malaria
Reading File
Asking for Preferences
all
Finding Sources
Searching PubMed
malaria treatment prevention
Searching the Web
malaria overview lifecycle diagnosis treatment 2025 WHO guidelines
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Malaria - Comprehensive Overview
1. Epidemiology
Malaria remains one of the most serious infectious diseases worldwide. The WHO estimated ~219 million cases and ~435,000 deaths annually, primarily children infected with P. falciparum in sub-Saharan Africa. More than 41% of the world's population lives in endemic zones (Africa, Asia, Oceania, Central/South America). Most fatalities in the developed world stem from delayed diagnosis, since clinicians may not recognize the risk in returning travelers. - Murray & Nadel's Textbook of Respiratory Medicine, p. 1352
2. Causative Species
Five Plasmodium species infect humans:
| Species | Fever Periodicity | Notes |
|---|---|---|
| P. falciparum | Every 48 h (but unreliable) | Most deadly; causes cerebral malaria, multiorgan failure |
| P. vivax | Every 48 h | Can relapse (hypnozoites in liver) |
| P. ovale | Every 48 h | Can relapse (hypnozoites in liver) |
| P. malariae | Every 72 h | Mild; can persist for decades |
| P. knowlesi | Every 24 h | Simian parasite (SE Asia); morphologically mimics P. malariae but can be virulent |
All are transmitted by the bite of female Anopheles mosquitoes. Humans are the only natural reservoir for the first four species. - Robbins & Kumar Basic Pathology, p. 392
3. Life Cycle & Pathogenesis

Step-by-step:
- Mosquito bite - sporozoites injected into bloodstream
- Hepatic (pre-erythrocytic) stage - sporozoites travel to liver; surface proteins (thrombospondin-related adhesive protein, circumsporozoite protein) bind heparan sulfate proteoglycans on hepatocytes; sporozoites enter and differentiate into merozoites (clinically silent phase, 1-4 weeks)
- Hepatocyte rupture - thousands of merozoites released into blood
- Erythrocytic stage - a lectin-like molecule on merozoites binds sialidated glycophorin on RBCs; merozoites invaginate into a digestive vacuole and differentiate into ring trophozoites → trophozoites → schizonts
- Schizont phase - schizonts express PfEMP1 (P. falciparum erythrocyte membrane protein 1), which forms knob-like extensions on the RBC surface and binds endothelial adhesion molecules (ICAM-1, VCAM-1, CD36) - causing sequestration of infected RBCs in capillary beds
- Red cell lysis - schizonts differentiate into merozoites; RBCs lyse and release merozoites to infect new RBCs (cycle continues)
