Explain circle of wills for my anatomy test tomorrow as a 5 marker question
Circle of Willis - 5 Mark Answer
Definition & Location
Components - "AAPIPP" (Mnemonic)
| Component | Origin | Role in Circle |
|---|---|---|
| Anterior communicating artery (AComm) | Connects both ACAs | Anterior crosslink |
| Anterior cerebral arteries x2 (ACA) | Terminal ICA | Anterior part of circle |
| Internal carotid arteries x2 (ICA) | Common carotid | Lateral supply |
| Posterior communicating arteries x2 (PComm) | ICA → PCA | Anterior-posterior link |
| Posterior cerebral arteries x2 (PCA) | Top of basilar artery | Posterior part of circle |
Diagram
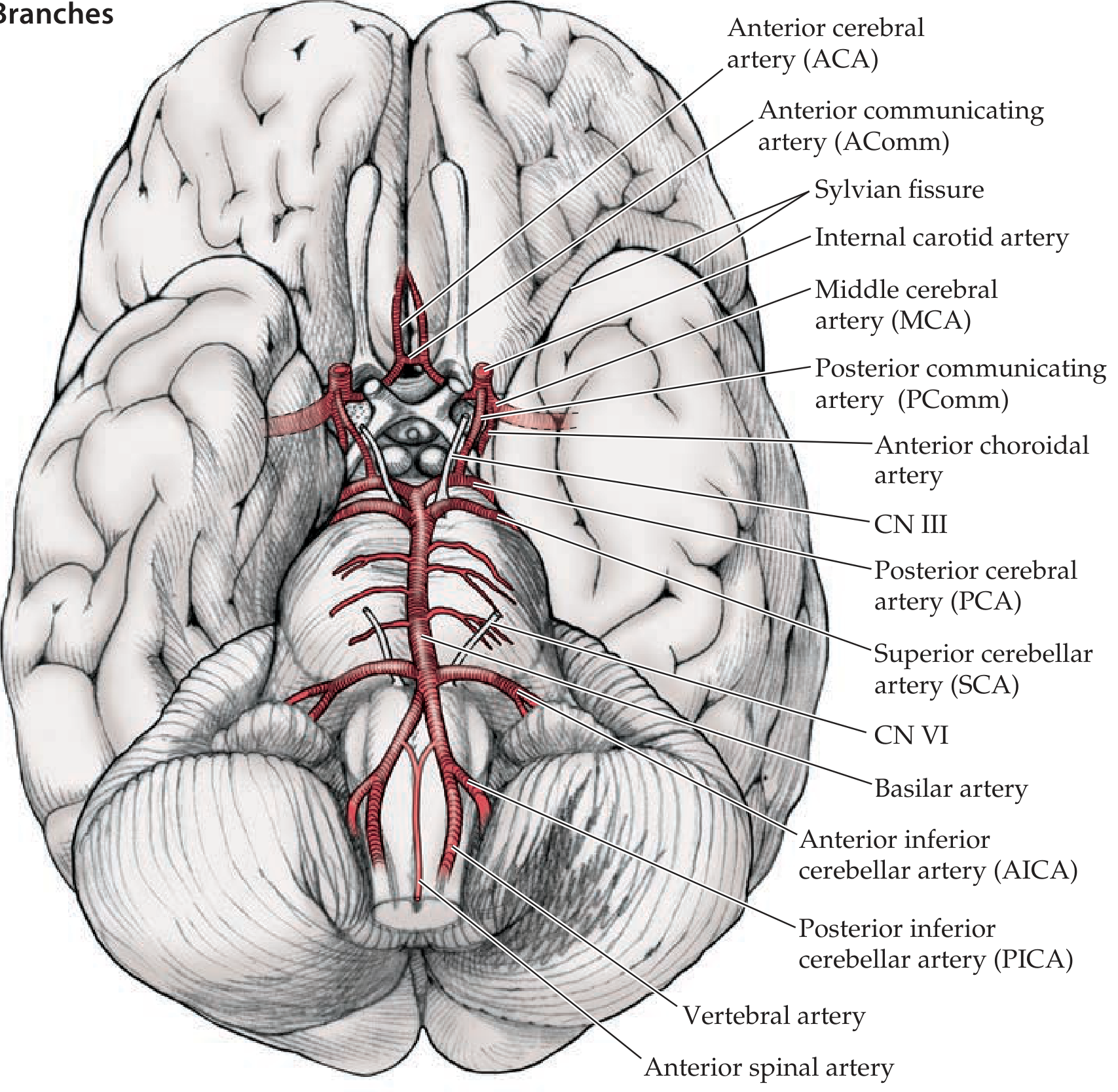
Blood Supply to Cerebral Hemispheres
- ACA - medial surfaces of the frontal and parietal lobes
- MCA (middle cerebral artery) - lateral surfaces, including motor/speech areas; arises from the ICA just outside the circle
- PCA - occipital and inferior temporal lobes
Functional Significance (Clinical Importance)
-
Collateral circulation - If one vessel is blocked (e.g. ICA stenosis), blood can reroute through the communicating arteries to maintain perfusion. A complete, full-caliber circle is present in only ~34% of individuals, so collateral protection is variable.
-
Berry (saccular) aneurysms - The bifurcation points of the circle are the most common sites for intracranial aneurysms. The AComm artery is the single most common site. Rupture causes subarachnoid hemorrhage.
-
Stroke territory - Occlusion of specific vessels produces predictable deficits based on which territory is deprived (e.g. MCA stroke = contralateral hemiplegia + aphasia).
Key Points to Remember for Exam
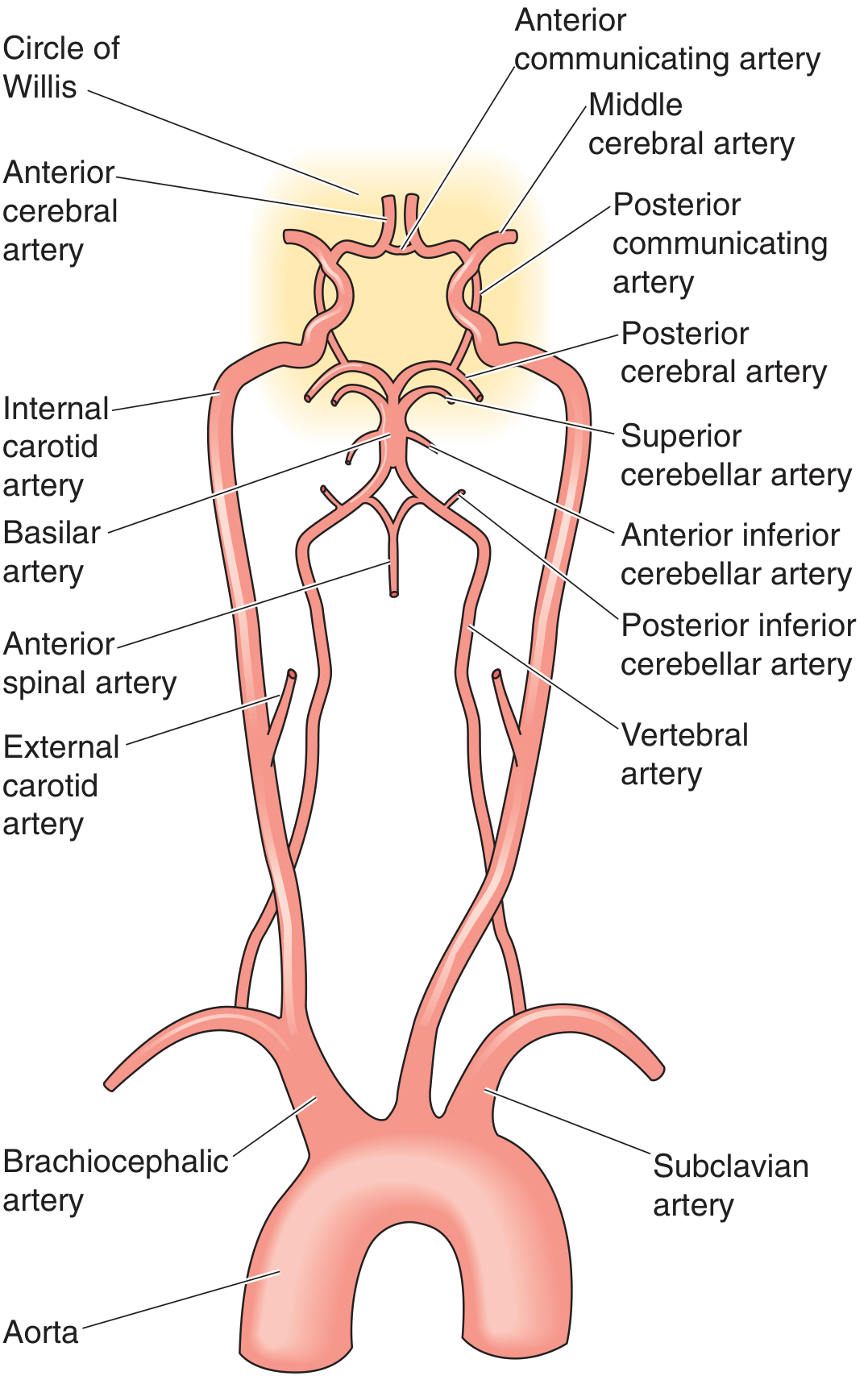
- Circle of Willis = anastomotic ring at base of brain connecting ICA system + vertebrobasilar system
- 7 vessels form the ring: 2 ACAs + AComm + 2 ICAs + 2 PComms + 2 PCAs (the ICAs and PCAs are bilateral)
- The AComm links the two anterior circulations; the PComms link anterior to posterior
- A complete circle exists in only ~34% of people (variants are very common)
- Common sites for berry aneurysms: AComm > PComm > MCA bifurcation
Give me a well labeled diagram of spermatogenesis
Spermatogenesis - Well-Labeled Diagrams
Diagram 1 - Stages of Spermatogenesis within the Seminiferous Tubule
