A 3 month old girl with fever for 8 days, and rashes for 3 days, what is the differentials
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
fever rash infant differential diagnosis
Searching PubMed
Kawasaki disease infant atypical young age
Loading Image
Now I have comprehensive information to construct a thorough answer. Let me synthesize this.
Differential Diagnosis: 3-Month-Old Girl with 8 Days of Fever + 3 Days of Rash
This is a high-priority pediatric presentation. In a 3-month-old, prolonged fever with rash narrows the differential but must be approached systematically - serious life-threatening conditions must be excluded first.
Priority 1 - Must Rule Out (Life-Threatening)
1. Incomplete/Atypical Kawasaki Disease (KD) - TOP PRIORITY
This is the most important diagnosis NOT to miss in this age group.
"Baseline echocardiogram should be strongly considered for any infant <6 months with fever of 7 days or greater duration, even in the absence of clinical or laboratory criteria." - The Harriet Lane Handbook, 23rd ed.
At 3 months, classic KD criteria are often not met (hence "incomplete KD"), yet the coronary artery risk is identical. Classic features include:
- Fever ≥5 days + 4 of 5 criteria: bilateral conjunctival injection, oral changes (strawberry tongue, cracked lips), polymorphous rash (morbilliform, maculopapular, or scarlatiniform), swelling/erythema of hands/feet, cervical lymphadenopathy >1.5 cm
- In incomplete KD: fewer than 4 criteria, but laboratory support (WBC ≥15,000, CRP/ESR elevated, albumin ≤3.0, platelets ≥450,000 after day 7, sterile pyuria, elevated ALT) + echocardiogram findings guide diagnosis
- Untreated, 20-25% develop coronary artery aneurysms
Pearl: Infants <6 months are MORE likely to present with incomplete KD and are at HIGHER risk for coronary complications.
2. Bacterial Sepsis with Skin Manifestations
- E. coli, GBS (Group B Strep), Listeria, Staphylococcal bacteremia can all present with rash
- Meningococcemia: non-blanching petechial or purpuric rash - a medical emergency
- Toxic shock syndrome: diffuse erythroderma, desquamation
3. Bacterial Meningitis with Rash
- Fever + petechiae/purpura = meningococcal meningitis until proven otherwise
- May have bulging fontanelle, irritability, nuchal rigidity (though unreliable in this age group)
Priority 2 - Viral Exanthems
4. Roseola Infantum (Exanthem Subitum) - HHV-6
Classic pattern closely matches this presentation:
- Incubation 5-15 days (avg 10 days)
- High fever lasting 3-7 days, followed by appearance of rash as fever resolves - the rash appears 1 day before to 1-2 days after defervescence
- "Rose"-colored macules and papules, 2-5 mm, surrounded by white halo, widespread on neck and trunk
- May have palpebral edema ("sleepy" appearance) and Nagayama spots (erythematous papules on soft palate)
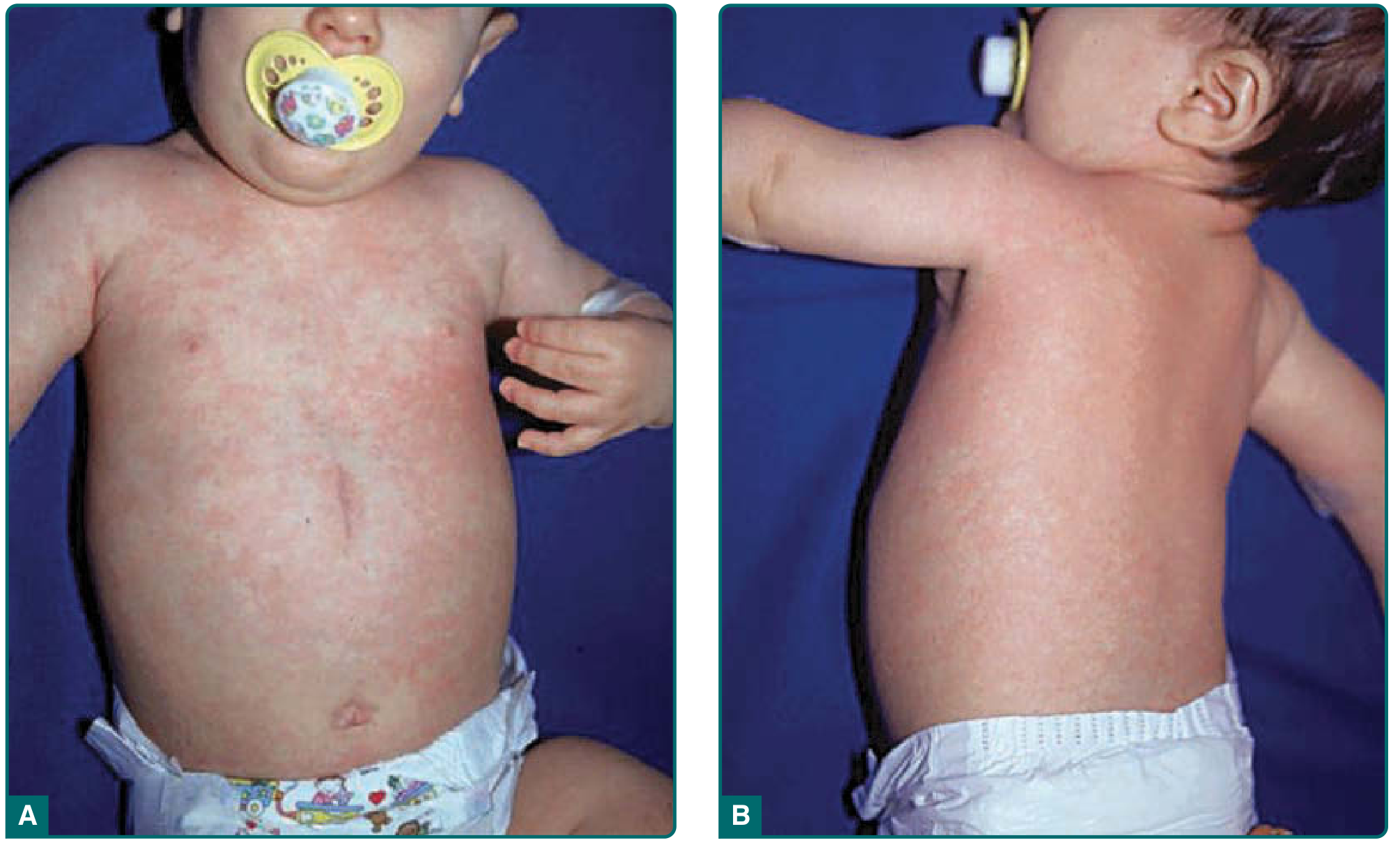
Exanthem subitum in an infant - truncal pink macules and papules that appeared 1 day after defervescence. (Fitzpatrick's Dermatology)
However: Classical roseola typically occurs 6-24 months; at 3 months, maternal antibodies should still be providing some protection, making this less common but still possible.