- Gametocyte formation - some trophozoites differentiate into gametocytes, which are taken up by another mosquito and restart the sexual cycle
For P. vivax / P. ovale: some sporozoites form dormant hypnozoites in hepatocytes, responsible for relapses months to years later. - Robbins & Kumar Basic Pathology, p. 392
4. Clinical Features
Typical Presentation
- Episodic fever with rigors/chills corresponding to synchronized RBC lysis and merozoite release
- Headache, myalgia, malaise, nausea/vomiting
- Fever periodicity: 24 h (P. knowlesi), 48 h (P. falciparum, P. vivax, P. ovale), 72 h (P. malariae) - but periodic fever is not a reliable sign, especially in P. falciparum
- Splenomegaly (massive in chronic infection) and hepatomegaly from hyperplasia of mononuclear phagocytes and deposition of malarial pigment (hematin)
- Hemolytic anemia (universal)
Severe Malaria (P. falciparum)
| Feature | Mechanism |
|---|---|
| Cerebral malaria | Sequestration of parasitized RBCs in brain microvessels; cytokine-mediated inflammation |
| Blackwater fever | Massive intravascular hemolysis → hemoglobinemia, hemoglobinuria, jaundice, renal failure |
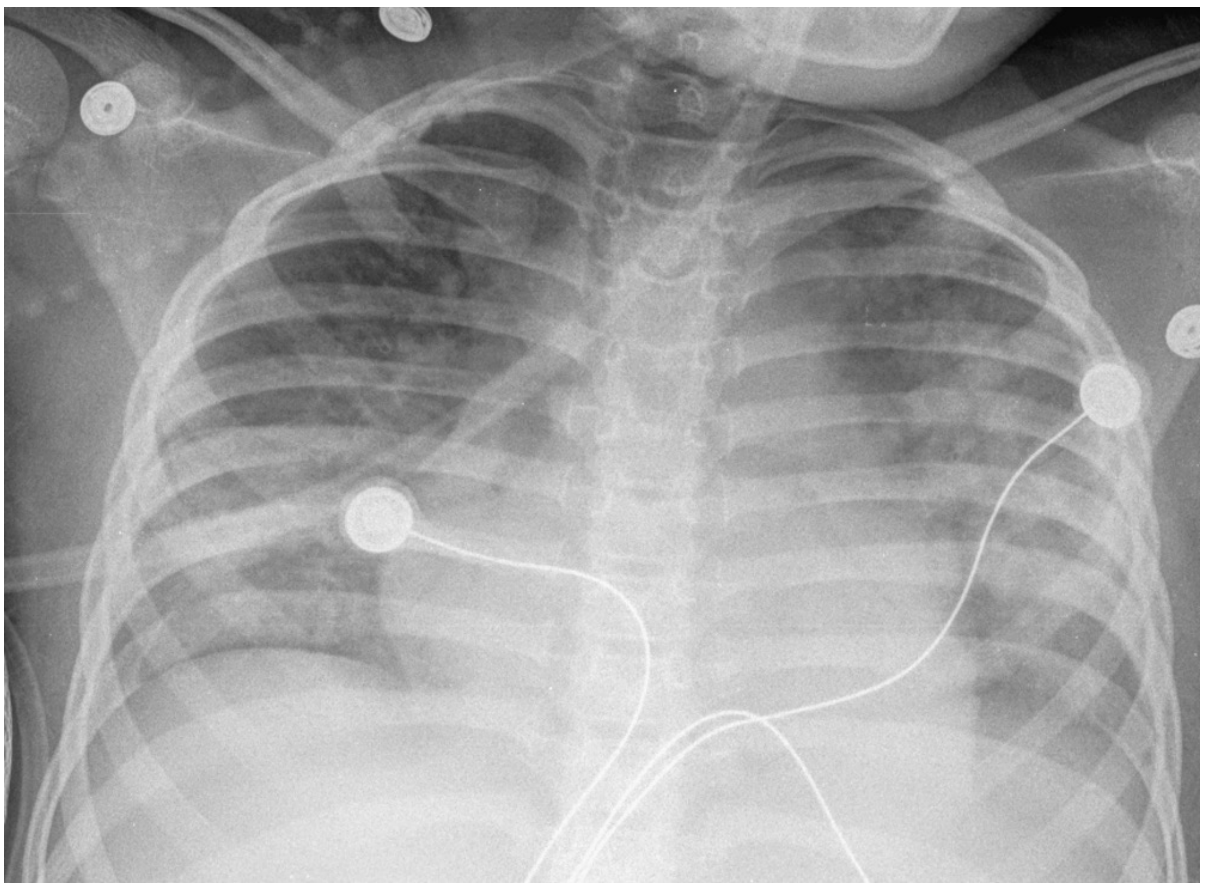
| ARDS / pulmonary edema | Increased alveolar-capillary permeability; may appear even after starting treatment |
| Hypoglycemia | Parasite glucose consumption + anorexia + quinine-induced insulin release |
| Thrombocytopenia | Common; from splenic sequestration + destruction |
| Acute kidney injury | From hemoglobinuria, cytokines, reduced perfusion |
| Acidosis | Tissue hypoxia from anemia and vascular obstruction |
Parasitemia >10% of erythrocytes or presence of mature P. falciparum forms in peripheral blood = severe disease. - Murray & Nadel's Textbook of Respiratory Medicine, p. 1352
Chest X-ray may show diffuse bilateral opacities resembling pulmonary edema:
5. Diagnosis
Gold standard: Peripheral blood smear - thick and thin films stained with Giemsa or Wright stain
- Thick smear: detects whether parasites are present (higher sensitivity)
- Thin smear: identifies the species by RBC morphology
- Important note: P. falciparum shows only immature ring forms in peripheral blood (mature forms sequester in microvessels); initial smears may be negative - repeat after 8 hours if high suspicion
Rapid Diagnostic Tests (RDTs): Antigen-based point-of-care tests (e.g., BinaxNOW) - detect P. falciparum-specific HRP2 antigen and pan-malarial pLDH. Fast (~15 min), ~$5/test. Less sensitive than microscopy. Antigen can persist after treatment, so cannot reliably distinguish current from very recent infection.
