Csom surgery can be performed if the ear is wet or puss coming out
Reading File
Finding Sources
Searching PubMed
"chronic suppurative otitis media" AND surgery AND "active discharge"
Finding Sources
Searching PubMed
"chronic suppurative otitis media" AND tympanoplasty AND timing
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
I now have enough from the authoritative sources to give a thorough answer. Let me compile it.
Can CSOM Surgery Be Performed When the Ear Is Wet (Discharging)?
This is one of the most frequently asked questions in ear surgery, and the answer is: it depends on the type of surgery and the clinical context. Here is the full picture:
The Traditional Teaching: "Dry Ear" First
The classical principle states that elective tympanoplasty (eardrum repair) should ideally be performed on a dry, non-discharging ear. The rationale is:
- Active infection and mucosal edema reduce graft take rates
- Pus in the middle ear creates a hostile environment for healing
- The operating field is cleaner and better visualized
This is why medical treatment is the first step in managing CSOM without cholesteatoma - topical antibiotic eardrops (ototopical antibiotics) + aural toilet are used to dry up the ear before committing to surgery.
When Surgery IS Done Despite Discharge (Wet Ear)
According to Shambaugh Surgery of the Ear, surgery should be undertaken even with active discharge in these situations:
-
Cholesteatoma is present - cholesteatoma combined with medically refractory CSOM is considered a "nearly absolute indication for surgery" regardless of ear status. You cannot wait indefinitely, as cholesteatoma continues to erode bone.
-
Failed multiple medical treatment attempts - if the ear keeps discharging despite repeated courses of appropriate ototopical antibiotics and aural cleaning, surgery is indicated.
-
Signs of complications are developing:
- Vertigo (suggests labyrinthitis or fistula)
- Facial weakness (suggests facial nerve involvement)
- Headache (suggests intracranial spread)
- These are urgent/emergency indications - you cannot wait for a dry ear.
-
Persistent suppurative drainage with TM perforation - some surgeons consider this an indication for mastoidectomy when tympanoplasty alone has repeatedly failed.
What Happens to Graft Success Rates?
Studies and meta-analyses (cited in Cummings Otolaryngology) show that graft take rates are generally better in a dry ear, but:
- A well-executed tympanoplasty can succeed even with some discharge, particularly if proper intraoperative irrigation and antibiotic coverage are used
- In practice, many experienced surgeons proceed with surgery on a "relatively dry" ear (not actively dripping pus but not perfectly dry) rather than delaying indefinitely
- The contralateral ear status and Eustachian tube function are actually stronger predictors of outcome than whether the ear was dry at the time of surgery
For Cochlear Implantation Specifically
Scott-Brown's Otorhinolaryngology notes that CSOM was previously considered a contraindication to cochlear implantation. The current approach is staged surgery:
- First stage: eradicate disease, wait for the ear to become dry
- Second stage (months later): implant once the ear is stable
Practical Summary Table
| Situation | Operate on wet ear? |
|---|---|
| Tympanoplasty (elective, no cholesteatoma) | Prefer dry ear - treat medically first |
| Cholesteatoma | Yes - cannot delay regardless of discharge |
| Complications (facial palsy, vertigo, intracranial signs) | Yes - emergency/urgent |
| Failed repeated medical treatment | Yes - proceed with surgery |
| Cochlear implantation | Staged approach - dry first, then implant |
Bottom line: For routine tympanoplasty, a wet/discharging ear is not an absolute contraindication but a relative one - you try to dry it medically first. However, when cholesteatoma is present, complications are developing, or medical treatment has repeatedly failed, surgery must proceed even with active discharge.
- Shambaugh Surgery of the Ear, pp. 528-529
- Cummings Otolaryngology Head and Neck Surgery, CSOM and Tympanic Membrane Repair section
- Scott-Brown's Otorhinolaryngology, CSOM and cochlear implantation section
Blood coming out of the ear sometimes
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
I now have enough textbook-grounded information to give a thorough answer. Here it is:
Blood Coming Out of the Ear (Otorrhagia)
Blood from the ear is called otorrhagia and should never be ignored, especially when it occurs intermittently ("sometimes"). The cause can range from trivial to life-threatening. Here is a structured breakdown:
1. Trauma to the Ear Canal (Most Common Cause)
The skin lining the external auditory canal (EAC) is extremely thin and sensitive. Even minor trauma causes bleeding:
- Cotton bud (Q-tip) injury - the single most common cause of blood from the ear
- Foreign body insertion - scratching from an inserted object
- Self-cleaning or scratching - fingernails, hairpins, etc.