5. Enteroviral Infection (Coxsackie/Echovirus)
- Common viral exanthem in infants
- Maculopapular or vesicular rash
- May have fever for several days before rash
- Can cause aseptic meningitis - important consideration in this age group
6. Parvovirus B19 (Fifth Disease)
- Fever followed by characteristic slapped-cheek appearance and lacy reticular rash
- Less typical at 3 months but possible
7. Measles (Rubeola)
- Prodrome: high fever, cough, coryza, conjunctivitis, Koplik spots
- Rash appears day 3-5 of illness, maculopapular starting at head and descending
- Important if unvaccinated or travel history (too young to be vaccinated)
8. Congenital/Early Cytomegalovirus (CMV) or EBV
- Prolonged fever with petechial or maculopapular rash
- Hepatosplenomegaly, lymphadenopathy
Priority 3 - Inflammatory/Rheumatologic
9. Systemic JIA (sJIA) / Still's Disease
- Although rare at 3 months, presents with quotidian fever (daily spiking pattern), salmon-colored evanescent rash that comes and goes with fever spikes, arthritis, hepatosplenomegaly
- Rash is classically present during fever and disappears when afebrile
10. Drug Reaction / Serum Sickness
- If the infant received any medications or vaccines in the preceding weeks
- Urticarial or morbilliform rash with prolonged fever
Priority 4 - Less Common but Notable
11. Congenital Syphilis
- Can present at 3 months with persistent fever, maculopapular or desquamating rash (palms/soles), hepatosplenomegaly, bone pain
- Maternal history important
12. Staphylococcal Scalded Skin Syndrome (SSSS)
- Diffuse erythema with blistering/peeling
- Fever + positive Nikolsky sign
13. Neonatal Lupus
- Transient photosensitive annular rash, heart block
- Due to passage of maternal anti-Ro/SSA antibodies
- Rash typically appears 4-6 weeks of life and can persist to ~3 months
Recommended Workup Framework
| Investigation | Rationale |
|---|---|
| CBC with differential | Leukocytosis (KD, sepsis), anemia |
| CRP, ESR | Elevated in KD, bacterial infection |
| Blood culture x2 | Bacteremia/sepsis |
| Urinalysis + culture | Sterile pyuria (KD), UTI |
| LFTs, albumin | KD liver involvement |
| Echocardiogram | Mandatory if fever ≥7 days in infant <6 months |
| LP (if meningism/irritability) | Meningitis workup |
| Platelets | Thrombocytosis (KD after day 7) |
| Viral panel (enterovirus, HHV-6) | Viral exanthem workup |
| Chest X-ray | Pneumonia, cardiomegaly |
| VDRL/RPR if clinically indicated | Congenital syphilis |
Bottom Line
In a 3-month-old with 8 days of fever and 3 days of rash, the working diagnosis until proven otherwise is incomplete Kawasaki Disease - this age group is at higher risk for missed diagnosis AND higher risk for coronary complications. An echocardiogram is indicated now. Simultaneously, sepsis and meningococcemia must be excluded urgently. Roseola/viral exanthem is the most common benign explanation but is a diagnosis of exclusion in this age group.
- The Harriet Lane Handbook, 23rd ed. (Johns Hopkins Hospital)
- Fitzpatrick's Dermatology, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.