Torticollis vs Wry neck
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough answer.
Torticollis (Wry Neck)
Torticollis and wry neck are the same condition. "Torticollis" comes from the Latin tortus (twisted) + collum (neck); "wry neck" is simply its English common name. The terms are interchangeable in clinical literature.
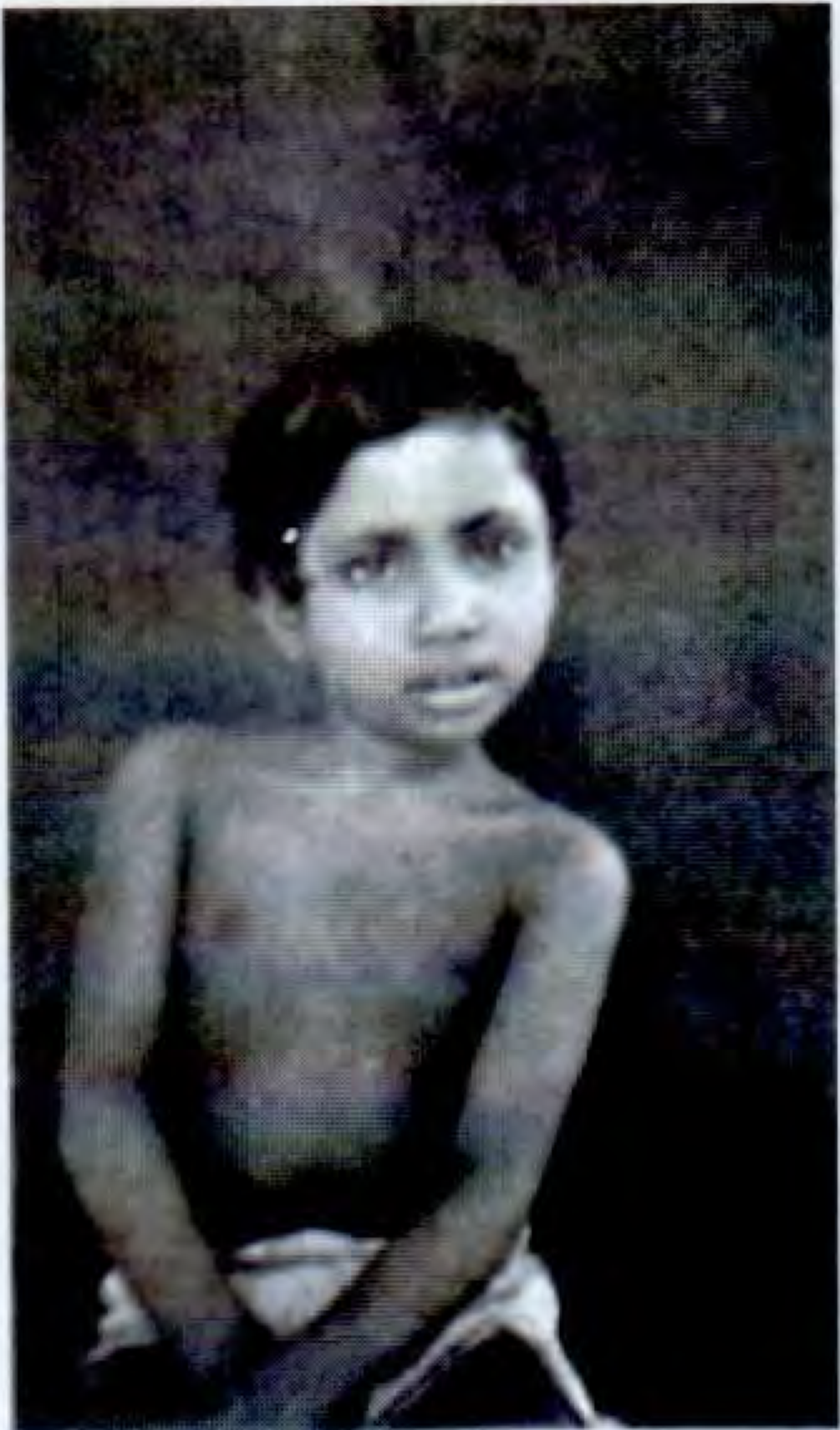
Clinical appearance of torticollis - S Das: A Manual on Clinical Surgery, 13th Ed
Definition
Torticollis is a deformity in which the head is bent (tilted) to one side while the chin points to the opposite side, due to contraction or spasm of the sternocleidomastoid (SCM) muscle and adjacent cervical muscles. In the head, the SCM tilts to its own side and rotates to the contralateral side.
- Bailey and Love's Short Practice of Surgery, 28th Ed: "In torticollis the head is tilted towards and rotated away from the tight sternocleidomastoid muscle."
Classification and Types
| Type | Key Features |
|---|---|
| Congenital | Birth/intrauterine origin; SCM fibrosis/tumour; most common |
| Traumatic | Fracture-dislocation of the cervical spine |
| Rheumatic | Sudden onset after cold/draught exposure |
| Inflammatory | Inflamed cervical lymph nodes (e.g., Grisel syndrome) |
| Spasmodic (Dystonic) | Idiopathic cervical dystonia; adult-onset; neurological |
| Compensatory | Secondary to scoliosis, ocular problems (ocular torticollis) |
| Pott's disease | Tuberculosis of the cervical spine |
| Contracture | Post-burn, post-ulcer scarring |
| Paroxysmal | Benign paroxysmal torticollis (associated with migraine/BPV in children) |
1. Congenital Muscular Torticollis (CMT)
The most common form, presenting in infancy.
