Premalignant lesions of skin
Reading File
Finding Sources
Finding Sources
Searching PubMed
"premalignant skin lesions" AND management
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Premalignant Lesions of the Skin
Premalignant (precancerous) skin lesions are those with a demonstrable potential to undergo malignant transformation into invasive carcinoma. They are broadly divided into those that precede squamous cell carcinoma (SCC), those that precede melanoma, and miscellaneous others.
I. PRECURSORS OF SQUAMOUS CELL CARCINOMA
1. Actinic Keratosis (Solar Keratosis)
The most common premalignant skin lesion.
Pathogenesis: Caused by UV-induced DNA damage with mutations in TP53 and other genes frequently mutated in SCC. Chronic cumulative sun exposure is the main driver. - Robbins & Kumar Basic Pathology, p. 890
Who gets it: Elderly individuals with fair skin (Fitzpatrick types I-II), chronic outdoor sun exposure, immunosuppressed patients (e.g., organ transplant recipients).
Clinical features:
- Rough, erythematous macule or papule with white-to-yellow scale, < 1 cm diameter
- Located on head, neck, dorsal hands, forearms, bald scalp - areas of highest cumulative UV exposure
- May itch or be tender, especially hyperkeratotic variants
- Lesions can spontaneously regress, but then reappear
Clinical subtypes:
| Subtype | Features |
|---|---|
| Classic | Rough, erythematous macule/papule with scale |
| Hypertrophic | Thick papule/plaque with heavy scale-crust; may form cutaneous horn |
| Pigmented | Basilar hyperpigmentation, may mimic solar lentigo |
| Lichenoid | Band-like lymphocytic infiltrate in dermis |
| Atrophic | Thinned epidermis |
| Actinic cheilitis | Confluent AKs on the lower vermilion lip |
Malignant potential: Risk of a single AK progressing to invasive SCC is estimated at 0.1% to 20% (widely varies in literature). - Dermatology 2-Volume Set 5e, p. 2254
Histology:
- Lower epidermis shows cytologic atypia with basal cell hyperplasia or atrophy
- Hyperkeratosis with parakeratosis (retention of nuclei in stratum corneum)
- Dermal solar (actinic) elastosis - thickened blue-gray elastic fibers
- When full-thickness epidermal atypia is present, this is classified as SCC in situ (grade III / Bowen disease)
Treatment:
- Cryotherapy (liquid nitrogen): open spray, single freeze-thaw cycle 8-10 seconds; most widely used. 1-2 mm freeze margin. Cure rates ~99% in some series. - Fitzpatrick's Dermatology
- 5-Fluorouracil (5-FU) cream: field treatment for multiple lesions
- Imiquimod 5% cream: immune-mediated destruction
- Photodynamic therapy (PDT): ALA or methyl-ALA + light; clearance 50-70% single session, up to 90% with repeat. Especially effective on face and scalp. - Andrews' Diseases of the Skin
- Diclofenac 3% gel, ingenol mebutate
- Topical calcipotriol + 5-FU: a recent systematic review (2024) confirms efficacy of this combination for AK and Bowen's disease
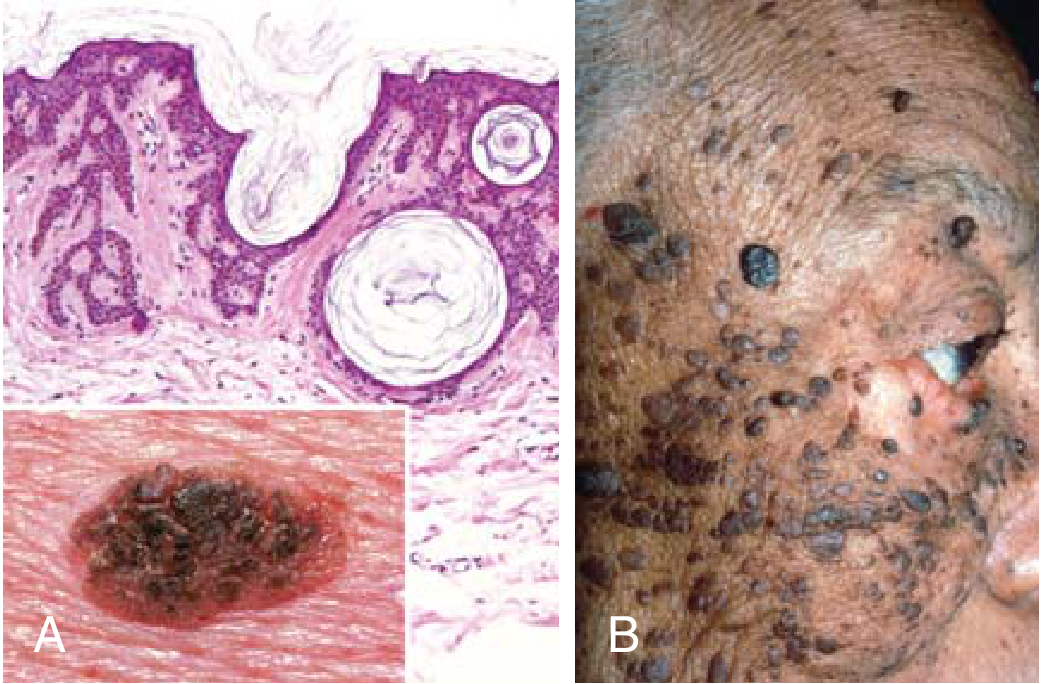
2. Squamous Cell Carcinoma In Situ (Bowen Disease)
Definition: Full-thickness epidermal atypia (keratinocyte dysplasia throughout the entire epidermis) without dermal invasion.
Clinical features:
- Slowly growing, well-demarcated, scaly, erythematous plaque
- Most common on sun-exposed sites