PCR: More sensitive and specific than microscopy; available from reference labs; not widely available point-of-care. Especially useful for mixed infections and low parasitemias.
Key laboratory findings:
- Hemolytic anemia (elevated LDH, indirect bilirubin, reticulocytosis)
- Thrombocytopenia
- Elevated creatinine (in severe disease)
- Hypoglycemia - Rosen's Emergency Medicine, p. 2660
6. Treatment
Uncomplicated Malaria
| Situation | Treatment |
|---|---|
| Chloroquine-sensitive regions (Haiti, Dominican Republic, Central America N of Panama Canal, limited Middle East) | Chloroquine phosphate oral |
| Chloroquine-resistant regions (most of Africa, Asia, S America) | Artemether-lumefantrine (Coartem) - first-line oral; OR Atovaquone-proguanil (Malarone); OR oral quinine + doxycycline/clindamycin |
| P. vivax / P. ovale (to prevent relapse) | Add primaquine (check G6PD first) or tafenoquine to eliminate hypnozoites |
G6PD deficiency: Primaquine and tafenoquine are contraindicated - they precipitate severe hemolysis. G6PD testing required before use.
Severe Malaria
- IV artesunate - first-line treatment worldwide
- Dose: 2.4 mg/kg IV at 0, 12, 24 hours, then every 24 h
- Switch to oral therapy once stable and parasitemia <1%
- In the US: available via CDC Malaria Hotline (855-856-4713); after hours 770-488-7100
- IV quinine/quinidine: alternative where artesunate unavailable; requires cardiac monitoring (risk of hypoglycemia, QT prolongation)
- Cerebral malaria: IV artesunate/quinine + mechanical ventilation if comatose + antiepileptics + correct acidosis and hypoglycemia
- Exchange transfusion: no longer recommended by CDC (benefit unestablished)
- Fluid management: careful balance - avoid overload to prevent pulmonary edema while maintaining organ perfusion
Artesunate resistance is emerging in SE Asia (manifested as slower parasitemia clearance), requiring longer treatment courses. - Rosen's Emergency Medicine, Murray & Nadel
7. Prevention
Personal Protective Measures
- Insecticide-treated bed nets (ITNs) - most cost-effective intervention
- DEET-containing insect repellents
- Permethrin-treated clothing
- Indoor residual spraying (IRS) - WHO 2025 guidelines updated to include chlorfenapyr and isocycloseram as new approved insecticides
- Spatial emanators / spatial repellents - new recommendation in WHO Malaria Guidelines August 2025
Chemoprophylaxis for Travelers
| Drug | Regimen | Notes |
|---|---|---|
| Atovaquone-proguanil (Malarone) | Start 1-2 days before, during, and 7 days after travel | Fewer side effects; expensive |
| Doxycycline | Start 1-2 days before, during, and 28 days after | Cheap; photosensitivity; no use in children <8 yr or pregnancy |
| Mefloquine | Weekly; start 2-3 weeks before | Neuropsychiatric side effects; increasing resistance |
| Chloroquine | Weekly (chloroquine-sensitive areas only) | Rarely used now due to widespread resistance |
| Primaquine | Daily (for P. vivax-only destinations); requires G6PD testing |