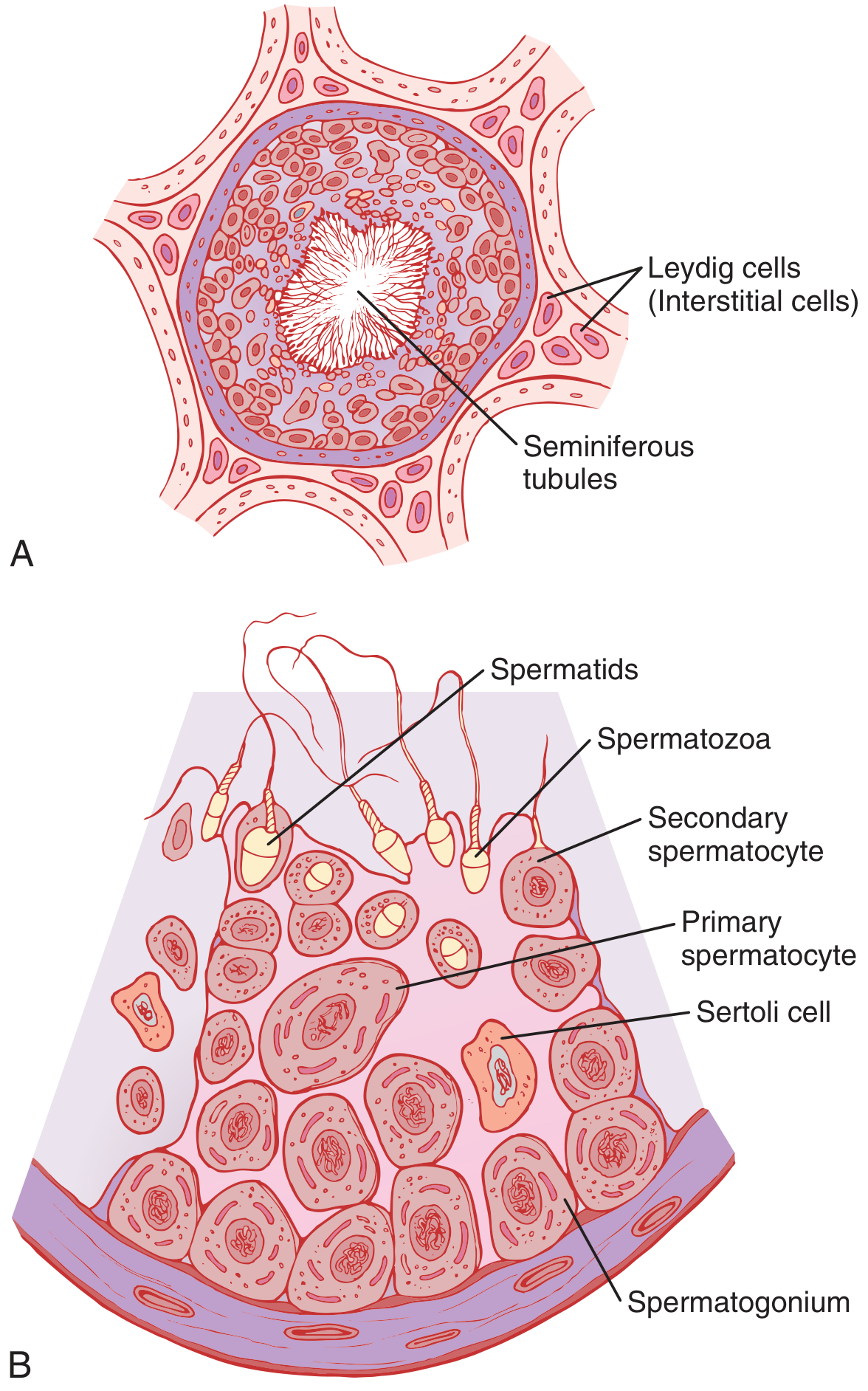
- Spermatogonium (base/basal lamina) - diploid (2n), 46 chromosomes; the stem cell
- Primary spermatocyte - largest germ cell; undergoes Meiosis I
- Secondary spermatocyte - haploid (n), 23 chromosomes; undergoes Meiosis II
- Spermatids - haploid; rounded cells that undergo spermiogenesis
- Spermatozoa - mature sperm released into tubule lumen
Diagram 2 - Detailed Histology of the Seminiferous Epithelium
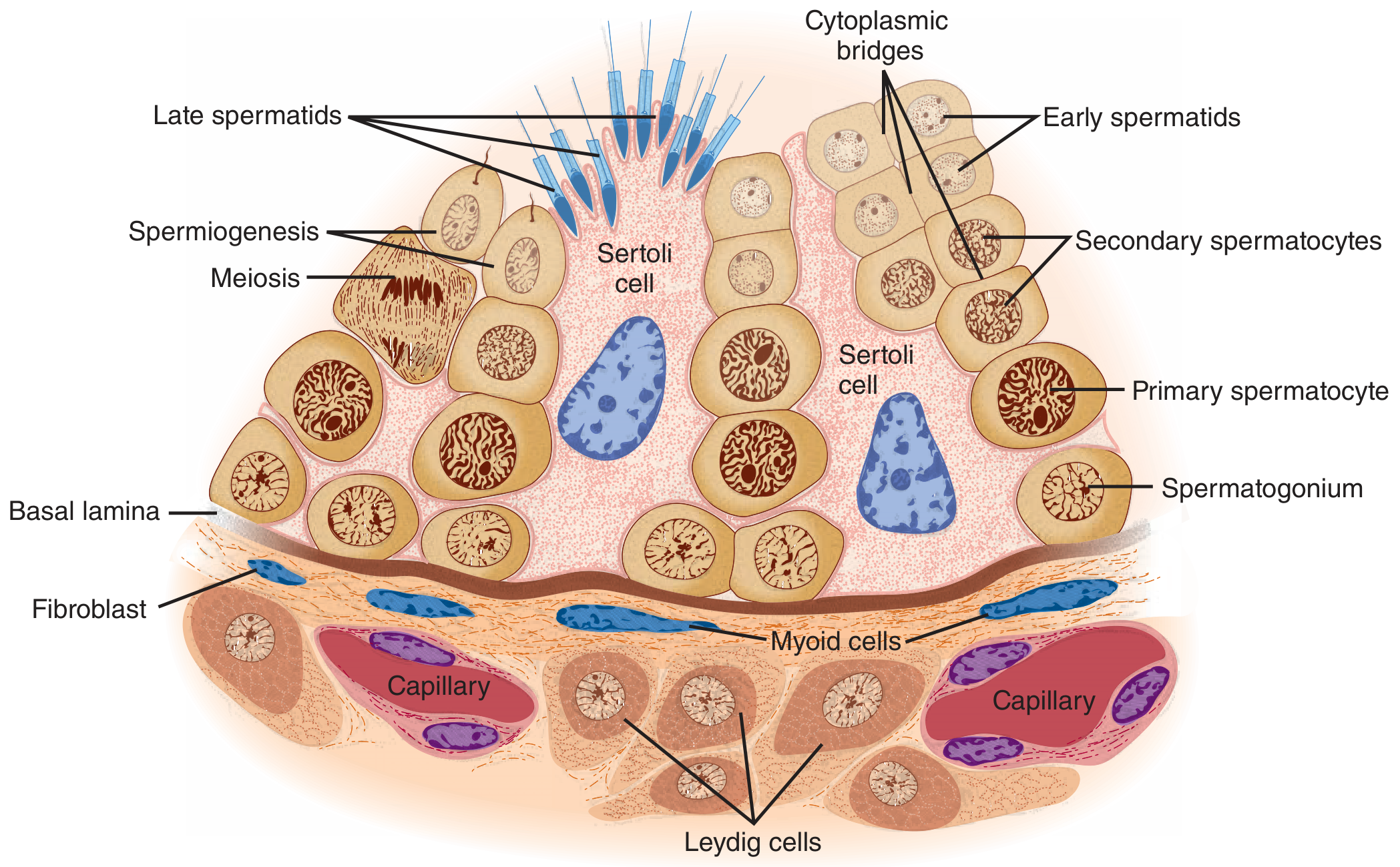
| Structure | Location | Function |
|---|---|---|
| Spermatogonium | Basal lamina | Stem cell; mitotic divisions |
| Primary spermatocyte | Inner layer | Meiosis I (longest stage) |
| Secondary spermatocyte | Mid layer | Meiosis II |
| Early spermatids | Near lumen | Post-meiosis, rounded |
| Late spermatids | Near lumen | Elongating during spermiogenesis |
| Sertoli cells | Full height (blue cells) | Nurse cells; secrete ABP, inhibin, MIS |
| Leydig cells | Interstitium (outside) | Produce testosterone |
| Cytoplasmic bridges | Between spermatids | Synchronize differentiation of a clone |
| Basal lamina | Outer wall | Structural boundary |
| Myoid cells | Surrounding tubule | Contractile peristalsis |
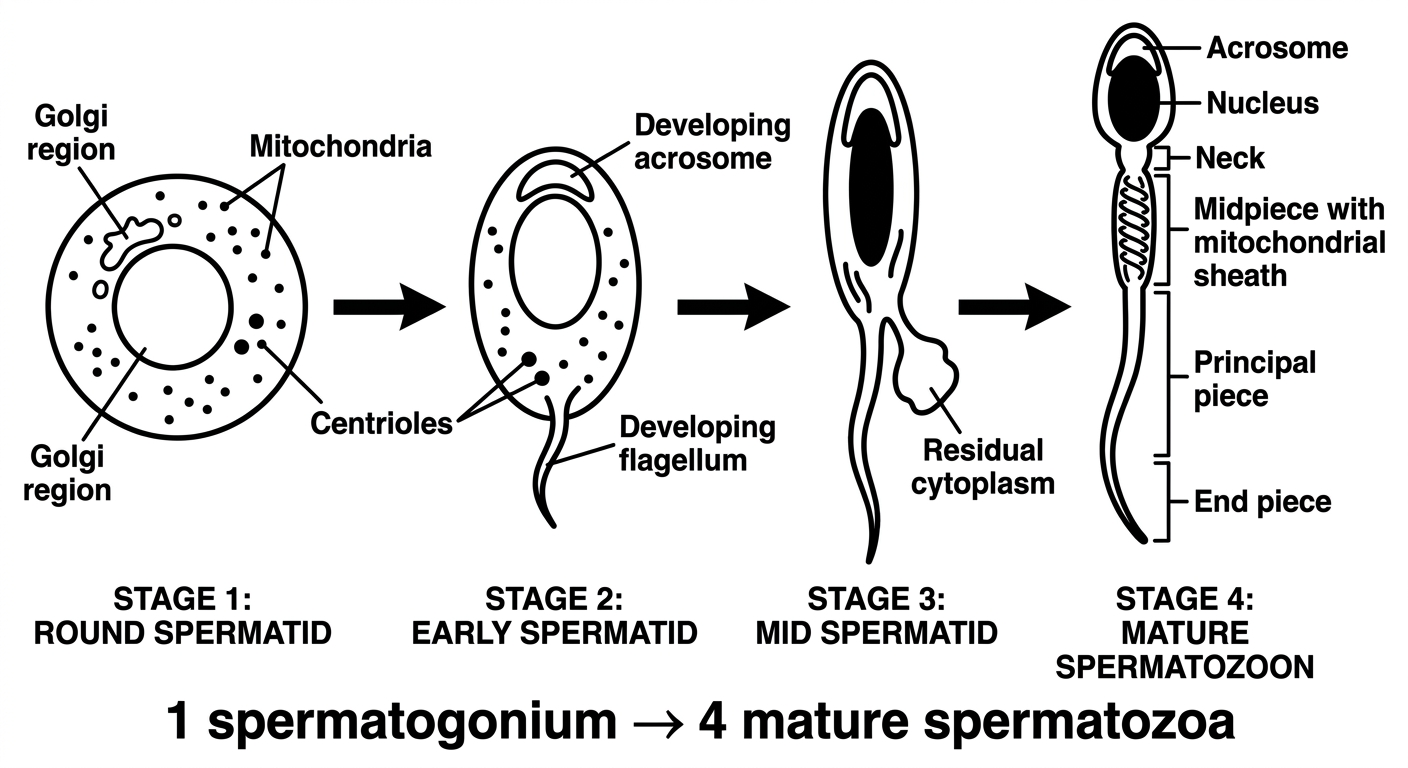
Diagram 3 - Spermiogenesis (Spermatid → Spermatozoon)
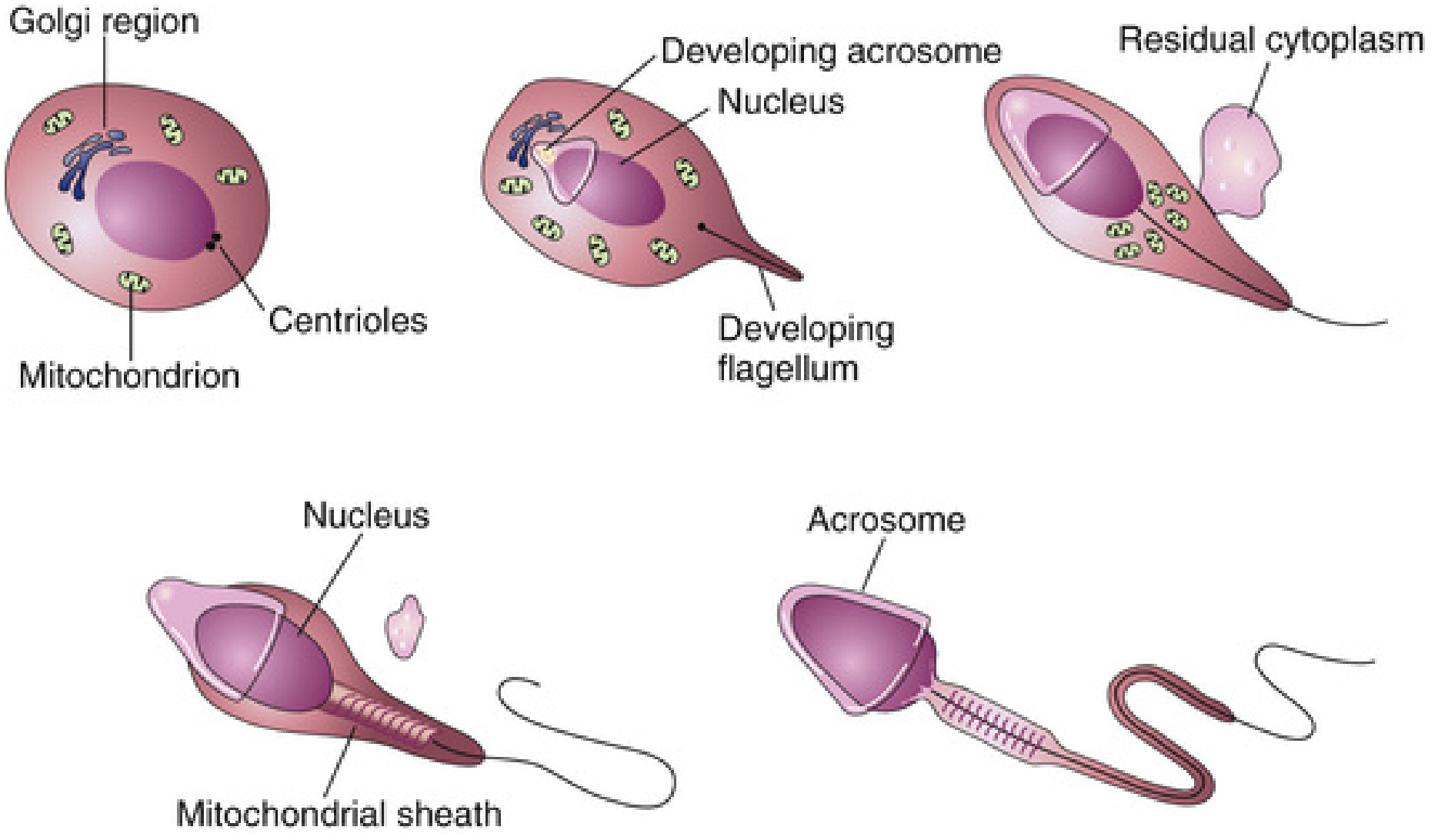
- Round spermatid - Golgi region, centrioles, mitochondria visible
- Acrosome formation - Golgi forms acrosome cap over nucleus
- Flagellum development - centrioles form the axoneme (tail)
- Elongation - cytoplasm shed as residual body; mitochondria wrap around midpiece → mitochondrial sheath
- Mature spermatozoon - acrosome capping the head + flagellum complete
Summary Flow Chart
Spermatogonium (2n, 46 chr)
↓ Mitosis (proliferation)
Primary Spermatocyte (2n, 46 chr)
↓ Meiosis I [REDUCTION DIVISION]
Secondary Spermatocyte (n, 23 chr) × 2
↓ Meiosis II [EQUATORIAL DIVISION]
Spermatids (n, 23 chr) × 4
↓ Spermiogenesis (no division - just morphological change)
Spermatozoa (n, 23 chr) × 4
- 1 spermatogonium → 4 functional spermatozoa (vs. oogenesis which gives only 1 ovum)
- Total duration: ~74 days (Ganong) / ~2 months (Moore)
- Begins at puberty (~age 13); regulated by FSH (maintains spermatogenesis) and LH (stimulates Leydig cells → testosterone)
