Medial leminiscus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of the medial lemniscus based on authoritative neuroanatomy textbooks.
Medial Lemniscus
Overview
The medial lemniscus (ML) is the major second-order sensory tract of the dorsal column-medial lemniscal (DCML) pathway. It carries fine touch, vibration, proprioception, and kinesthesia from the contralateral body to the thalamus. The name comes from the Latin lemniscus meaning "ribbon" - an apt description of its flat, ribbon-like shape in brainstem cross sections.
The Complete Pathway (3-Neuron Arc)
Neuron 1 - Primary Sensory Neuron (Periphery → Medulla)
- Receptors: Meissner's corpuscles (light touch), Merkel discs (pressure/vibration 5-15 Hz), Pacinian corpuscles (vibration 200-300 Hz), Ruffini endings (stretch), muscle spindles/Golgi tendon organs (proprioception)
- Fiber type: Large-diameter, heavily myelinated A-alpha and A-beta fibers
- Cell body: Dorsal root ganglion (DRG)
- Course: Enters spinal cord via the medial dorsal root entry zone → ascends ipsilaterally in the posterior (dorsal) columns
- Fasciculus gracilis (medial): legs, lower trunk (below ~T6)
- Fasciculus cuneatus (lateral): upper trunk, arms, neck (above T6)
- 1st synapse: Nucleus gracilis and nucleus cuneatus in the caudal medulla
Neuron 2 - Second-Order Neuron (Medulla → Thalamus)
- Origin: Nucleus gracilis and nucleus cuneatus
- Decussation: Axons sweep ventrally and medially as internal arcuate fibers, crossing the midline at the lower/caudal medulla
- Formation of the medial lemniscus: After crossing, fibers aggregate into the medial lemniscus on the contralateral side
- Course through the brainstem:
- Medulla: Vertical orientation, immediately dorsal to the pyramidal (corticospinal) tract, adjacent to the midline. Gracile fibers ventrolaterally, cuneate fibers dorsomedially
- Pons: Moves dorsolaterally, now horizontal in orientation
- Midbrain: Located in the tegmentum, lateral to the red nucleus
- 2nd synapse: Ventral posterolateral (VPL) nucleus of the thalamus
Additional input: The lateral cervical nucleus (LCN, C1-C2) and nucleus Z also send fibers to join the medial lemniscus. The face equivalent - the trigeminal lemniscus - runs in parallel and terminates in the VPM (ventral posteromedial) nucleus.
Neuron 3 - Thalamocortical Neuron (Thalamus → Cortex)
- From the VPL, axons pass through the posterior limb of the internal capsule (thalamic somatosensory radiations)
- Terminate in primary somatosensory cortex (S1), postcentral gyrus (Brodmann areas 3, 1, 2)
Somatotopic Organization
The ML maintains a precise somatotopic map throughout its course, but its orientation rotates as it ascends:
| Level | Orientation | Legs | Arms |
|---|---|---|---|
| Medulla | Vertical ("person stands up") | Ventral/lateral | Dorsal/medial |
| Pons/Midbrain | Horizontal ("person lies down") | Lateral | Medial |