Intermittent Preventive Treatment (IPT)
- IPTp (in pregnancy): Sulfadoxine-pyrimethamine (SP) given at routine antenatal visits in endemic areas. A 2025 Lancet Infectious Diseases meta-analysis notes increasing SP resistance in Africa, raising concerns about IPTp effectiveness - the effectiveness of IPTp with SP is declining in regions with high-level SP resistance
- Seasonal Malaria Chemoprevention (SMC): SP + amodiaquine given monthly to children during peak transmission season in the Sahel
Vaccine
- RTS,S/AS01 (Mosquirix): first licensed malaria vaccine; targets circumsporozoite protein of P. falciparum; partial protection (~30-50%) but expected to prevent thousands of fatal cerebral malaria cases in children when fully deployed
- R21/Matrix-M: newer vaccine showing ~75% efficacy; recommended by WHO 2023 - Robbins & Kumar Basic Pathology, p. 393
Public Health
- Elimination of stagnant water (mosquito breeding sites)
- Community-wide IRS programs
- Surveillance and early case detection
8. Genetic Protection Against Malaria
Malaria has exerted profound selective pressure on human evolution. Several genetic RBC abnormalities are most prevalent in malaria-endemic regions because they offer protection from severe disease:
- Sickle cell trait (HbAS): protective against P. falciparum severe malaria
- Thalassemia (alpha and beta)
- G6PD deficiency
- Pyruvate kinase deficiency
- Duffy antigen negativity (most West Africans lack the Duffy antigen, making them resistant to P. vivax)
There is no sterile immunity to malaria. - Murray & Nadel's Textbook of Respiratory Medicine, p. 1352
Recent Evidence (2024-2026)
- van Eijk et al., Lancet Infect Dis 2025 (PMID 40675171): Updated meta-analysis confirms IPTp with sulfadoxine-pyrimethamine effectiveness is declining in Africa due to SP resistance - a significant concern for malaria control in pregnancy
- Ruisch et al., Malar J 2024 (PMID 39695670): Systematic review on the cost of seasonal malaria chemoprevention (SMC) - informing WHO scale-up decisions
Summary Mnemonic - "FALCI" for severe malaria features:
- Fever (high-grade, periodic)
- Anemia (hemolytic)
- Liver/kidney failure (blackwater fever, AKI)
- Cerebral malaria (convulsions, coma)
- Impaired gas exchange (ARDS, pulmonary edema)
systemic lupus erythamatous
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND treatment
Searching the Web
systemic lupus erythematosus 2025 guidelines diagnosis treatment ACR EULAR
Reading File
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND guideline
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Systemic Lupus Erythematosus (SLE) - Comprehensive Overview
1. Definition & Epidemiology
SLE is a chronic, systemic autoimmune disease characterized by immune complex deposition and autoantibody production against nuclear antigens, causing inflammation and damage across virtually every organ system.
- Prevalence: ~50-100 per 100,000 in Western populations; higher in Asians, Blacks, and Hispanics