- Testosterone acts via androgen receptors on Sertoli cells, not directly on germ cells
Make drawable images
Clean simple black and white line drawing diagram of spermatogenesis stages, suitable for medical students to copy by hand. Show a vertical flow chart with clearly labeled cells from top to bottom: Spermatogonium (large round cell with nucleus, labeled "2n 46 chromosomes") → arrow labeled "Mitosis" → Primary Spermatocyte (large cell, labeled "2n 46 chromosomes") → arrow labeled "Meiosis I (First meiotic division)" → two Secondary Spermatocytes (medium cells, labeled "n 23 chromosomes") → arrow labeled "Meiosis II (Second meiotic division)" → four Spermatids (small round cells, labeled "n 23 chromosomes") → arrow labeled "Spermiogenesis" → four Spermatozoa (sperm cells with head and tail). Each cell drawn as a simple circle with a nucleus inside. Bold clear labels on every cell and every arrow. Simple clean educational style, white background, black lines only, no shading, no color.
Clean simple black and white line drawing diagram of spermiogenesis for medical students to copy by hand. Show 4 stages in a horizontal row with arrows between them, all clearly labeled. Stage 1: Round spermatid - circle with large nucleus and small Golgi vesicle labeled "Golgi region" and dots labeled "Mitochondria" and two small dots labeled "Centrioles". Stage 2: Early spermatid - oval shape, nucleus condensing, small cap forming labeled "Developing acrosome", a short tail labeled "Developing flagellum". Stage 3: Mid spermatid - elongated, nucleus condensed and darkened, acrosome covering anterior nucleus, longer tail, cytoplasm shrinking, blob labeled "Residual cytoplasm". Stage 4: Mature spermatozoon - fully elongated sperm, labeled parts: "Acrosome" (cap on head), "Nucleus" (in head), "Neck", "Midpiece with mitochondrial sheath", "Principal piece", "End piece" (tail). Below the diagram write: "1 spermatogonium → 4 mature spermatozoa". Bold black labels, white background, simple clean educational line art, no color, no shading.
Diagram 1 - Spermatogenesis Stages (Full Flow)
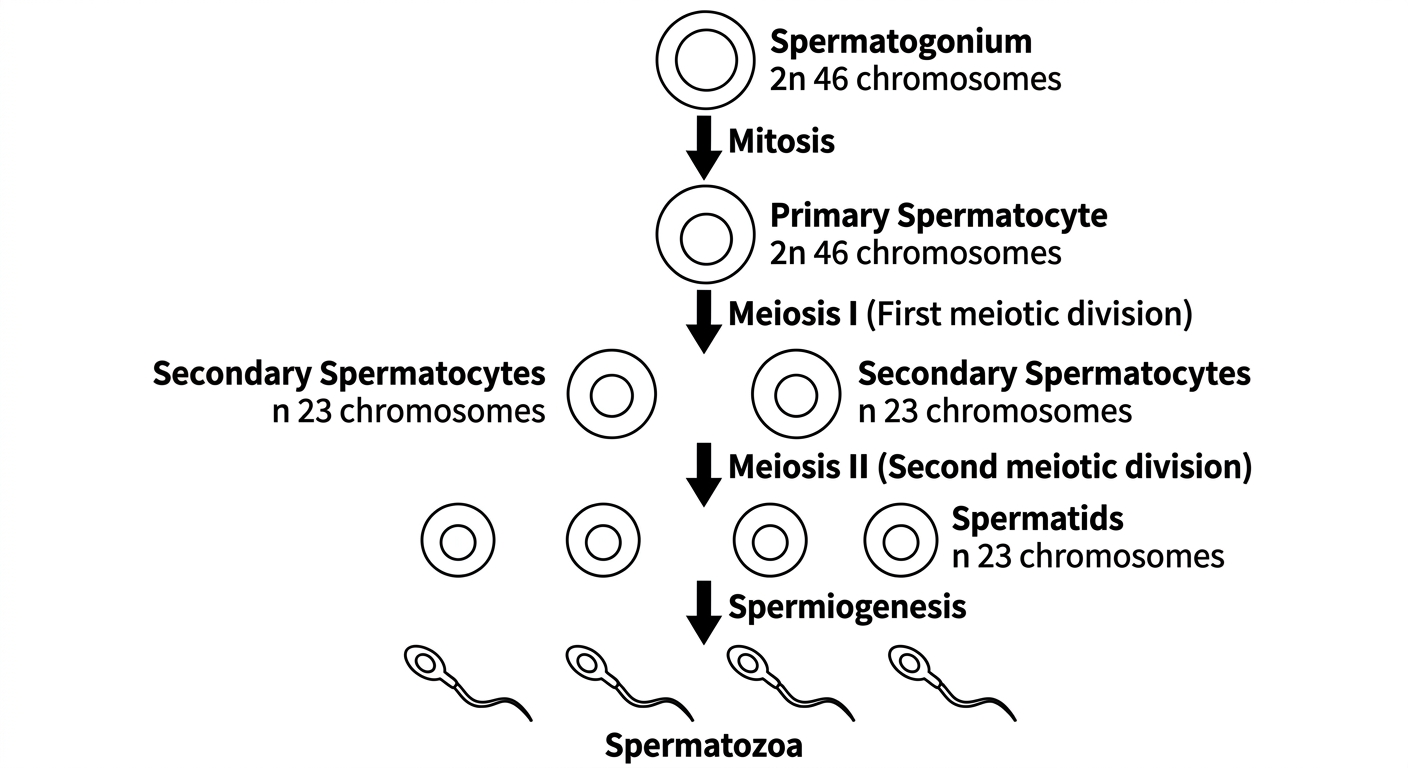
Diagram 2 - Spermiogenesis (Spermatid → Mature Sperm)
- Diagram 1 - Draw circles getting progressively smaller from top to bottom. Use brackets to show where meiosis I gives 2 cells and meiosis II gives 4 cells.