- Must be distinguished clinically from eczema and psoriasis (biopsy is important)
Histology:
- Full-thickness atypia of the epidermis with dyskeratosis, nuclear pleomorphism, and apoptosis - more florid than in AK
- Atypical keratinocytes extend down adnexal structures (hair follicles, sweat glands)
- Diffuse confluent parakeratosis; mitoses frequent
- Basal layer is usually spared (palisading small compressed basaloid keratinocytes at the base - key distinguishing feature from invasive SCC)
Malignant potential: Fewer than 5% become invasive SCC. However, genital Bowen disease (erythroplasia of Queyrat) has much higher progression risk: 10-30%. - Dermatology 2-Volume Set 5e
Special forms:
- Erythroplasia of Queyrat: SCC in situ of the glans penis - bright red, velvety plaque; higher malignant potential
- Bowenoid papulosis: HPV-associated SCC in situ of the genitalia in younger patients
Treatment: Topical 5-FU, PDT (76% clearance with mALA PDT), cryosurgery, excision, or radiotherapy (40-50 Gy; 5-year cure rates 98-100%). - Dermatology 5e
3. Actinic Cheilitis
- Confluent actinic keratoses on the lower lip vermilion
- Lip appears dry, scaly, cracked, atrophic with loss of clear vermilion border
- Higher progression risk than cutaneous AK due to thin epidermis and persistent UV exposure
- Treatment: PDT, 5-FU, vermilionectomy (lip shave) for extensive cases
4. Keratoacanthoma (KA)
- Rapidly growing crateriform nodule with a central keratin-filled plug, arising in hair-bearing sun-exposed skin of middle-aged to elderly patients
- Classic course: rapid growth over 6-8 weeks, then spontaneous involution over months
- Histologically resembles well-differentiated SCC - many pathologists regard it as a low-grade SCC variant rather than a truly benign entity
- Important subtypes: Keratoacanthoma centrifugum marginatum (expands peripherally without central healing), generalized eruptive KA (Grzybowski variant)
- Management: Excision is preferred (also provides full histology); some advocate curettage or intralesional methotrexate - Andrews' Diseases of the Skin
5. Cutaneous Horn (Cornu Cutaneum)
- A clinical descriptor, not a diagnosis - refers to a projecting column of compacted keratin
- The underlying pathology may be AK (most common), SCC, verruca vulgaris, seborrheic keratosis, KA, or trichilemmoma
- A biopsy of the base is mandatory to determine the underlying lesion
- "If the base is red and inflamed, suspect SCC" - Fitzpatrick's Dermatology
II. PRECURSORS OF MELANOMA
6. Lentigo Maligna (Hutchinson's Melanotic Freckle)
- Melanoma in situ arising on photodamaged skin of elderly patients
- Large, flat, irregularly pigmented patch - typically on the face and neck
- Preinvasive phase (radial growth only) - becomes lentigo maligna melanoma once vertical growth and dermal invasion occur (least common melanoma subtype, 5-10% of cases)
- Rate of progression: variable, reported between 2% and 33% - K.J. Lee's Essential Otolaryngology
- Treatment: Wide local excision with 5-10 mm margins; imiquimod 5% topical is effective for inoperable/large lesions; radiotherapy (40-50 Gy) achieves 5-year cure rates of 90-95% - Dermatology 5e
7. Dysplastic (Atypical) Nevus
The single most important marker of melanoma risk.