- Sex ratio: 9:1 female-to-male predominance
- Peak age: Women of reproductive age (15-45 years)
- Race/ethnicity: More common and more severe in Black and Hispanic patients; Asian patients have higher rates of renal involvement
- Lupus nephritis is the leading cause of secondary glomerular disease in countries such as China, Korea, and Japan (>50% of cases)
2. Pathogenesis
SLE results from breakdown of self-tolerance due to interplay of genetic, hormonal, and environmental factors:
Genetic Factors
- HLA associations: HLA-DR2 and HLA-DR3 (odds ratio 2-3 each; ~5 if both present)
- Complement deficiencies: C1q, C2, or C4 deficiency (seen in ~5% of SLE patients) impairs clearance of immune complexes and apoptotic cells
- FcγRIIB polymorphism: Defective inhibitory Fc receptor - fails to control B cell activation
- PTPN22 and many other genes identified by GWAS
- CCR6 variants: Associated with lupus nephritis susceptibility (especially in Chinese patients)
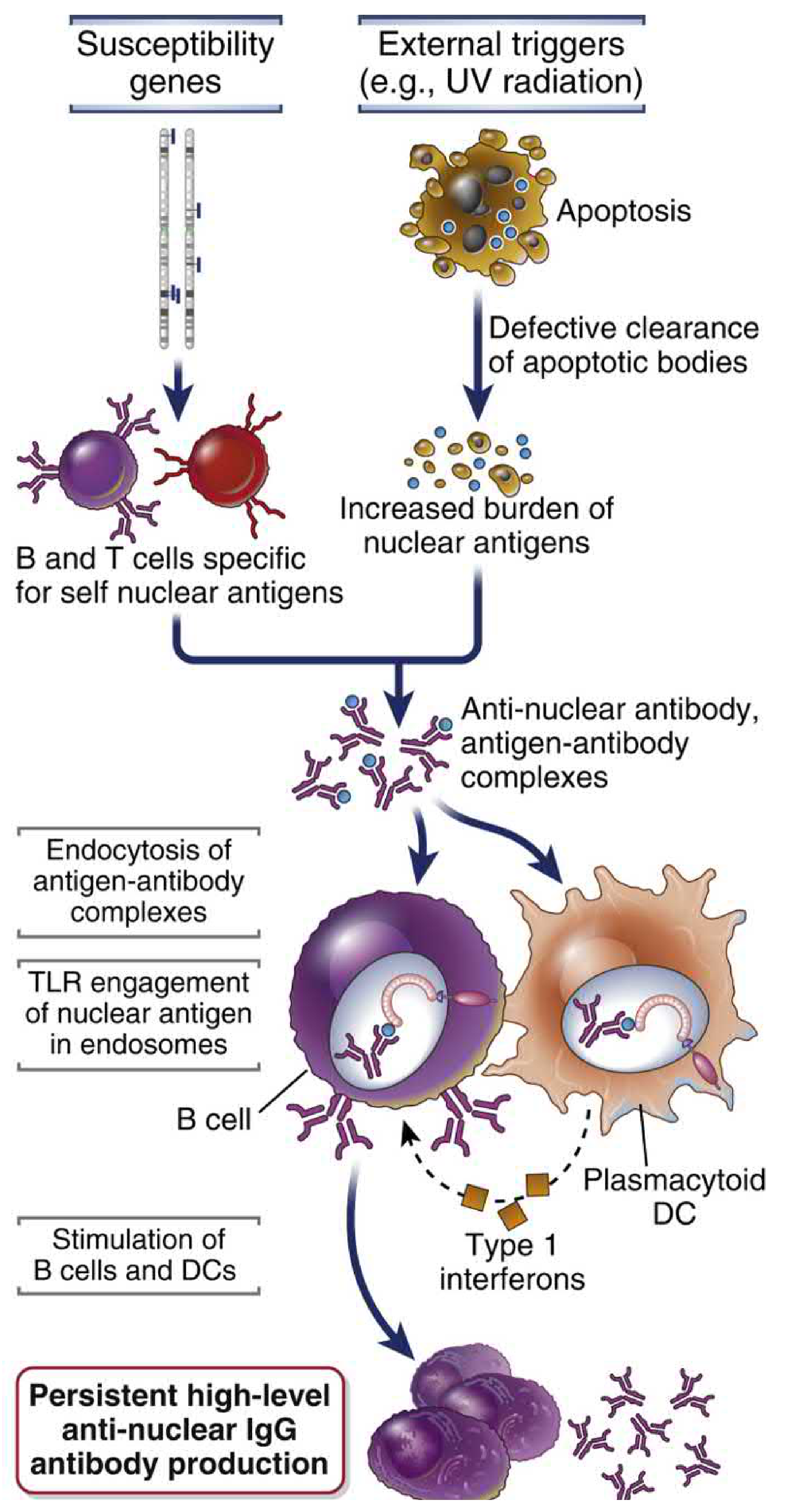
Key Pathogenic Mechanism
- Environmental triggers (especially UV radiation) cause apoptosis of skin cells, releasing nuclear antigens
- Defective clearance of apoptotic bodies (due to complement deficiency, reduced TREX1 nuclease activity) creates a large burden of nuclear antigens
- Self-reactive B and T cells (not deleted due to failed tolerance) are stimulated by these nuclear antigens
- Antigen-antibody complexes form and are endocytosed into DCs and B cells
- Endosomal TLRs (TLR9 recognizes DNA; TLR7 recognizes RNA) are engaged by the nucleic acid components - amplifying B cell activation
- Plasmacytoid DCs are activated and produce IFN-α (type I interferon) - the "interferon signature" found in blood cells of SLE patients
- IFN-α further enhances immune responses and may cause more apoptosis → self-perpetuating cycle
- Net result: Persistent high-level anti-nuclear IgG antibody production and immune complex-mediated tissue injury
- Cellular and Molecular Immunology, p. 1275-1276
3. Autoantibodies in SLE
| Antibody | Frequency in SLE | Clinical Significance |
|---|---|---|
| ANA (antinuclear antibody) | ~99% | Screening test; not specific |
| Anti-dsDNA | ~70% | Highly specific; correlates with disease activity and lupus nephritis |
| Anti-Sm (Smith) | ~38% | Highly specific; associated with worse renal prognosis |
| Anti-Ro (SSA) | ~49% | Neonatal lupus, photosensitivity, Sjogren's overlap |
| Anti-La (SSB) | ~35% | Sjogren's overlap; neonatal heart block |
| Anti-U1-RNP | ~33% | Mixed connective tissue disease overlap |
| Antiphospholipid antibodies (aCL, anti-β2GPI, lupus anticoagulant) | ~21% | Antiphospholipid syndrome: thrombosis, recurrent miscarriage |
| Anti-ribosomal P | ~10% | Neuropsychiatric lupus, psychosis |
- Goldman-Cecil Medicine, p. 2817
4. Clinical Features
SLE can affect virtually any organ. Four of the 11 original ACR criteria are mucocutaneous - skin involvement occurs in 80% of cases.
