
| Decreased resting membrane potential | Into infarct | TQ segment depression (manifested as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
Evolutionary ECG changes:
- Hyperacute T waves (minutes): Tall, peaked T waves (earliest change)
- ST elevation (minutes to hours): Hallmark of acute transmural injury; reciprocal ST depression in opposite leads
- Q waves (hours to days): Pathologic Q waves (>40 ms wide, >25% of R amplitude) indicate transmural necrosis - electrically silent dead tissue
- T-wave inversion (days to weeks): Persists for weeks
- Normalization: ST segments normalize over days; Q waves often persist permanently
Leads and corresponding territory:
| ECG Leads | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior wall | LAD |
| I, aVL, V5-V6 | Lateral wall | LCx |
| II, III, aVF | Inferior wall | RCA (usually) |
| V1, tall R in V1-V2 | Posterior wall | RCA or LCx |
| V1 ST elevation + right-sided leads | Right ventricle | RCA |
Biomarkers
| Marker | Rise | Peak | Normalizes | Notes |
|---|---|---|---|---|
| Cardiac Troponin I/T | 2-4 hr | 24-48 hr | 7-14 days | Most sensitive and specific; gold standard |
| CK-MB | 3-6 hr | 12-24 hr | 2-3 days | Useful for reinfarction detection |
| Myoglobin | 1-2 hr | 4-8 hr | 24 hr | Earliest but non-specific |
- Troponin levels rise to 20-50x the upper reference limit in classic MI
- Early reperfusion causes earlier peak of biomarkers (rapid washout from infarct zone)
- WBC: Polymorphonuclear leukocytosis (12,000-15,000/µL) peaks within 3-7 days
- ESR: Rises more slowly, peaks in first week, may stay elevated for 1-2 weeks
Imaging
- Echocardiography: Wall motion abnormalities almost universally present; useful for LV function assessment, complications detection
- Coronary angiography: Definitive - shows occlusion site; allows immediate PCI
- Cardiac MRI: Gold standard for infarct size quantification; late gadolinium enhancement
- Nuclear imaging (SPECT): Perfusion defects; used for risk stratification
9. Management
Immediate (First 10-30 minutes) - "MONA" + antiplatelet
| Drug | Dose/Route | Rationale |
|---|---|---|
| Oxygen | If SpO2 <90% | Correct hypoxia |
| Morphine | IV 2-4 mg | Analgesia; reduce sympathetic activation |
| Aspirin | 325 mg chewed immediately | Irreversible COX-1 inhibition; antiplatelet |
| Nitroglycerin | SL or IV | Pain relief, preload reduction (avoid if hypotensive or RV infarct) |
Reperfusion (the Core Treatment)
Primary PCI (preferred) - Goal: door-to-balloon time <90 minutes (within 120 min if transferred)
- Mechanical recanalization of the occluded artery by balloon inflation and stent placement
- Superior to thrombolysis when performed within 120 min of first medical contact
Fibrinolysis (thrombolysis) - when primary PCI is not available within time targets
- Alteplase (tPA) - tissue plasminogen activator
- Reteplase - bolus dosing; easier to administer
- Tenecteplase (TNK) - single bolus; most fibrin-specific
- Streptokinase - older agent; not fibrin-specific; approved for acute MI, PE, DVT
- Time window: Up to 12 hours after symptom onset; most effective within 3 hours
Contraindications to fibrinolysis:
- Any prior intracranial hemorrhage
- Recent stroke (<3 months)
- Active internal bleeding
- Suspected aortic dissection
- Severe uncontrolled hypertension (>180/110)
Antiplatelet Therapy
| Drug | Mechanism | Notes |
|---|---|---|
| Aspirin | COX-1 inhibitor | Lifelong after MI |
| Clopidogrel | P2Y12 inhibitor | 75 mg/day; 12 months post-MI (DAPT) |
| Ticagrelor | P2Y12 inhibitor (reversible) | 90 mg BID; faster onset than clopidogrel |
| Prasugrel | P2Y12 inhibitor (irreversible) | Preferred with PCI; avoid if prior stroke/TIA |
| GP IIb/IIIa inhibitors | Block fibrinogen binding to platelets | Eptifibatide, tirofiban; used perioperatively in high-risk PCI |
Anticoagulation
| Drug | Use |
|---|---|
| Unfractionated heparin (UFH) | IV bolus + infusion during PCI |
| LMWH (enoxaparin) | Preferred for NSTEMI; predictable dosing |
| Bivalirudin | Direct thrombin inhibitor; used in PCI |
| Fondaparinux | Factor Xa inhibitor; used in NSTEMI if conservative management |
Long-term Secondary Prevention (Post-MI)
| Drug | Rationale |
|---|---|
| Beta-blockers (metoprolol, carvedilol) | Reduce HR, myocardial O2 demand, ventricular remodeling; reduce sudden death |
| ACE inhibitors/ARBs (ramipril, lisinopril) | Reduce afterload, prevent LV remodeling; mandatory if EF <40% |
| Statins (high-intensity: rosuvastatin 40 mg, atorvastatin 80 mg) | Plaque stabilization, LDL reduction; reduce mortality |
| Aspirin (81 mg/day) | Lifelong |