- Barotrauma (pressure change during diving/flying) - the EAC skin becomes injected, petechial hemorrhages appear, and frank bleeding may occur
From Scott-Brown's Otorhinolaryngology: "The ear canal skin and tympanic membrane become injected and petechial haemorrhages, and bleeding, may be observed" in ear barotrauma.
Key feature: Stops quickly, small amount, usually one-sided, follows a clear history of trauma or cleaning.
2. Ruptured Tympanic Membrane (Eardrum Perforation)
- Caused by a slap to the ear, explosion blast, sudden pressure change, or a penetrating injury
- Blood comes from the torn edges of the eardrum
- Often accompanied by sudden sharp pain, hearing loss, and ringing (tinnitus)
- If it follows a severe head injury, this is an emergency (see #4 below)
3. Cholesteatoma or Granulation Tissue (in CSOM patients)
- In someone with chronic ear disease (CSOM), blood-stained discharge can come from granulation tissue growing in the middle ear or canal
- Granulation tissue bleeds easily when touched or with aural toilet
- Cholesteatoma eroding blood vessels can also cause bloody discharge
- Blood mixed with pus in a person with known CSOM is a sign the disease is progressing
4. Skull Base / Temporal Bone Fracture (EMERGENCY)
This is the most dangerous cause.
From Cummings Otolaryngology: "Otoscopy often demonstrates a blood-filled canal in patients with facial lacerations who are transported supine. After removal of blood and debris, closer inspection may reveal lacerations in the ear canal in the setting of a skull base fracture."
From Neuroanatomy through Clinical Cases: Hemotympanum is "dark purple blood visible behind the tympanic membrane" - a classic sign of basal skull fracture.
Red flags suggesting fracture:
- Recent head trauma or road accident
- Blood coming from behind the eardrum (dark/maroon colored)
- CSF (clear, watery fluid) mixed with blood
- Bruising behind the ear (Battle's sign)
- Bruising around the eyes (raccoon eyes)
- Facial weakness or dizziness
This is a medical emergency - go to the ER immediately.
5. Glomus Tumor (Paraganglioma) - Important to Recognize
From Cummings Otolaryngology: "Occasionally, either a glomus tympanicum or a glomus jugulare tumor may erode the tympanic membrane and appear as a bleeding mass in the external auditory canal."
Features that suggest this cause:
- Intermittent blood without any injury
- Pulsatile tinnitus (hearing the heartbeat in the ear)
- Conductive hearing loss
- Visible reddish mass behind or through the eardrum on examination
- No prior history of trauma
This is a vascular tumor - never biopsy it in clinic as it can cause life-threatening hemorrhage.
6. Ear Canal Tumors (Less Common)
- Squamous cell carcinoma of the EAC can present with bloodstained discharge, pain, and a mass
- Often mistaken for chronic infection for months before diagnosis
- Should be suspected if discharge is blood-stained, foul-smelling, does not respond to antibiotics, and there is a visible mass in the canal
When to Seek Urgent/Emergency Care
| Symptom | Action |
|---|---|
| Blood after head injury | Emergency room immediately |
| Blood + facial weakness or dizziness | Emergency room immediately |
| Pulsatile (heartbeat-like) blood | Urgent ENT referral (possible glomus tumor) |
| Blood + hearing loss + ear pain | Urgent ENT within days |
| Blood from cotton bud, stops quickly | Can wait - observe |
| Recurrent unexplained blood | ENT appointment needed |
What the Doctor Will Do
- Otoscopy / microscopy to examine the canal and eardrum
- Audiogram (hearing test)
- CT scan of temporal bones if trauma or tumor is suspected
- MRI if glomus tumor or intracranial extension is suspected
The bottom line: Occasional blood from the ear after cleaning or minor trauma is usually benign. But recurrent, unexplained blood - especially with pulsatile tinnitus, hearing loss, or a history of head trauma - requires urgent ENT evaluation. Do not ignore it.