Mucocutaneous (80%)
- Malar (butterfly) rash: Erythema over malar eminences and nasal bridge, sparing nasolabial folds; triggered/worsened by sun exposure
- Discoid lupus: Scarring, hyperpigmented plaques; can occur without systemic disease
- Subacute cutaneous lupus (SCLE): Annular or papulosquamous non-scarring rash; strongly linked to anti-Ro/La antibodies
- Photosensitivity: Rash or flare after UV exposure
- Oral ulcers: Usually painless (21% of patients)
- Non-scarring alopecia: Diffuse hair loss during flares
- Bullous lupus
Musculoskeletal (>90%)
- Arthritis/arthralgia: Most common presenting symptom; typically non-erosive, non-deforming polyarthritis (unlike RA)
- Jaccoud arthropathy: Reducible deformities from ligamentous laxity
- Myositis: Less common
Renal (50-60%)
- Lupus nephritis (LN): Leading cause of morbidity and mortality
- Presents with proteinuria, hematuria, cellular casts, hypertension, declining GFR
- WHO/ISN classification (Classes I-VI):
- Class I: Normal light microscopy, minimal mesangial deposits
- Class II: Mesangial hypercellularity
- Class III: Focal proliferative GN (<50% glomeruli)
- Class IV: Diffuse proliferative GN (≥50% glomeruli) - most severe, "wire-loop" lesions
- Class V: Membranous LN
- Class VI: Advanced sclerotic
Cardiovascular
- Libman-Sacks endocarditis: Non-bacterial verrucous endocarditis on both surfaces of mitral valve
- Pericarditis / pericardial effusion: Most common cardiac manifestation
- Myocarditis, premature atherosclerosis (major cause of long-term mortality)
- Thrombosis: From antiphospholipid antibodies
Neuropsychiatric (NPSLE)
- Wide spectrum: headache, cognitive dysfunction ("lupus fog"), psychosis, seizures, stroke, transverse myelitis, peripheral neuropathy
- MRI shows white matter lesions, cerebral infarction, venous sinus thrombosis in 19-70% of patients
- Anti-ribosomal P antibodies associated with psychosis
Pulmonary
- Pleuritis/pleural effusion: Most common pulmonary manifestation (exudative)
- Shrinking lung syndrome: Diaphragmatic dysfunction
- Pulmonary hypertension
- Lupus pneumonitis and rarely diffuse alveolar hemorrhage (life-threatening)
Hematologic
- Cytopenias common: hemolytic anemia (Coombs-positive), leukopenia, lymphopenia, thrombocytopenia
- Thrombocytopenia can be from antiphospholipid antibodies or anti-platelet antibodies
Constitutional
- Fever, fatigue, weight loss (often present during flares)
5. Diagnosis
2019 EULAR/ACR Classification Criteria (Score-Based)
Entry criterion: ANA titer ≥1:80 (if absent, do not classify as SLE)
Classify as SLE if total score ≥10 points (within each domain, count only the highest-weighted criterion):
| Domain | Criterion | Points |
|---|---|---|
| Constitutional | Fever | 2 |
| Neuropsychiatric | Delirium | 2 |
| Psychosis | 3 | |
| Seizure | 5 | |
| Mucocutaneous | Non-scarring alopecia | 2 |
| Oral ulcers | 2 | |
| Subacute cutaneous/discoid lupus | 4 | |
| Acute cutaneous lupus (malar rash) | 6 | |
| Musculoskeletal | Joint involvement | 6 |
| Serosal | Pleural/pericardial effusion | 5 |
| Acute pericarditis | 6 | |
| Hematologic | Leukopenia | 3 |
| Thrombocytopenia | 4 | |
| Autoimmune hemolysis | 4 | |
| Renal | Proteinuria >0.5 g/24 h | 4 |
| Renal biopsy class II or V LN | 8 | |
| Renal biopsy class III or IV LN | 10 | |