| Eplerenone/Spironolactone | Aldosterone antagonist; indicated if EF <40% + HF or diabetes |
NSTEMI/UA Management
- Antiplatelet + anticoagulation
- Stratify risk using TIMI score or GRACE score
- Invasive strategy (coronary angiography + PCI) preferred for high-risk patients
- Conservative (ischemia-driven) strategy for low-risk patients
10. Complications
Nearly three-quarters of patients experience one or more complications post-MI:
Mechanical Complications
| Complication | Time | Features |
|---|---|---|
| Free wall rupture | 3-7 days (peak) | 1-3% of MIs; rapidly fatal hemopericardium + cardiac tamponade |
| Ventricular septal rupture (VSD) | 3-5 days | Left-to-right shunt; harsh pansystolic murmur; high mortality without surgery |
| Papillary muscle rupture | 2-7 days | Acute severe mitral regurgitation; pulmonary edema; high mortality |
| Papillary muscle dysfunction | Subacute | Common; ischemic mitral regurgitation without rupture |
| LV aneurysm | Weeks to months | Thinned, fibrotic, non-contracting bulge; risk of mural thrombus + embolism |
| LV pseudoaneurysm | Days-weeks | Contained free wall rupture - hemopericardium contained by pericardium |
| Mural thrombus | Days-weeks | Forms over akinetic wall; source of systemic embolism |
Electrical Complications
| Arrhythmia | Notes |
|---|---|
| Ventricular fibrillation | Most common cause of early out-of-hospital death |
| Ventricular tachycardia | Non-sustained or sustained; defibrillate if pulseless |
| Accelerated idioventricular rhythm | "Reperfusion arrhythmia"; benign; no treatment needed |
| Sinus bradycardia / AV block | Inferior MI (RCA); vagal; may need atropine or temporary pacing |
| Complete heart block (3rd degree) | Inferior MI: usually transient; anterior MI: often permanent, high mortality |
Other Complications
| Complication | Notes |
|---|---|
| Cardiogenic shock | Occurs in ~10% of transmural MIs; >40% LV damage; mortality >50% without support |
| Acute heart failure / pulmonary edema | Common; manage with diuretics, vasodilators, O2 |
| Right ventricular infarction | 1-3% isolated; common with inferior MI; treat with IV fluids (NOT diuretics) |
| Pericarditis | Early (2-4 days): fibrinous pericarditis overlying infarct; Dressler syndrome (2-10 weeks): immune-mediated |
| Infarct expansion | Thinning and stretching of infarcted wall segment, leading to aneurysm formation |
11. Cardiogenic Shock - Special Mention
- Defined as systolic BP <90 mmHg + signs of hypoperfusion + elevated filling pressures
- Occurs when 40% or more of LV is damaged
- Causes of death: (1) decreased cardiac output, (2) pulmonary venous congestion/pulmonary edema, (3) ventricular fibrillation, (4) cardiac rupture (Guyton & Hall)
- Systolic stretch: Non-functional segments bulge outward during systole, further reducing effective cardiac output
- Treatment: Immediate revascularization (PCI/CABG), vasopressors (norepinephrine), inotropes (dobutamine), mechanical circulatory support (IABP, Impella, VA-ECMO)
12. Reperfusion Injury
When ischemic myocardium is reperfused, a paradoxical injury can occur:
- Calcium overload in previously ischemic cells
- Reactive oxygen species burst
- Mitochondrial permeability transition pore (mPTP) opening
- Manifests as: contraction band necrosis, ventricular arrhythmias, microvascular obstruction ("no-reflow"), myocardial stunning
13. Prognosis and Risk Stratification
Favorable factors:
- Small infarct size
- Preserved EF (>50%)
- Early reperfusion
- No complications
- Absence of heart failure
Prognostic tools:
- TIMI Risk Score: Predicts 30-day mortality in STEMI
- GRACE Score: Validated for NSTEMI/UA risk stratification
- LVEF (measured by echo): Single strongest predictor of long-term prognosis
- EF <35-40%: Indication for ICD (if persists >40 days post-MI)
- EF <40%: ACE inhibitor mandatory; consider aldosterone antagonist
14. Summary Table
| Feature | STEMI | NSTEMI | UA |
|---|---|---|---|
| ECG | ST elevation | ST depression / normal | ST depression / T-wave changes |
| Troponin | Elevated | Elevated | Normal |
| CK-MB | Elevated | Elevated | Normal |
| Vessel occlusion | Complete | Partial | Partial |
| Infarct depth | Transmural | Subendocardial | No necrosis |
| Reperfusion urgency | Immediate (<90 min PCI) | Early invasive (2-24 hr) | Risk-stratified |
Sources: Robbins & Cotran Pathologic Basis of Disease (10th Ed.) | Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine (22nd Ed., 2025) | Ganong's Review of Medical Physiology (26th Ed.) | Guyton & Hall Textbook of Medical Physiology | Fuster & Hurst's The Heart (15th Ed.) | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.