- Cummings Otolaryngology Head and Neck Surgery, Paraganglioma section p. 631-640
- Scott-Brown's Otorhinolaryngology, Ear Barotrauma section
- Neuroanatomy through Clinical Cases, Skull Base Fracture section
I have a hole in ear drum amd some times blood comes from the ear is it normal?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Blood from a Perforated Eardrum - Is It Normal?
No, it is not normal. A simple perforation (hole in the eardrum) on its own does not bleed repeatedly. If you have a known hole in your eardrum and blood keeps coming out - even occasionally - this is a warning sign that needs proper ENT examination. Here is why:
Why a Simple Perforation Does NOT Normally Bleed
Once a perforation is established and healed at its edges, there are no blood vessels at the rim that would bleed spontaneously. Routine discharge from a perforated ear is usually:
- Clear or yellowish (mucus)
- White or cloudy (infected pus)
Blood is different and points to something additional going on.
What Could Be Causing the Blood
1. Granulation Tissue (Most Likely Cause)
When a perforation has been present for a long time with recurrent infections (CSOM), the middle ear lining becomes chronically inflamed and forms granulation tissue - soft, fragile, highly vascular overgrowth. This bleeds very easily with:
- Minor pressure changes
- Coughing, sneezing, nose blowing
- Any discharge flowing past it
This is the most common reason for blood-stained discharge in a person with a perforated eardrum.
2. Aural Polyp - A Very Important Warning Sign
From Shambaugh Surgery of the Ear: "Polyps protruding directly from the middle ear through a tympanic membrane perforation... suggest chronic middle ear disease or cholesteatoma."
A polyp is a fleshy, grape-like growth that can poke out through the hole in the eardrum. It looks harmless but it is not - it almost always means serious underlying disease.
From Cummings Otolaryngology: "An infected cholesteatoma will sometimes present as an 'aural polyp.' These polyps are actually granulation tissue at the junction between an eroding cholesteatoma and bone. The presence of an aural polyp in a chronically infected ear should be considered to be a cholesteatoma until proven otherwise."
This is what a cholesteatoma growing through a perforation can look like:
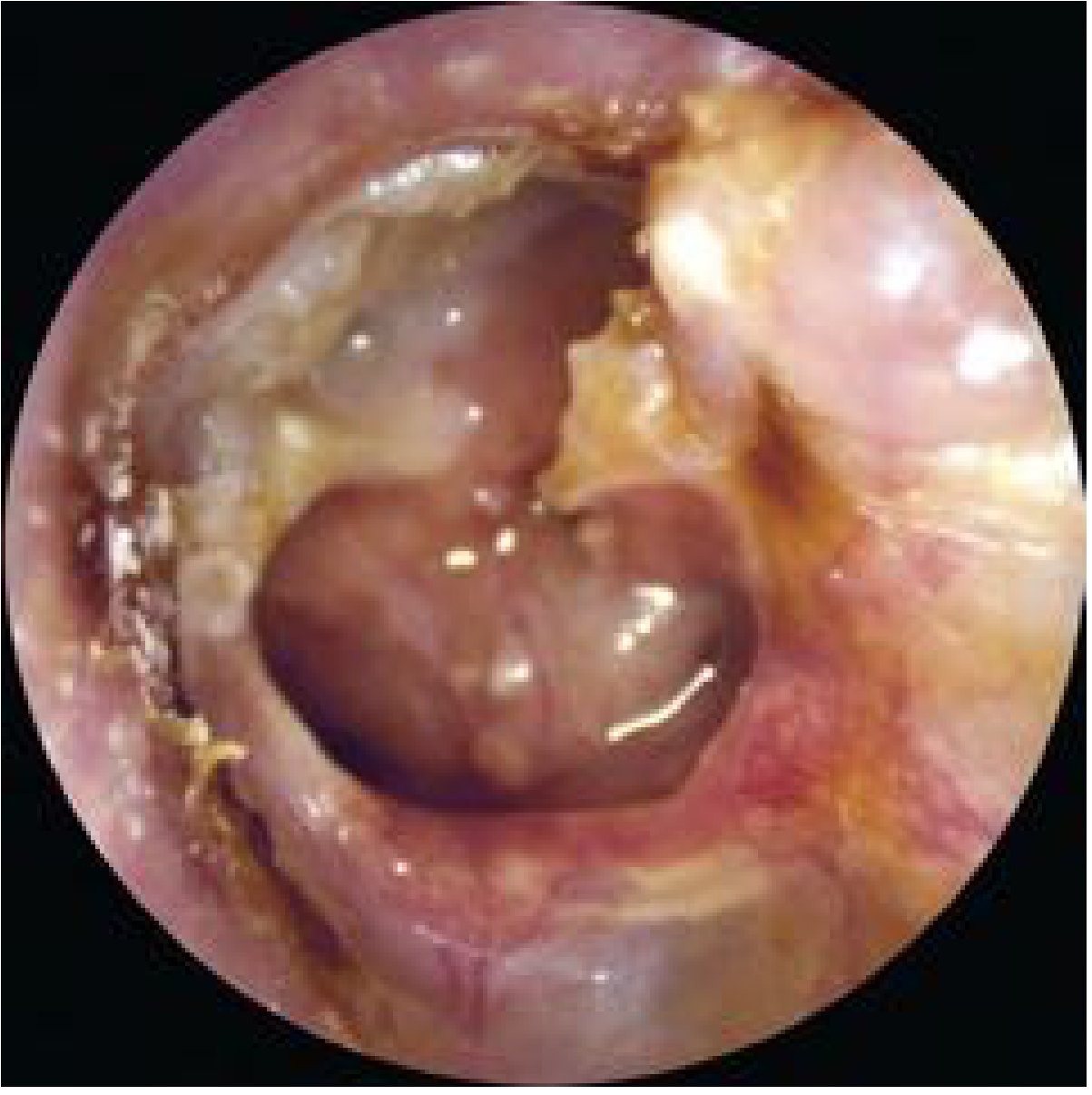