| Antiphospholipid Abs | aCL or anti-β2GPI | 2 |
| Lupus anticoagulant | 3 | |
| Complement | Low C3 OR low C4 | 3 |
| Low C3 AND low C4 | 4 | |
| SLE-specific Abs | Anti-dsDNA | 6 |
| Anti-Sm | 6 |
Note: The older ACR 11-criterion rule (≥4 criteria = SLE) is also still used clinically. The SLICC criteria require ≥4 criteria (with ≥1 clinical + ≥1 immunologic) OR biopsy-proven LN + ANA or anti-dsDNA.
- Goldman-Cecil Medicine, p. 2817; Andrews' Diseases of the Skin, p. 189
Key Investigations
- ANA (screening) - nearly universal in SLE
- Anti-dsDNA, anti-Sm - confirmation and specificity
- Complement levels (C3, C4): low in active disease (consumed by immune complexes); useful for monitoring activity
- CBC: cytopenias
- Urinalysis with microscopy: proteinuria, RBC casts
- Spot urine protein:creatinine ratio / 24-h urine protein
- Serum creatinine/GFR
- Antiphospholipid antibody panel
- Renal biopsy: mandatory for classification of lupus nephritis and guiding therapy
6. Treatment
2025 ACR / EULAR Treatment Goals
- Achieve low disease activity (SLEDAI score 0-4) or ideally remission (SLEDAI = 0)
- Use minimum prednisone ≤5 mg/day (or equivalent) for maintenance
- Minimize organ damage and treatment-related complications
- Prevent flares
The 2025 ACR SLE Guideline (the first ACR lupus guideline since 1999) was released November 2025 and provides updated evidence-based recommendations.
Step 1 - Universal Measures (ALL SLE patients)
- Daily sunscreen on sun-exposed areas (avoid UV triggers)
- Avoid smoking (interferes with antimalarial efficacy)
- Regular exercise, healthy diet, BP/lipid/glucose control
- Vaccination (avoid live vaccines if immunosuppressed)
- Hydroxychloroquine (HCQ) in ALL patients unless contraindicated
Step 2 - Hydroxychloroquine (Cornerstone Therapy)
- Dose: up to 5 mg/kg/day (actual body weight); typically 200-400 mg/day
- Benefits: prevents flares, reduces overall mortality, decreases renal disease and accelerated atherosclerosis, anti-thrombotic effects, improves fatigue, safe in pregnancy
- Monitoring: Baseline ophthalmologic exam + annual eye exams (macular toxicity with prolonged use)
- Tobacco smoking reduces antimalarial efficacy
Step 3 - Disease Severity-Based Treatment (Non-Renal)
| Severity | First-Line | Second-Line / Add-On |
|---|---|---|
| Mild (constitutional, mild arthritis, rash, SLEDAI ≤6) | HCQ ± low-dose steroids | MTX or AZA or MMF |
| Moderate (significant arthritis, rash, serositis) | HCQ + glucocorticoids + MTX/AZA/MMF | Belimumab or anifrolumab |
| Severe (NPSLE, vasculitis, significant cytopenias) | High-dose glucocorticoids + CYC or MMF | Rituximab (off-label) |
- Harrison's Principles of Internal Medicine 22E (2025), EULAR recommendations
Step 4 - Lupus Nephritis Treatment (ISN Class III/IV)
- Induction: High-dose corticosteroids + mycophenolate mofetil (MMF) (preferred over cyclophosphamide in most patients) OR cyclophosphamide (NIH regimen or Euro-Lupus low-dose)
- Adjunct: Belimumab (BLISS-LN trial: improved renal response when added to standard therapy)
- Maintenance: MMF or azathioprine (AZA) + HCQ
- Membranous LN (Class V): MMF or calcineurin inhibitors (voclosporin, tacrolimus)
Biologic Agents
| Drug | Target | Indication |
|---|---|---|