- Diagram 2 - Draw 4 stages left to right: round cell → elongating → losing cytoplasm → final sperm shape. The acrosome is always at the front of the head (like a helmet/cap).
- Always label ploidy: 2n for spermatogonium and primary spermatocyte, n from secondary spermatocyte onward.
Explain csf circulation for my anat exam tomorrow as a 5 marker
CSF Circulation - 5 Mark Answer
Diagram
1. Production
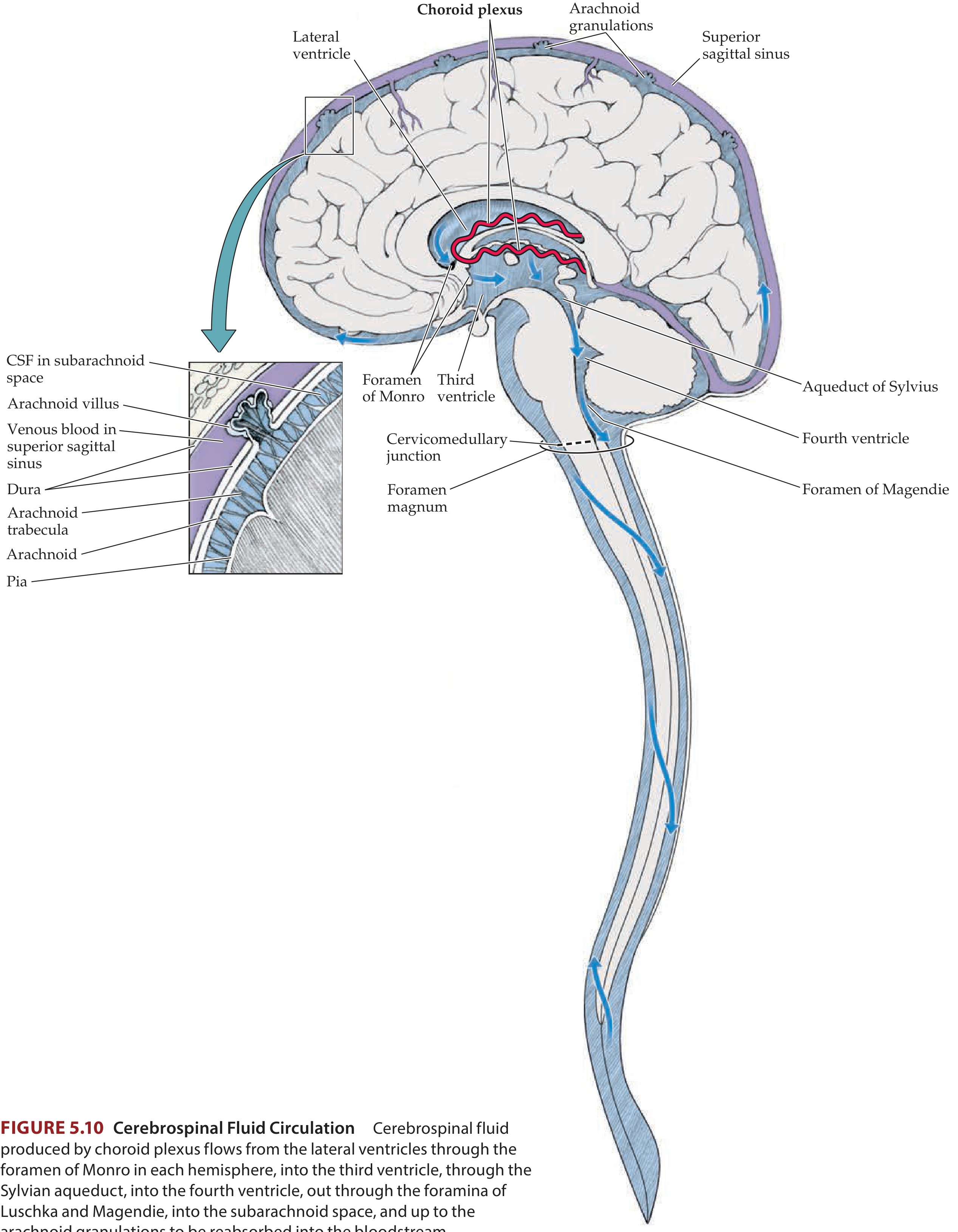
2. Circulation Pathway (Follow the Flow)
Lateral ventricles (choroid plexus produces CSF)
↓ Interventricular foramen of Monro (×2)
Third ventricle
↓ Cerebral aqueduct (Aqueduct of Sylvius) — through the midbrain
Fourth ventricle
↓ Three foramina exit the ventricular system:
• Foramen of Magendie (median, in roof of 4th ventricle)
• Foramina of Luschka (×2, lateral apertures of 4th ventricle)
Subarachnoid space (bathes brain + spinal cord)
↓ Fills cisterns (cisterna magna, interpeduncular cistern, etc.)
↓ Flows upward over cerebral convexities
Arachnoid granulations (villi) projecting into superior sagittal sinus
↓ Absorption into venous blood (one-way pressure-dependent valve)
Superior sagittal sinus → internal jugular vein → systemic circulation
3. Key Foramina - Must Know
| Foramen | Location | Connects |
|---|---|---|
| Foramen of Monro (interventricular) | Between lateral & 3rd ventricle | Lateral → 3rd ventricle |
| Aqueduct of Sylvius (cerebral aqueduct) | Through midbrain | 3rd → 4th ventricle |
| Foramen of Magendie (median aperture) | Roof of 4th ventricle | 4th ventricle → subarachnoid |
| Foramina of Luschka (lateral apertures ×2) | Lateral recesses of 4th ventricle | 4th ventricle → subarachnoid |
4. Absorption
5. Functions of CSF
- Mechanical protection - cushions the brain against trauma (buoyancy reduces effective brain weight from ~1400g to ~25g)
- Waste removal - removes metabolic waste products from the CNS
- Chemical stability - maintains a stable ionic environment for neurons
- Nutrient transport - delivers glucose and other nutrients to brain tissue
Clinical Relevance - Hydrocephalus
- Obstructive (non-communicating) - blockage within the ventricular system (e.g. at aqueduct of Sylvius - most common site)
- Communicating - impaired absorption at arachnoid granulations (e.g. after meningitis or subarachnoid haemorrhage); all ventricles dilate
Mnemonic for flow: "Little Monkeys Are Mighty Lovable Superstars" = Lateral ventricles → foramen of Monro → third ventricle → Aqueduct of Sylvius → fourth ventricle → foramina of Magendie/Luschka → Subarachnoid space → arachnoid granulations
Explain floor of 4 ventricle with drawable diagram
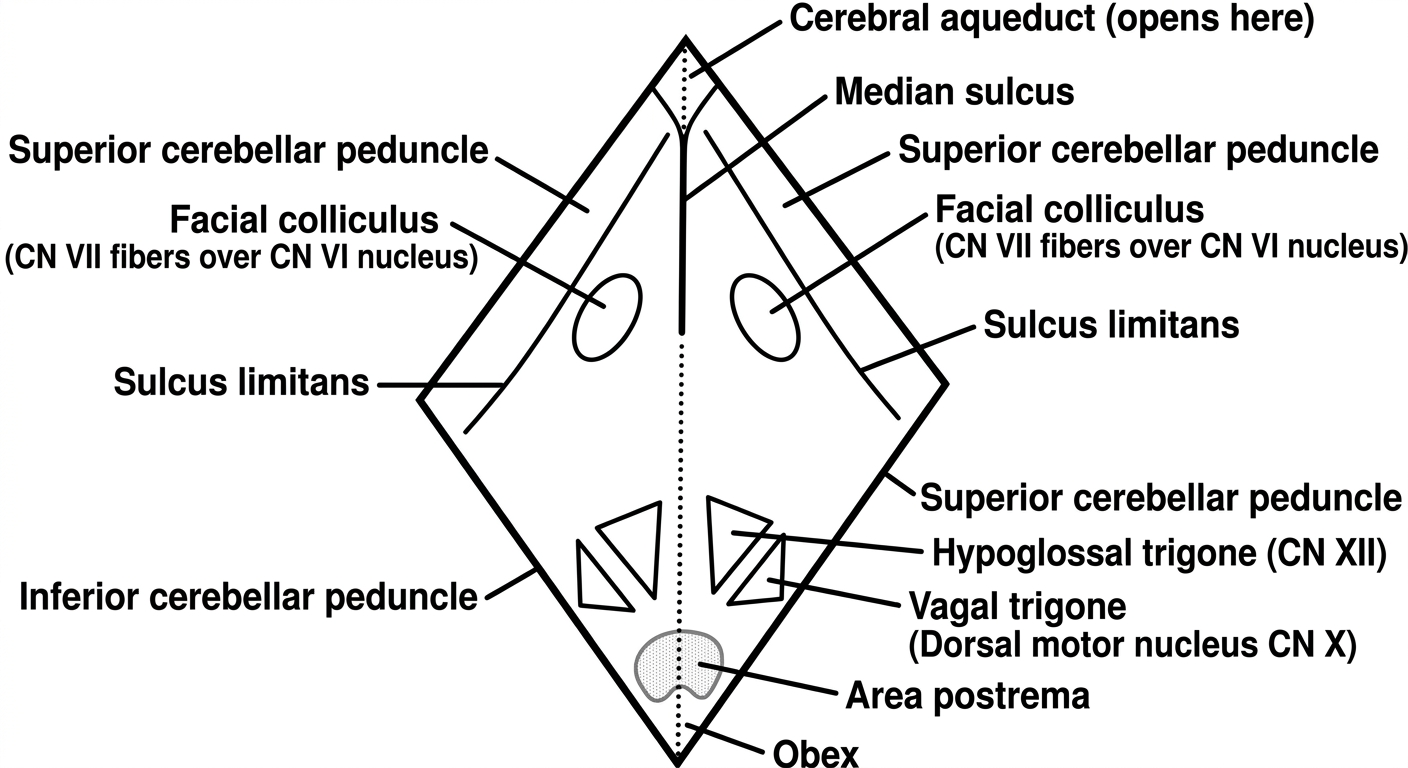
Clean simple black and white line drawing diagram of the floor of the fourth ventricle (rhomboid fossa) as seen from above (dorsal view), for medical students to copy by hand. Draw a diamond/rhombus shape representing the floor. Label all the following structures clearly with leader lines: At the top point: "Cerebral aqueduct (opens here)". On the upper half (pontine part): a central vertical groove labeled "Median sulcus", two oval bumps on either side labeled "Facial colliculus (CN VII fibers over CN VI nucleus)", a diagonal groove on each side labeled "Sulcus limitans". On the lower half (medullary part): two small triangles labeled "Hypoglossal trigone (CN XII)" medially and "Vagal trigone (Dorsal motor nucleus CN X)" laterally, a small grey area at bottom labeled "Area postrema", a rounded structure at the very bottom point labeled "Obex". Along the lateral sides of the rhombus label: "Superior cerebellar peduncle" (upper lateral), "Inferior cerebellar peduncle" (lower lateral). Draw a dotted midline. White background, black lines only, bold clear labels, educational medical style, no color, no shading.