Pathogenesis
- Fibrosis of the SCM muscle, resulting in a palpable "tumour" (sternomastoid tumour)
- Histologically: collagen and fibroblast deposition around atrophied muscle cells (Schwartz's Principles of Surgery)
- Proposed causes: malposition/intrauterine constraint, birth trauma (tearing of SCM fibers with haematoma formation), intrauterine compartment syndrome, vascular injury, primary SCM myopathy
- Also occurs in C-section deliveries, confirming intrauterine factors
Clinical Features
- Head tilted toward the affected (tight) SCM, chin rotated away
- Palpable firm/rigid mass in the muscle in ~2/3 of cases
- In long-standing cases: facial hemiatrophy on the affected side (smaller eye-to-mouth distance, flattened nose, less arched eyebrow, less full cheek - due to impaired vascular supply from restricted mobility)
Investigations
- Diagnosis usually clinical (characteristic fibrotic nodule)
- USS: evaluates SCM thickness and predicts need for surgery; useful in management
- Cervical spine X-ray: if congenital vertebral anomaly suspected
- MRI: if neurological findings present
Treatment
Non-operative (first-line):
- Stretching exercises during infancy
- Early intervention (before 3-4 months) achieves 92-100% full passive neck rotation; only ~1% need surgery
- For every month treatment is delayed, surgical risk increases
- Established facial asymmetry or >30° motion restriction at start of treatment predicts a poor outcome
- If CMT persists beyond 1 year, non-operative treatment is rarely successful
Surgical:
- Release of SCM origin and/or insertion
- Indicated when non-operative treatment fails or if significant restriction persists
- Campbell's Operative Orthopaedics (2026): surgery for neglected cases improves health-related quality of life; botulinum toxin combined with PT may help resistant cases
2. Spasmodic Torticollis (Idiopathic Cervical Dystonia)
A neurological form, distinct from congenital/mechanical types.
Features
- Most frequent form of focal (restricted) dystonia
- Onset: early to middle adult life; slightly more common in women (peak 5th decade)
- Usually idiopathic; rare DYT1 gene abnormality in some patients
- Quality of movement: intermittent turning/tilting, smooth or jerky, or sustained deviation to one side
- Often accompanied by irregular high-frequency tremor
- Gestes antagonistes ("sensory tricks"): placing a hand on the chin/neck, counterpressure, or resting occiput on a high-backed chair reduces spasms (becomes less effective over time)
- Spasms worse on standing/walking; reduced when lying down
- Chronic cases: muscle hypertrophy and pain
- Muscles affected: SCM, levator scapulae, trapezius, posterior cervical muscles bilaterally
- ~15% also have oral/mandibular/hand dystonia; ~10% have blepharospasm
Treatment (Adams and Victor's Principles of Neurology, 12th Ed)
| Modality | Notes |
|---|---|
| Botulinum toxin | Injection every 3-6 months into affected muscles (guided by palpation + EMG); ~90% response rate; first-line |
| Anticholinergics | Trihexyphenidyl/benztropine - partial relief; poorly tolerated at effective doses |
| Deep brain stimulation (DBS) | Globus pallidus interna or subthalamic nucleus; for refractory cases; some adverse effects (dysarthria, dyskinesia) |
| Surgical denervation | Combined sectioning of spinal accessory nerve + first 3 cervical motor roots (bilateral); reserved for severe refractory cases; 1/3 to 1/2 long-term relief |
| Spontaneous remission | Occurs in 10-20% (usually early-onset cases); nearly all relapse within 5 years |
Key Comparison: Congenital vs Spasmodic Torticollis
| Feature | Congenital Muscular | Spasmodic (Dystonic) |
|---|---|---|
| Age of onset | Birth/infancy | Adult (peak 5th decade) |
| Cause | SCM fibrosis/trauma | Idiopathic cervical dystonia |
| SCM finding | Firm palpable mass | Muscle hypertrophy (late) |
| Movement quality | Fixed positional deformity | Intermittent, jerky, or sustained |
| Sensory trick | Absent | Present (geste antagoniste) |
| Facial asymmetry | Yes (long-standing) | No |
| First-line treatment | Physiotherapy/stretching | Botulinum toxin |
| Surgery | SCM release | DBS / nerve sectioning (refractory) |
Sources:
- S Das: A Manual on Clinical Surgery, 13th Ed, pp. 377-378
- Bailey and Love's Short Practice of Surgery, 28th Ed
- Schwartz's Principles of Surgery, 11th Ed
- Campbell's Operative Orthopaedics, 15th Ed (2026)
- Adams and Victor's Principles of Neurology, 12th Ed, pp. 109-111
- The Developing Human - Clinically Oriented Embryology
This is a shared conversation. Sign in to Orris to start your own chat.