| Belimumab (Benlysta) | BAFF (B cell-activating factor) | Moderate-severe SLE; lupus nephritis (IV formulation) |
| Anifrolumab (Saphnelo) | IFN-α/β receptor (IFNAR1) | Moderate-severe non-renal SLE; approved 2021 |
| Voclosporin (Lupkynis) | Calcineurin inhibitor | Lupus nephritis Class III/IV/V (approved 2021) |
| Rituximab | CD20 (B cell depletion) | Refractory SLE, severe NPSLE (off-label) |
Note on anti-IFN-α therapy: Despite IFN-α being central to SLE pathogenesis, anti-IFN-α antibodies had disappointing clinical trials. However, anifrolumab (blocking the IFN-α/β receptor) has shown efficacy and is now approved. - Cellular and Molecular Immunology, p. 1276
Pregnancy Considerations (EULAR 2025)
- Safe to continue: HCQ, low-dose steroids, AZA, calcineurin inhibitors
- Discontinue: Mycophenolate, cyclophosphamide, methotrexate (teratogenic)
- Belimumab: EULAR 2025 allows use if no pregnancy-compatible medication controls disease; no data on anifrolumab in pregnancy
- Antiphospholipid antibody-positive patients: aspirin ± LMWH during pregnancy
7. Complications & Prognosis
| Short-term Risks | Long-term Risks |
|---|---|
| Lupus nephritis (ESKD) | Premature atherosclerosis (CVD - major cause of death) |
| Diffuse alveolar hemorrhage | Avascular necrosis (from steroids) |
| Thrombosis (APS) | Osteoporosis |
| Serious infection (immunosuppression) | Malignancy (especially lymphoma; increased with cyclophosphamide) |
| Catastrophic APS | Cognitive decline, chronic pain |
| Neonatal lupus / congenital heart block (anti-Ro/La) | Organ damage accumulation |
- Flare triggers: UV light, infections, pregnancy, certain drugs (procainamide, hydralazine, isoniazid cause drug-induced lupus)
- 10-year survival now >90% in high-resource settings; prognosis worsened by renal involvement, NPSLE, antiphospholipid syndrome, delayed diagnosis
8. Drug-Induced Lupus
Drugs that commonly cause lupus-like syndrome:
- Procainamide (highest risk), hydralazine, isoniazid, minocycline, anti-TNF agents
- Usually associated with anti-histone antibodies (positive in ~95%)
- Typically anti-dsDNA negative (distinguishes from idiopathic SLE)
- Resolves after stopping the offending drug
9. Monitoring Disease Activity
- SLEDAI (SLE Disease Activity Index) - most widely used scoring tool
- BILAG (British Isles Lupus Assessment Group)
- Key monitoring labs: anti-dsDNA titers, C3/C4 levels, CBC, urine protein - correlate with disease activity
- High anti-dsDNA + low complement = active disease / impending flare
Quick Mnemonic - SOAP BRAIN MD (ACR criteria):
- Serositis, Oral ulcers, Arthritis, Photosensitivity
- Blood disorders (hemolytic anemia, leukopenia, thrombocytopenia), Renal (proteinuria/casts), ANA, Immunologic (anti-dsDNA, anti-Sm, aPL)
- Neurologic (seizures/psychosis), Malar rash, Discoid rash
2025 Updates: The ACR released its first SLE guideline since 1999 in November 2025. The EULAR 2025 guidelines added recommendations for anifrolumab and belimumab use in pregnancy (with restrictions). The 2024 ACR Lupus Nephritis guideline updated treatment algorithms with voclosporin and belimumab as part of standard induction therapy. EULAR 2025 also updated recommendations for lupus nephritis management incorporating evidence from newer biologics.
This is a shared conversation. Sign in to Orris to start your own chat.