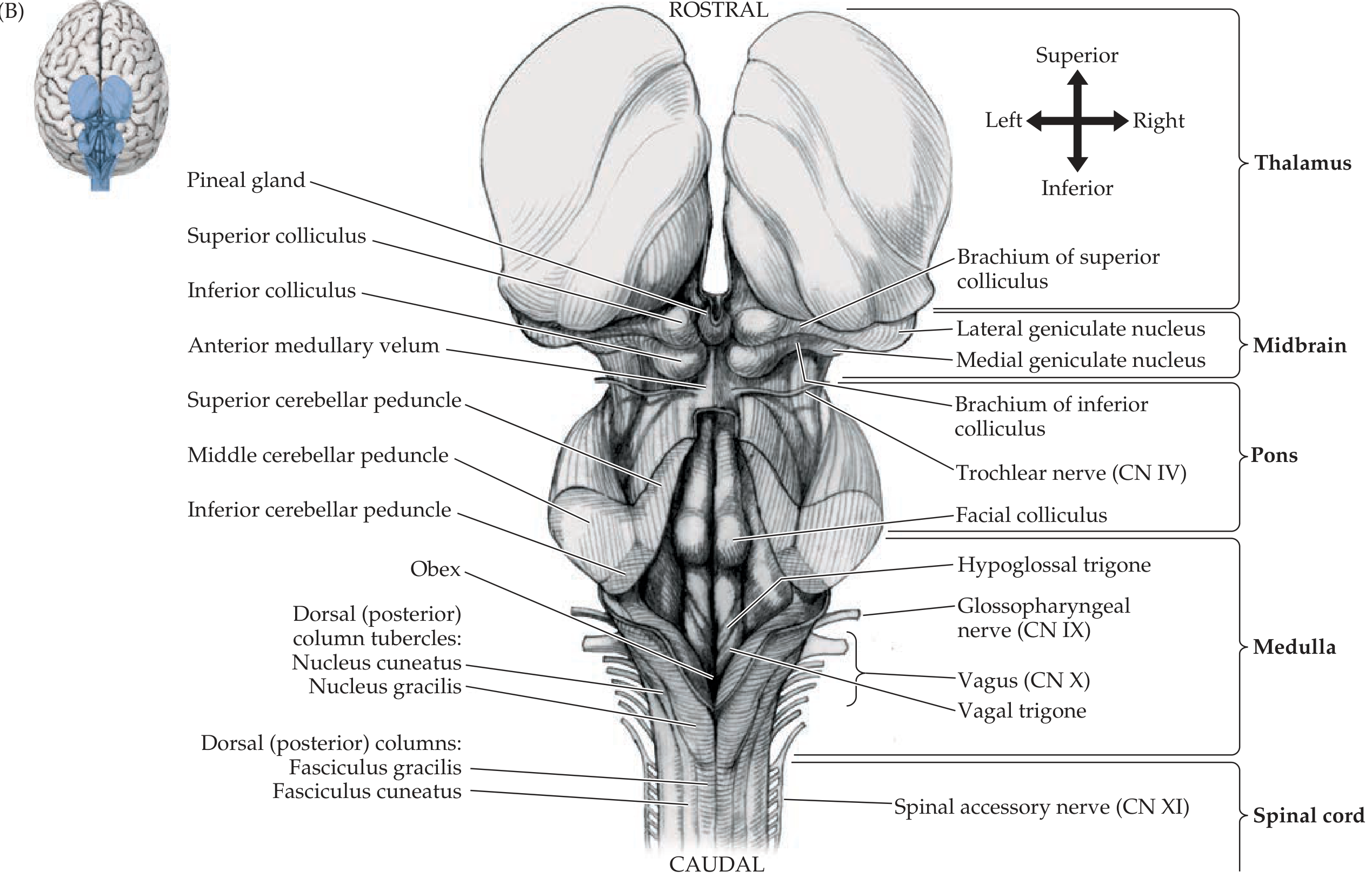
Floor of the Fourth Ventricle
Textbook Diagram - Dorsal View of Brainstem (Cerebellum Removed)
Drawable Diagram - Floor of Fourth Ventricle (Rhomboid Fossa, from above)
Shape & Boundaries
- Upper half (rostral) - dorsal surface of the pons
- Lower half (caudal) - dorsal surface of the rostral medulla
- Superior cerebellar peduncle (upper lateral border)
- Middle cerebellar peduncle
- Inferior cerebellar peduncle (lower lateral border)
Key Features - From Rostral to Caudal
Sulci (Grooves)
| Structure | Position | Significance |
|---|---|---|
| Median sulcus | Runs vertically along midline | Divides floor into two symmetric halves |
| Sulcus limitans | Diagonal groove on each side of median sulcus | Separates motor (medial) from sensory (lateral) cranial nerve nuclei - equivalent to the embryonic alar/basal plate boundary |
Elevations (Bumps)
| Structure | Location | What lies underneath |
|---|---|---|
| Facial colliculus | Upper pons, just lateral to median sulcus | CN VI (abducens) nucleus + looping fibres of CN VII (facial nerve genu) wrap around it |
| Hypoglossal trigone | Lower medulla, medial | CN XII (hypoglossal nucleus) |
| Vagal trigone | Lower medulla, lateral to hypoglossal trigone | Dorsal motor nucleus of CN X (vagus) |
| Area postrema | At the caudal tip, near obex | Chemoreceptor trigger zone (CTZ); no blood-brain barrier; detects emetics in blood |
Caudal End
- Obex - the most caudal point of the 4th ventricle where it narrows to become the central canal of the spinal cord (normally closed in adults)
Important Relations
ROSTRAL TIP
↑ Opens into Cerebral Aqueduct (Aqueduct of Sylvius)
UPPER HALF = PONTINE PART
Facial colliculus (CN VI nucleus + CN VII genu)
Median sulcus (midline groove)
Sulcus limitans (diagonal)
LOWER HALF = MEDULLARY PART
Hypoglossal trigone (CN XII) ← medial
Vagal trigone (CN X DMN) ← lateral
Area postrema (CTZ)
CAUDAL TIP
Obex → narrows to central canal
Clinical Points
- Facial colliculus lesion - damages both CN VI (lateral gaze palsy) AND CN VII (ipsilateral facial weakness) simultaneously - a classic localising sign to the pons
- Area postrema - the vomiting centre; stimulated by toxins, opioids, chemotherapy drugs (it lacks the blood-brain barrier)
- Wernicke's encephalopathy (thiamine deficiency) - causes haemorrhagic lesions in the floor of the 4th ventricle, particularly in the periaqueductal grey and around the floor structures, causing ophthalmoplegia, ataxia, and confusion
Mnemonic for medullary structures medial → lateral:
"Hypnotised Vagrants Avoid Problems" = Hypoglossal trigone → Vagal trigone → Area postrema
Transverse section of the Medulla (at the level of sensory decussation or the olive). As 5 marker answer
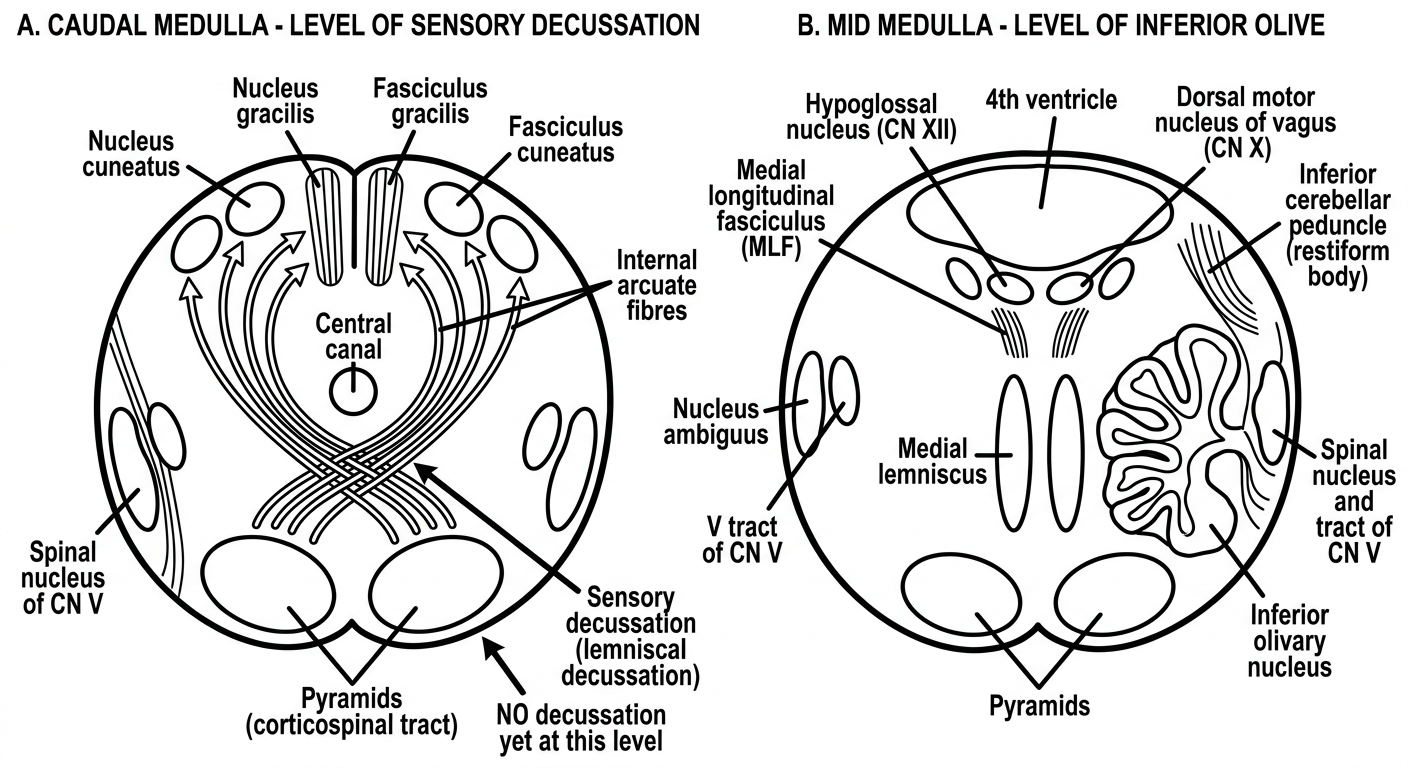
Clean simple black and white line drawing diagram showing TWO transverse sections of the medulla oblongata side by side for medical students to copy by hand. White background, black lines only, no shading, bold clear labels. LEFT DIAGRAM labeled at top: "A. Caudal Medulla - Level of Sensory Decussation" Draw an oval cross section. Label these structures with leader lines: - DORSAL side (top): "Nucleus gracilis" (medial, paired oval), "Nucleus cuneatus" (lateral, paired oval), "Fasciculus gracilis", "Fasciculus cuneatus" - MIDDLE crossing the midline: curved arrows showing "Internal arcuate fibres" sweeping from dorsal nuclei toward midline, labeled "Sensory decussation (lemniscal decussation)" at midline - VENTRAL (bottom): two oval bumps labeled "Pyramids (corticospinal tract)" - note "NO decussation yet at this level" - LATERAL: "Spinal nucleus of CN V", "Spinal tract of CN V" - Central canal labeled in middle RIGHT DIAGRAM labeled at top: "B. Mid Medulla - Level of Inferior Olive" Draw an oval cross section. Label: - DORSAL (top): "4th ventricle" (open space at top), "Hypoglossal nucleus (CN XII)" medially, "Dorsal motor nucleus of vagus (CN X)" laterally, "Medial longitudinal fasciculus (MLF)" - MIDDLE: "Medial lemniscus" (paired vertical ovals near midline), "Nucleus ambiguus" laterally, "Inferior olivary nucleus" (large folded structure, like a crumpled bag) - LATERAL: "Spinal nucleus and tract of CN V", "Inferior cerebellar peduncle (restiform body)" - VENTRAL: "Pyramids" (two oval bumps at bottom) Educational clean style, all structures clearly labeled.
