Ascent of kidney embryology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from both Langman's Medical Embryology and Campbell-Walsh Urology. Let me compile the full answer.
Ascent of the Kidney - Embryology
Overview
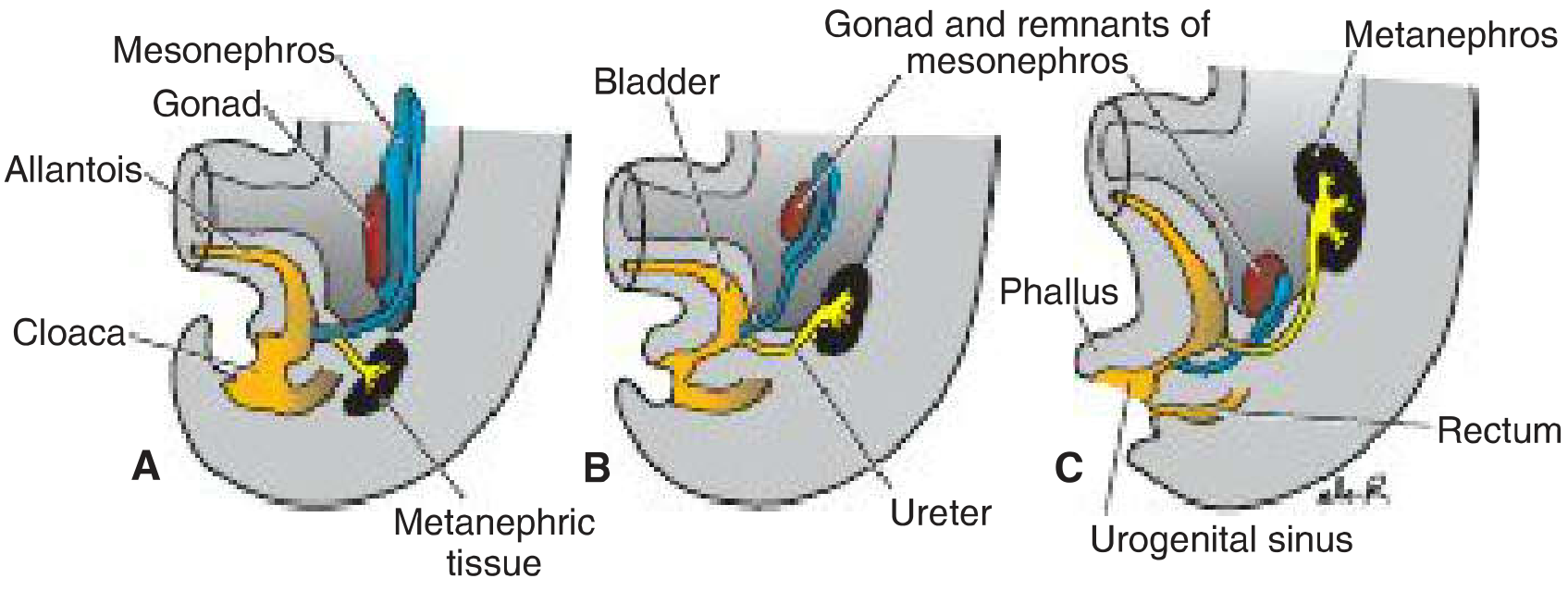
The permanent kidney (metanephros) initially develops in the pelvic region and subsequently migrates to its adult position in the upper lumbar retroperitoneum, just below the adrenal glands. This entire process is completed between weeks 6 and 9 of gestation.
The Three Embryonic Kidneys (Context)
There are three successive kidney systems:
- Pronephros - rudimentary, non-functional, disappears
- Mesonephros - functional briefly; largely degenerates (remnants associate with the gonad)
- Metanephros - the permanent kidney, formed from week 5
How Ascent Occurs
The ureteric bud (UB) arises from the Wolffian (mesonephric) duct at the end of week 4, grows cranially into the urogenital ridge, and acquires a cap of metanephric blastema by week 5. This combined unit then:
- Migrates cephalad (upward) from the sacral/pelvic region to the lumbar retroperitoneum
- Rotates medially ~90° on its long axis (the hilum, which initially faces ventrally, rotates to face medially)
The mechanism of ascent is not fully understood, but the main drivers are:
- Diminution of body curvature (straightening of the embryo)
- Differential growth of the lumbar and sacral regions of the embryo
"This ascent of the kidney is caused by diminution of body curvature and by growth of the body in the lumbar and sacral regions." - Langman's Medical Embryology
Changing Vascular Supply During Ascent
As the kidney ascends from the pelvis cranially into the upper lumbar region, it is vascularized by a succession of transient aortic sprouts arising at progressively higher levels:
- These arteries do not elongate to follow the kidney - they degenerate and are replaced by new, higher-level arteries
- The final (highest) pair of arteries becomes the definitive renal arteries
- Occasionally, a more inferior pair persists as accessory lower-pole arteries - these cross ventral to the ureter and can cause intermittent ureteropelvic junction (UPJ) obstruction
- This embryonic vascular variability explains why ~25% of adult kidneys have two or more renal arteries
Anomalies of Renal Ascent
1. Pelvic Kidney (Renal Ectopia)
- The kidney fails to ascend from its pelvic origin
- Incidence: ~1 in 900 (range 1:500 to 1:1200); slightly more common on the left
- Classification by position: pelvic (most common - lies opposite the sacrum) > iliac > abdominal > thoracic
- The ectopic kidney still rotates if it ascends partially, but malrotation may also occur
- Vascular supply is anomalous - may arise from distal aorta, aortic bifurcation, common/external iliac, or inferior mesenteric artery
- Associated anomalies:
- Vesicoureteral reflux in 30-50% of cases
- Genital anomalies in 15-45%: bicornuate/absent uterus, vaginal duplications (females); undescended testes, hypospadias (males)
- Skeletal and cardiac anomalies in ~14%
- The adrenal gland is NOT displaced - it develops independently of the kidney
2. Horseshoe Kidney (~1:500)
- The inferior poles of both kidneys fuse across the midline before ascent is complete
- The fused lower pole (isthmus) is arrested by the inferior mesenteric artery during ascent - it cannot pass beneath this vessel
- The kidneys therefore remain lower than normal (typically at L3-L5)
- Usually asymptomatic but associated with a slight increase in:
- UPJ obstruction
- Renal calculi
- Increased risk of renal trauma (less protected position)
3. Cross-fused Ectopia (Rare)
- One kidney fuses to the contralateral one and ascends to the opposite side
- Both kidneys are on the same side of the body
4. Incomplete Ascent (Renal Ectopia)
- The kidney may halt at any level of its ascent from the pelvis: pelvic, lumbar, or abdominal positions are all described
Summary Table
| Feature | Normal | Pelvic Kidney | Horseshoe Kidney |
|---|---|---|---|
| Timing of completion | Weeks 6-9 | Arrested early | Arrested at IMA |
| Final position | L1-L2 retroperitoneum | Opposite sacrum | L3-L5 (below IMA) |
| Rotation | Medial (hilum faces medially) | Incomplete | Incomplete |
| Blood supply | Definitive renal arteries from aorta | Anomalous (iliac/IMA branches) | Anomalous |
| Adrenal position | Normal | Normal (develops independently) | Normal |
Sources:
- Langman's Medical Embryology - "Position of the Kidney" (p. 282)
- Campbell-Walsh-Wein Urology - "Clinical Correlation: Ascent Anomalies" (p. 449) and "Anomalies of Renal Ascent" (p. 934-935)
This is a shared conversation. Sign in to Orris to start your own chat.