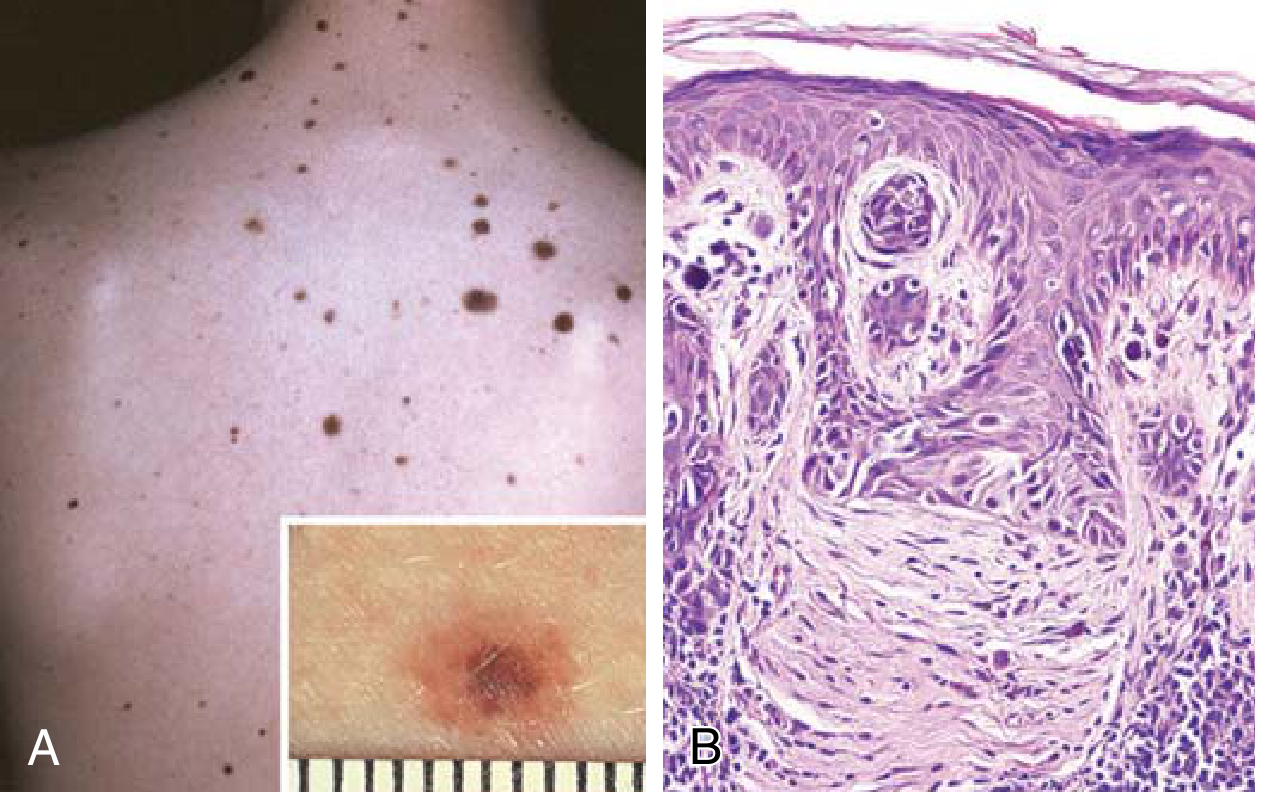
Clinical features (ABCDE rule helpful):
- Larger than ordinary nevi: often > 5 mm, may number in the hundreds
- Variable pigmentation (variegation) with irregular, ill-defined borders
- Flat macule to slightly raised plaque with "pebbly" surface
- Occur on sun-exposed AND non-sun-exposed sites
Histology:
- Compound nevi with architectural and cytologic atypia
- Enlarged junctional nests with "bridging" (fusion of adjacent nests)
- Lentiginous hyperplasia: single nevus cells replacing basal layer
- Nuclear atypia with angulated, hyperchromatic nuclei
- Sparse lymphocytic infiltrate + linear dermal fibrosis (lamellar fibroplasia) + melanin in dermal macrophages
Malignant potential:
- Familial dysplastic nevus syndrome: lifetime melanoma risk approaches 100% - Robbins & Kumar Basic Pathology
- Sporadic cases: only individuals with 10 or more dysplastic nevi have markedly increased risk
- Most melanomas arise de novo rather than from a preexisting nevus; dysplastic nevi are best viewed as markers of risk rather than obligate precursors
Management: Close surveillance, dermoscopy, serial photography. Excise if high suspicion for melanoma or if ABCDE features evolve.