Transverse Section of the Medulla - 5 Mark Answer
Drawable Diagram
Textbook Cross-Section - Level of the Inferior Olive (Mid Medulla)

A. Level of Sensory Decussation (Caudal Medulla)
Structures - Organized by Region
| Structure | Position | What it carries |
|---|---|---|
| Nucleus gracilis | Dorsal midline (medial) | Relay for vibration/proprioception from lower limbs |
| Nucleus cuneatus | Dorsolateral (lateral to gracilis) | Relay for vibration/proprioception from upper limbs |
| Fasciculus gracilis | Dorsomedial white matter | Ascending posterior column fibres, lower limb |
| Fasciculus cuneatus | Dorsolateral white matter | Ascending posterior column fibres, upper limb |
- 2nd order neurones from nucleus gracilis and cuneatus give off internal arcuate fibres
- These sweep anteriorly around the central grey and cross the midline = Sensory Decussation (Lemniscal decussation)
- After crossing, they form the medial lemniscus which ascends on the opposite side
- This is why a lesion ABOVE this level → contralateral loss of vibration/proprioception
- Spinal nucleus of CN V - relays pain/temperature from face
- Spinal tract of CN V - descending fibres of trigeminal nerve
- Pyramids - two rounded bulges at the ventral midline containing corticospinal tract fibres
- Note: at the very caudal end, 75-90% of pyramidal fibres cross = Pyramidal (Motor) decussation → forms lateral corticospinal tract
B. Level of the Inferior Olive (Mid/Rostral Medulla)
Structures - Organized by Region
- Hypoglossal nucleus (CN XII) - medial, under hypoglossal trigone; tongue movement
- Dorsal motor nucleus of CN X - lateral to hypoglossal; parasympathetics to thoracoabdominal viscera
- Nucleus solitarius (tractus solitarius) - ventrolateral to dorsal X nucleus; taste (VII, IX, X) and visceral afferents
- Medial longitudinal fasciculus (MLF) - coordinates eye movements; just under the floor of 4th ventricle near midline
- Medial lemniscus - paired vertical tracts running close to midline, carrying contralateral proprioception/vibration toward thalamus
- Nucleus ambiguus - branchial motor nucleus for CN IX, X (pharyngeal/laryngeal muscles - swallowing, voice)
- Spinal nucleus and tract of CN V - pain/temperature from face
- Inferior cerebellar peduncle (Restiform body) - connects medulla to cerebellum
- Vestibular nuclei - for balance/eye movement coordination (CN VIII)
- Inferior olivary nucleus - large folded/crumpled bag-shaped nucleus; the major relay in the cerebellar circuit (sends olivocerebellar fibres through inferior cerebellar peduncle)
- Pyramids - corticospinal tract, two oval bulges at anteromedian groove
Summary Table
| Structure | Location in Section | Clinical Relevance |
|---|---|---|
| Nucleus gracilis/cuneatus | Dorsal | Source of internal arcuate fibres |
| Internal arcuate fibres | Sweeping to midline | Sensory decussation - cross here |
| Medial lemniscus | Paramedian | Carries contralateral proprioception |
| Pyramids | Ventral | Corticospinal tract |
| Inferior olivary nucleus | Ventrolateral | Cerebellar relay - Wallenberg spares it |
| Hypoglossal nucleus (XII) | Dorsomedial | Tongue palsy in medial medullary syndrome |
| Nucleus ambiguus | Lateral tegmentum | Dysphagia/dysphonia in lateral medullary syndrome |
| Spinal V nucleus/tract | Lateral | Ipsilateral facial pain/temp loss |
Clinical Correlation - The Two Medullary Syndromes
- Pyramid → contralateral hemiplegia
- Medial lemniscus → contralateral loss of proprioception/vibration
- CN XII nucleus/fibres → ipsilateral tongue weakness (deviation toward lesion)
- Nucleus ambiguus → ipsilateral dysphagia, dysphonia (IX, X)
- Spinal V nucleus → ipsilateral facial pain/temp loss
- Spinothalamic tract → contralateral body pain/temp loss
- Inferior cerebellar peduncle → ipsilateral ataxia
- Descending sympathetics → ipsilateral Horner's syndrome
Memory aid for olive-level structures (ventral → dorsal): "Pyramids Make Large Nuclei Hate Dullness" = Pyramids → Medial lemniscus → Lateral inferior Olive → Nucleus ambiguus → Hypoglossal nucleus → Dorsal motor X nucleus
Internal capsule drawable diagram
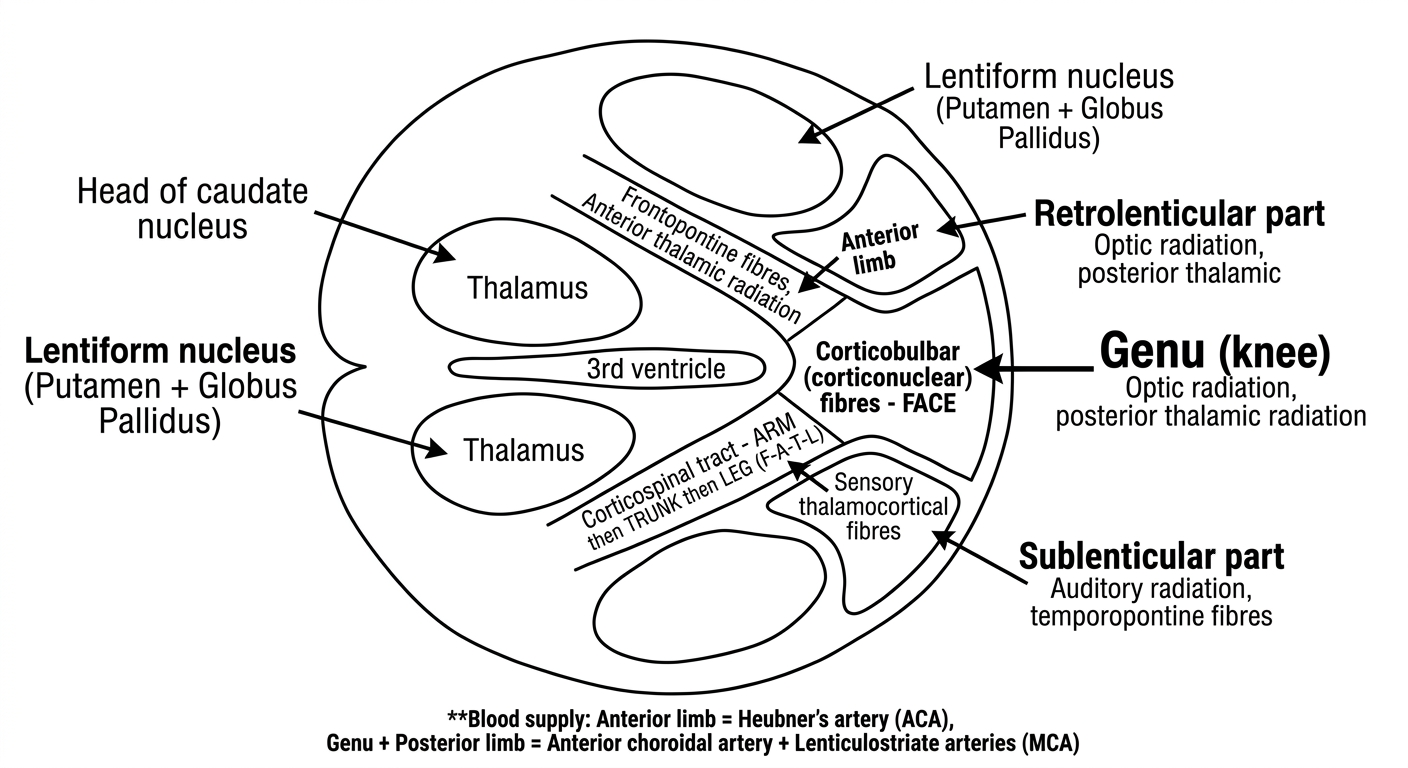
Clean simple black and white line drawing diagram of the internal capsule as seen in a HORIZONTAL section through the brain, for medical students to copy by hand. White background, black lines only, no shading or color. Draw a horizontal brain section showing the V-shaped (chevron) internal capsule with its concavity pointing laterally. The overall shape looks like two arrowheads pointing inward (like the letter V or a boomerang). Label the surrounding structures with simple shapes: - "Head of caudate nucleus" - oval on the medial side of the anterior limb - "Thalamus" - large oval on the medial side of the posterior limb - "Lentiform nucleus (Putamen + Globus Pallidus)" - oval on the lateral side of both limbs - "3rd ventricle" - narrow space in the center Label the 5 parts of the internal capsule clearly with arrows/lines pointing to each segment: 1. "Anterior limb" - front part of the V 2. "Genu (knee)" - the bend/apex of the V - write in bold 3. "Posterior limb" - back part of the V 4. "Retrolenticular part" - behind the lentiform nucleus 5. "Sublenticular part" - below the lentiform nucleus Inside each segment, write small text showing the fibers it carries: - Anterior limb: "Frontopontine fibres, Anterior thalamic radiation" - Genu: "Corticobulbar (corticonuclear) fibres - FACE" - Posterior limb (front): "Corticospinal tract - ARM then TRUNK then LEG (F-A-T-L)" - Posterior limb (back): "Sensory thalamocortical fibres" - Retrolenticular: "Optic radiation, posterior thalamic radiation" - Sublenticular: "Auditory radiation, temporopontine fibres" Add a small note at bottom: "Blood supply: Anterior limb = Heubner's artery (ACA), Genu + Posterior limb = Anterior choroidal artery + Lenticulostriate arteries (MCA)" Bold labels, clean educational style.