3. Cholesteatoma
Cholesteatoma is a skin-lined sac that grows inside the middle ear and slowly erodes bone. It causes:
- Foul-smelling discharge (due to anaerobic bacteria)
- Blood-stained or blood-mixed discharge
- Hearing loss
- If untreated: facial nerve damage, dizziness, meningitis, brain abscess
This is the most dangerous cause and must be ruled out urgently.
4. Vascular Tumour (Rare but Important)
From Shambaugh Surgery of the Ear: Any mass in the middle ear with a red, blue, or pulsatile appearance must be imaged before any attempt at removal. A glomus tumor (paraganglioma) can bleed heavily if disturbed.
Never let anyone blindly remove a "polyp" from your ear in a clinic without first doing imaging, as it could cause catastrophic bleeding.
Red Flag Symptoms - See an ENT Urgently
| Symptom | What It Suggests |
|---|---|
| Blood + foul/bad smell from ear | Cholesteatoma |
| Blood + pulsatile tinnitus (heartbeat sound) | Glomus tumor |
| Blood + dizziness/vertigo | Labyrinthine erosion by cholesteatoma |
| Blood + facial weakness | Facial nerve involvement |
| Blood + headache | Possible intracranial complication |
| Visible reddish/fleshy lump in ear canal | Aural polyp - needs imaging first |
What You Should Do
- See an ENT specialist - do not delay
- The doctor will perform otomicroscopy (detailed microscopic examination of the ear)
- A CT scan of the temporal bones is likely needed to look for cholesteatoma or bone erosion
- Do not let anyone probe, remove or biopsy anything from your ear without proper imaging first - this is important if a fleshy mass is present
- Do not put cotton buds or anything else in the ear - this aggravates bleeding from granulation tissue
Summary
Blood from a perforated eardrum is not normal and not something to ignore. The most likely causes are granulation tissue or an aural polyp - and importantly, polyps in a perforated ear must be considered cholesteatoma until proven otherwise. Cholesteatoma is a serious condition that erodes bone and causes severe complications if not treated surgically. Please get this seen by an ENT specialist soon.
- Cummings Otolaryngology Head and Neck Surgery, Cholesteatoma Diagnosis, p. 2684
- Shambaugh Surgery of the Ear, External Auditory Canal and Tubotympanic Disease sections
This is a shared conversation. Sign in to Orris to start your own chat.