This is the reverse of the posterior columns (where legs are medial). A useful mnemonic: the somatotopic map flips orientation when the ML rotates from its vertical medullary position into its horizontal pontine position.
Diagram - Dorsal Column-Medial Lemniscal Pathway
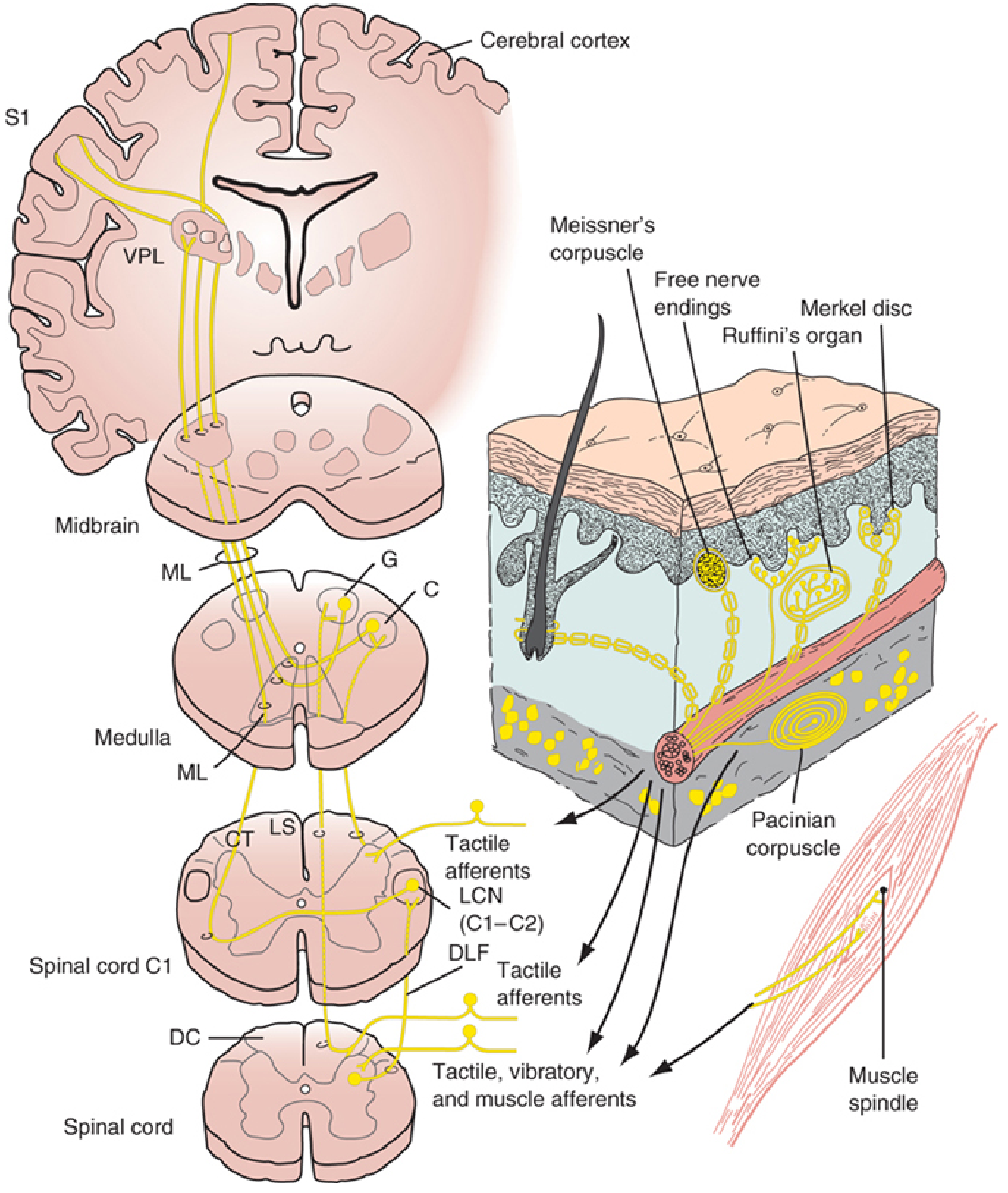
Figure: Central pathways of the DCML system. ML = medial lemniscus; G = nucleus gracilis; C = nucleus cuneatus; VPL = ventral posterolateral nucleus; S1 = primary somatosensory cortex; DC = dorsal columns; DLF = dorsolateral funiculus; LCN = lateral cervical nucleus. (From Localization in Clinical Neurology, 8e)
Blood Supply
The vascular supply of the ML varies by level and is clinically important:
| Level | Artery | Clinical Syndrome |
|---|---|---|
| Medulla | Anterior spinal artery (paramedian branches) | Medial medullary (Dejerine) syndrome |
| Pons | Paramedian branches of basilar artery | Pontine infarct |
| Midbrain | Paramedian branches of basilar / PCA | Weber or Claude syndrome |
Clinical Correlations
Lesion of the Medial Lemniscus
A pure ML lesion produces contralateral loss of:
- Vibration sense
- Joint position sense (proprioception)
- Discriminative (two-point) touch
- Stereognosis and graphesthesia
Pain and temperature are spared (they travel in the spinothalamic tract, which is laterally located and has a different blood supply).
Key Syndromes
Medial Medullary (Dejerine) Syndrome - anterior spinal artery occlusion:
- Contralateral loss of position/vibration sense (ML involvement)
- Contralateral hemiparesis (pyramidal tract)
- Ipsilateral CN XII palsy (hypoglossal nucleus/fibers)
- Pain and temperature spared (lateral spinothalamic tract unaffected)
Lateral Medullary (Wallenberg) Syndrome - PICA occlusion:
- ML spared (laterally located structures affected)
- Contralateral pain/temperature loss (spinothalamic tract)
- Ipsilateral face pain/temperature loss (spinal trigeminal nucleus/tract)
Thalamic (VPL) Lesion:
- Contralateral loss of all sensory modalities (face + body) including pain, temperature, touch, vibration, and proprioception
Brown-Sequard Syndrome (hemicord lesion):
- Ipsilateral loss of proprioception/vibration below the lesion (posterior column not yet crossed)
- Contralateral pain/temperature loss below the lesion (spinothalamic, already crossed)
Comparison: DCML vs. Spinothalamic Tract
| Feature | Dorsal Column-ML | Spinothalamic |
|---|---|---|
| Modalities | Fine touch, vibration, proprioception | Pain, temperature, crude touch |
| Where it crosses | Caudal medulla | At each spinal cord level (within 1-2 segments) |
| Brainstem position | Medial/paramedian | Lateral tegmentum |
| Thalamic relay | VPL | VPL (separate neurons) + intralaminar nuclei |
| Fiber type | A-alpha, A-beta (large, myelinated) | A-delta, C (small, thinly/unmyelinated) |
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld); Localization in Clinical Neurology, 8e; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.