Internal Capsule - Drawable Diagram
Drawable Line Diagram (Horizontal Section)
Textbook Diagram - 3D Representation with Fiber Contents
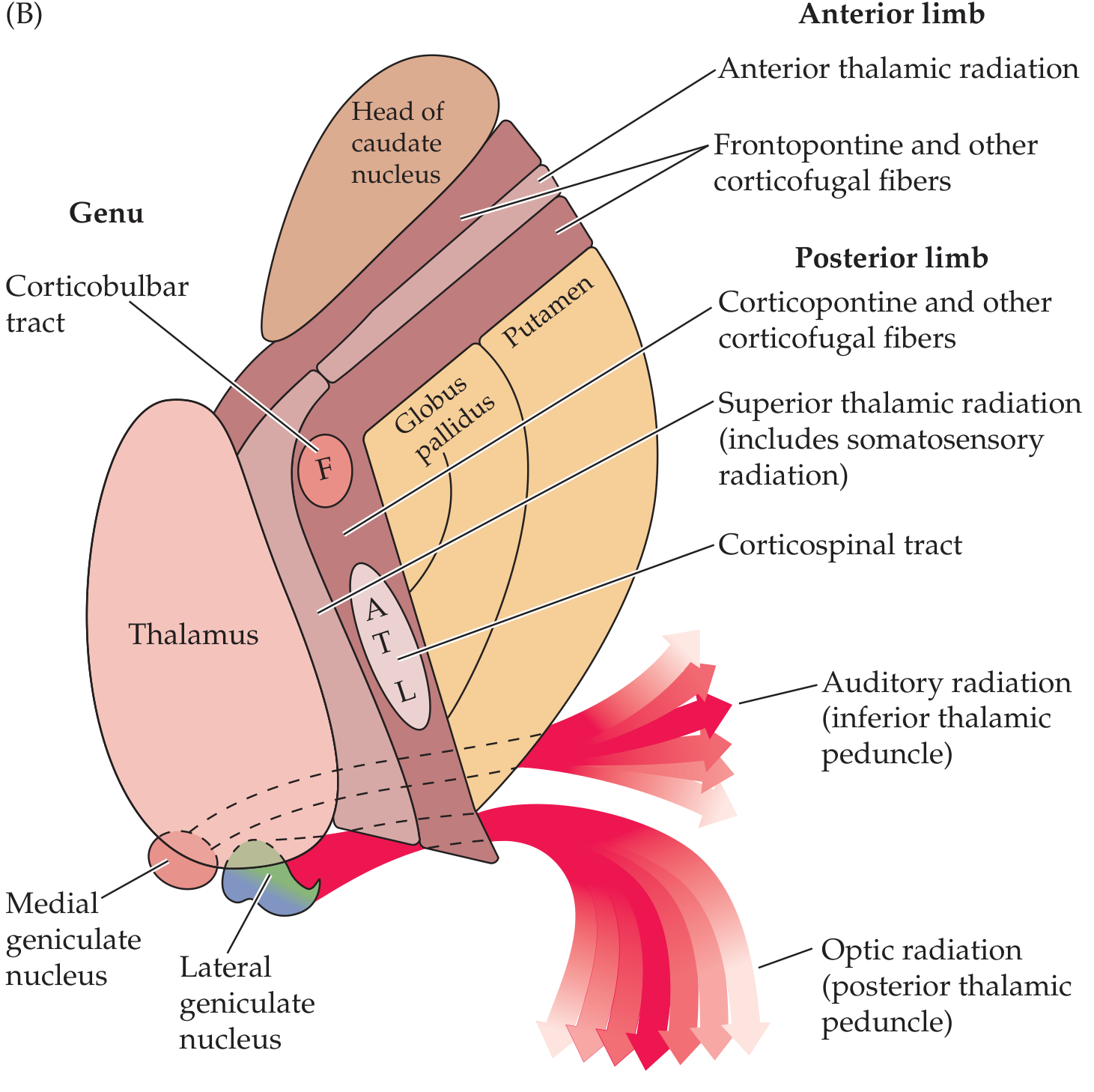
Definition & Shape
- Rostrally it is continuous with the corona radiata
- Caudally it continues as the cerebral peduncles of the midbrain
Relations (What Surrounds It)
| Side | Structure |
|---|---|
| Medial to anterior limb | Head of caudate nucleus |
| Medial to posterior limb | Thalamus |
| Lateral to both limbs | Lentiform nucleus (Putamen + Globus Pallidus) |
Memory rule: Caudate & Thalamus = always MEDIAL; Lentiform nucleus = always LATERAL
5 Parts and Their Fibre Contents
1. Anterior Limb
- Frontopontine fibres (corticopontine - frontal lobe → pons)
- Anterior thalamic radiation (thalamus ↔ prefrontal cortex)
- Caudate-putamenal fibres
2. Genu ("Knee")
- Corticobulbar (corticonuclear) fibres → motor cranial nerve nuclei
- Face fibres concentrated here → genu lesion = face + tongue weakness (capsular genu syndrome)
- Corticoreticular fibres
3. Posterior Limb
- Corticospinal tract - somatotopically arranged anterior → posterior:
- F - A - T - L = Face → Arm → Trunk → Leg (most anterior to most posterior)
- Superior thalamic radiation (somatosensory fibres, VPL → parietal cortex)
- Corticorubral fibres
4. Retrolenticular Part
- Optic radiation (lateral geniculate nucleus → visual cortex) - also called the geniculo-calcarine tract / radiatio optica
- Posterior thalamic radiation
- Corticotectal fibres
5. Sublenticular Part
- Auditory radiation (medial geniculate nucleus → auditory cortex)
- Temporopontine fibres
Blood Supply - High Yield!
| Part | Artery | Parent vessel |
|---|---|---|
| Anterior limb | Recurrent artery of Heubner | ACA (anterior cerebral artery) |
| Genu + middle/inferior posterior limb | Anterior choroidal artery | ICA |
| Superior anterior + posterior limb | Lenticulostriate arteries | MCA (middle cerebral artery) |
The lenticulostriate arteries are the classic "arteries of stroke" - they are small perforating end-arteries prone to hypertensive rupture → internal capsule haemorrhage → contralateral hemiplegia
Clinical Importance
- All motor fibres for face, arm, trunk and leg are packed tightly together here
- Small lacunar infarct → dense contralateral hemiplegia involving face + arm + leg equally
- Sensory loss if superior thalamic radiation also involved
Mnemonic for parts anterior → posterior:
"A Gentleman Properly Reads Stories" = Anterior limb → Genu → Posterior limb → Retrolenticular → Sublenticular
Drawable diagram of transverse section of medulla atlevel of pyramidal decussciation
Clean simple black and white line drawing diagram of a TRANSVERSE SECTION OF THE MEDULLA at the level of PYRAMIDAL DECUSSATION, for medical students to copy by hand in an exam. White background, black lines only, no shading or color, bold clear labels. Draw a rounded oval shape representing the cross-section. Orient it with DORSAL at top and VENTRAL at bottom. Label the following structures with clear leader lines pointing to each: DORSAL region (top): - "Central canal" - small circle in the center-top - "Posterior horn grey matter (central grey)" - butterfly/H-shaped grey matter around central canal - "Fasciculus gracilis" - dorsomedial white column (label both sides) - "Fasciculus cuneatus" - dorsolateral white column (label both sides) - "Nucleus gracilis" - small oval embedded in posterior grey (medial, both sides) - "Nucleus cuneatus" - small oval embedded in posterior grey (lateral to gracilis, both sides) LATERAL region: - "Spinal tract of CN V (trigeminal)" - small bundle in lateral white matter - "Spinal nucleus of CN V" - small oval just medial to the tract - "Anterolateral system (spinothalamic tract)" - small bundle in anterolateral white matter - "Anterior horn" - large anterior grey horn with label "Motor neurons (C1 spinal)" VENTRAL region (bottom) - THE KEY FEATURE: - Draw two large X-shaped CROSSING BUNDLES dominating the anterior part of the section - Label them: "DECUSSATING CORTICOSPINAL FIBRES" with a large bold label - On the left side (before crossing): "Corticospinal fibres (left)" - On the right side (after crossing): "Lateral corticospinal tract (right)" - Where they cross the midline: "PYRAMIDAL DECUSSATION (Motor decussation)" in bold - Small remnant anterior pyramids: "Anterior corticospinal tract (uncrossed 15%)" Add a note box: "~85% of fibres cross here → Lateral corticospinal tract. ~15% remain uncrossed → Anterior corticospinal tract" Add directional labels: "DORSAL" at top, "VENTRAL" at bottom, "LEFT" and "RIGHT" on sides. Educational medical anatomy style, all labels clearly legible.