8. Congenital Melanocytic Nevus
- Present at birth; occurs in 1-2% of newborns
- Risk of melanoma transformation depends on size:
- Small (<1.5 cm) and medium (1.5-20 cm): minimal increased risk
- Giant/large congenital nevus (>20 cm): approximately 10% lifetime risk of melanoma - K.J. Lee's Essential Otolaryngology
- Associated syndrome: neurocutaneous melanosis - melanotic CNS neoplasms + giant congenital nevi
III. ORAL/MUCOSAL PREMALIGNANT LESIONS (Relevant to Skin-Adjacent Sites)
Leukoplakia
- White mucosal plaque that cannot be rubbed off and cannot be classified as another disease
- < 10% of isolated leukoplakias prove to be carcinoma or severe dysplasia on biopsy
Erythroplakia
- Fiery red mucosal patch - much higher malignant potential than leukoplakia
- Histology ranges from severe dysplasia to frank carcinoma in situ in most biopsied cases
- Speckled erythroplakia (mixed red-white) has intermediate risk
IV. Summary Table
| Lesion | Malignant Potential | Progression To | Key Feature |
|---|---|---|---|
| Actinic keratosis | 0.1-20% per lesion | Cutaneous SCC | TP53 mutation; UV-induced |
| Bowen disease (SCC in situ) | <5% (genital 10-30%) | Invasive SCC | Full-thickness epidermal atypia |
| Actinic cheilitis | Higher than skin AK | SCC of lip | Loss of vermilion border |
| Keratoacanthoma | Low-grade SCC variant | SCC (disputed) | Rapid growth, central keratin crater |
| Cutaneous horn | Depends on base | SCC (if base is AK) | Biopsy the base |
| Lentigo maligna | 2-33% | Lentigo maligna melanoma | Melanoma in situ; face of elderly |
| Dysplastic nevus | Marker of risk (familial ~100%) | Melanoma | ABCDE features; lentiginous hyperplasia |
| Giant congenital nevus | ~10% lifetime | Melanoma | >20 cm, present at birth |
| Leukoplakia | <10% | Oral SCC | White mucosal plaque |
| Erythroplakia | High (>50%) | Oral SCC | Red mucosal plaque |
V. General Principles of Management
- Sun protection (SPF 30+, protective clothing, avoiding peak UV hours) - primary prevention
- Regular skin surveillance - especially in fair-skinned individuals, immunosuppressed, transplant patients
- Biopsy any lesion with atypical features or that does not respond to treatment
- Field therapy for patients with multiple/diffuse AKs (5-FU, imiquimod, PDT, ingenol mebutate)
- Treat all SCC in situ (Bowen disease) regardless of perceived invasive risk
- Dermoscopy aids diagnosis and monitoring of pigmented lesions
Sources:
- Dermatology 2-Volume Set 5e (Bolognia et al.)
- Robbins & Kumar Basic Pathology (Robbins Pathology)
- Fitzpatrick's Dermatology (2-volume edition)
- Andrews' Diseases of the Skin - Clinical Dermatology
- K.J. Lee's Essential Otolaryngology
- Recent systematic review on topical calcipotriol + 5-FU for AK and Bowen disease (PMID 38783539)
This is a shared conversation. Sign in to Orris to start your own chat.