Transverse Section of Medulla - Level of Pyramidal Decussation
Drawable Diagram
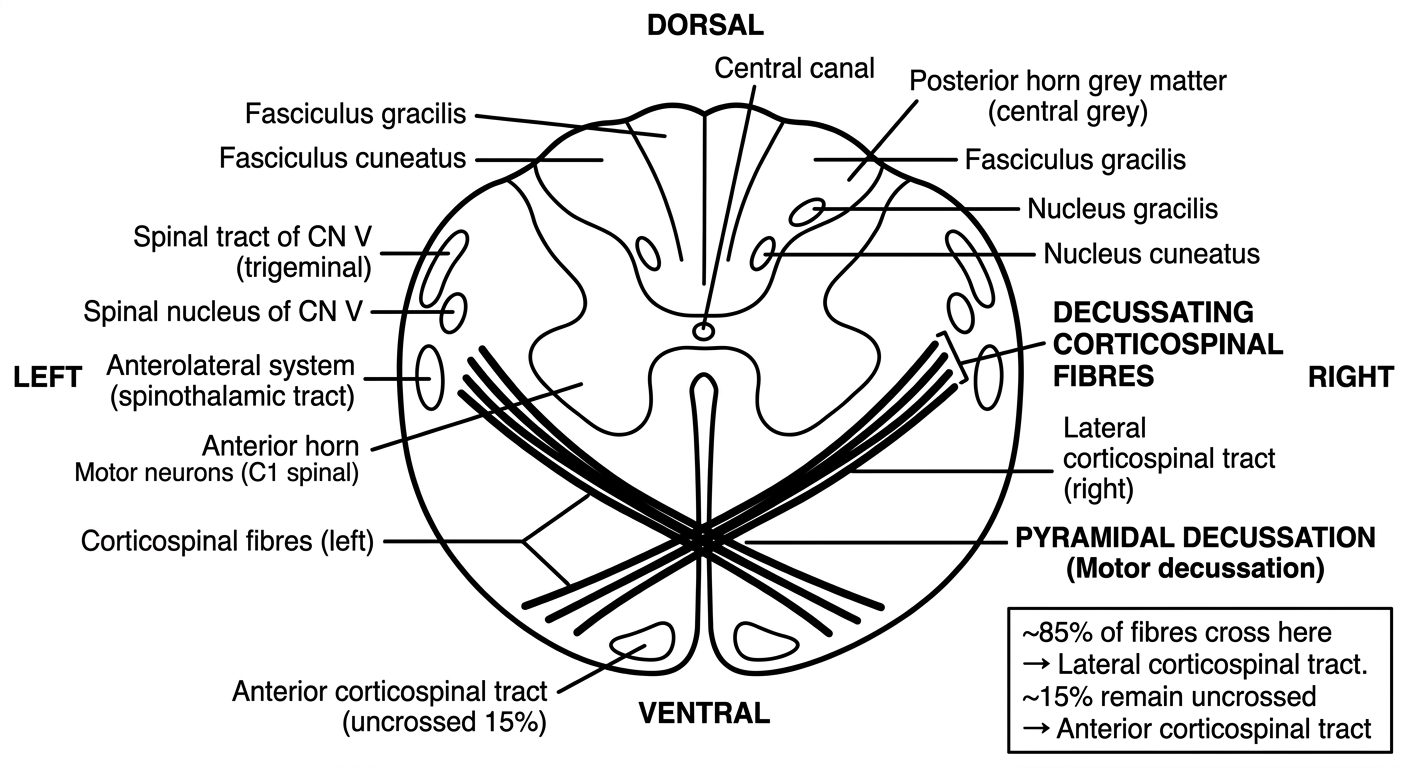
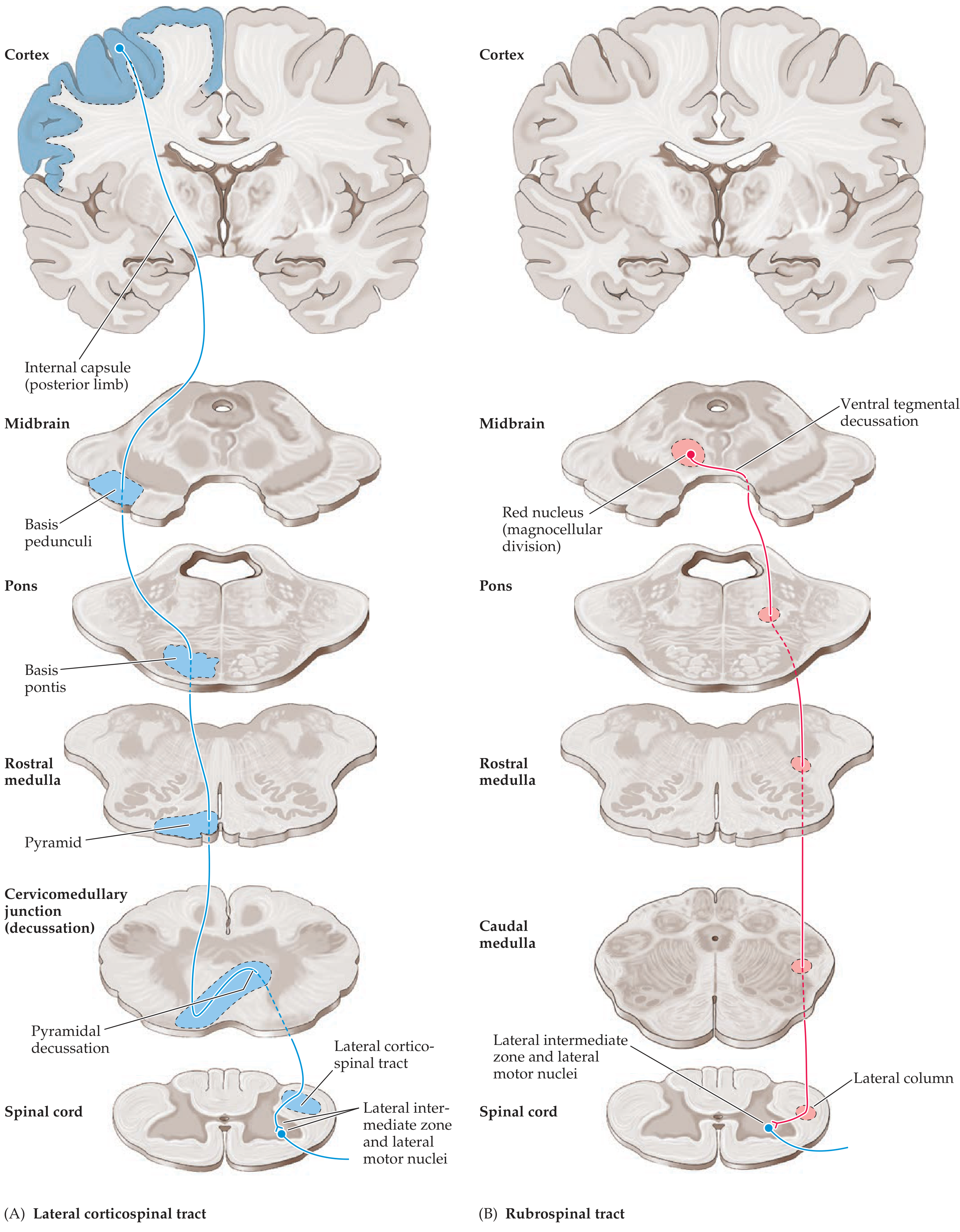
Textbook Pathway Diagram (showing where decussation fits)
Level & Context
Structures Seen - Organized Dorsal to Ventral
Dorsal Region
| Structure | Position | Significance |
|---|---|---|
| Central canal | Midline, dorsal | Remnant of ventricular system |
| Nucleus gracilis | Dorsomedial (paired) | 2nd order neurone for vibration/proprioception - lower limb |
| Nucleus cuneatus | Dorsolateral to gracilis (paired) | 2nd order neurone for vibration/proprioception - upper limb |
| Fasciculus gracilis | Dorsomedial white matter | Ascending posterior column - lower limb |
| Fasciculus cuneatus | Dorsolateral white matter | Ascending posterior column - upper limb |
Lateral Region
| Structure | Position | Significance |
|---|---|---|
| Spinal tract of CN V | Lateral white matter | Descending pain/temp fibres from face |
| Spinal nucleus of CN V | Just medial to spinal tract | Relay for facial pain/temperature |
| Anterolateral system (spinothalamic) | Anterolateral white matter | Pain/temperature from contralateral body (already crossed in spinal cord) |
Anterior/Ventral Region - THE KEY FEATURE
LEFT PYRAMID RIGHT PYRAMID
(corticospinal fibres) (corticospinal fibres)
\ /
\ X X X X X /
\ X X /
X DECUSSATION X
/ X X \
/ X X X X X \
/ \
RIGHT lateral corticospinal LEFT lateral corticospinal
tract (in spinal cord) tract (in spinal cord)
- ~85% of corticospinal fibres sweep across the midline here → become the lateral corticospinal tract on the opposite side
- ~15% do not cross → continue as the anterior corticospinal tract (cross later at spinal cord segmental level)
- The crossing fibres break up the anterior grey commissure, giving this section its distinctive X-shaped ventral pattern
Anterior Horn
- Anterior horn grey matter is present laterally → contains C1 spinal motor neurones (for neck muscles)
- Motor cells here are already below the decussation → they control ipsilateral muscles
Key Points for Exam
- What crosses: Corticospinal (pyramidal) motor fibres
- Direction: Ventral midline - fibres from each side sweep laterally across
- Proportion: 85-90% cross → lateral corticospinal tract; 10-15% descend uncrossed → anterior corticospinal tract
- Somatotopy: Lower limb fibres cross most laterally; upper limb fibres cross more medially
- Clinical rule: Lesion above decussation → contralateral hemiplegia; lesion below → ipsilateral weakness
Comparison of Decussation Levels
| Feature | Pyramidal Decussation | Sensory Decussation |
|---|---|---|
| Level | Most caudal medulla (cervicomedullary junction) | Just above pyramidal decussation |
| Fibres | Corticospinal (motor) | Internal arcuate fibres (sensory) |
| From | Pyramids (ventral) | Nucleus gracilis & cuneatus (dorsal) |
| Forms | Lateral corticospinal tract | Medial lemniscus |
| Location in section | Ventral, X-shaped crossing | Dorsal, arching anteriorly |
Mnemonic: "Motor fibres cross below sensory fibres" - pyramidal decussation is the most caudal of the two, just at the C1 level