Goniogram of angle closure glaucoma for exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Loading Image
I now have all the content needed for a comprehensive exam answer. Here is the full breakdown:
Gonioscopy (Goniogram) in Angle Closure Glaucoma
What is a Goniogram?
A goniogram is the schematic record of gonioscopic findings - a drawing/diagram of the anterior chamber angle as seen through a gonioscope. For exams, you must know the normal angle structures, grading systems, and the specific findings in angle closure.
Normal Angle Structures (Anterior to Posterior)
When you look into the angle from front to back, the structures you see are:
| Structure | Landmark Significance |
|---|---|
| Schwalbe line | Peripheral edge of Descemet membrane; most anterior |
| Trabecular meshwork (non-pigmented, then pigmented) | Aqueous drainage site |
| Scleral spur | White band; landmark between TM and ciliary body |
| Ciliary body band | Grey/dark; most posterior visible structure |
| Iris root | Inserts at various levels |
Angle Grading - Shaffer System (Most Exam-Tested)
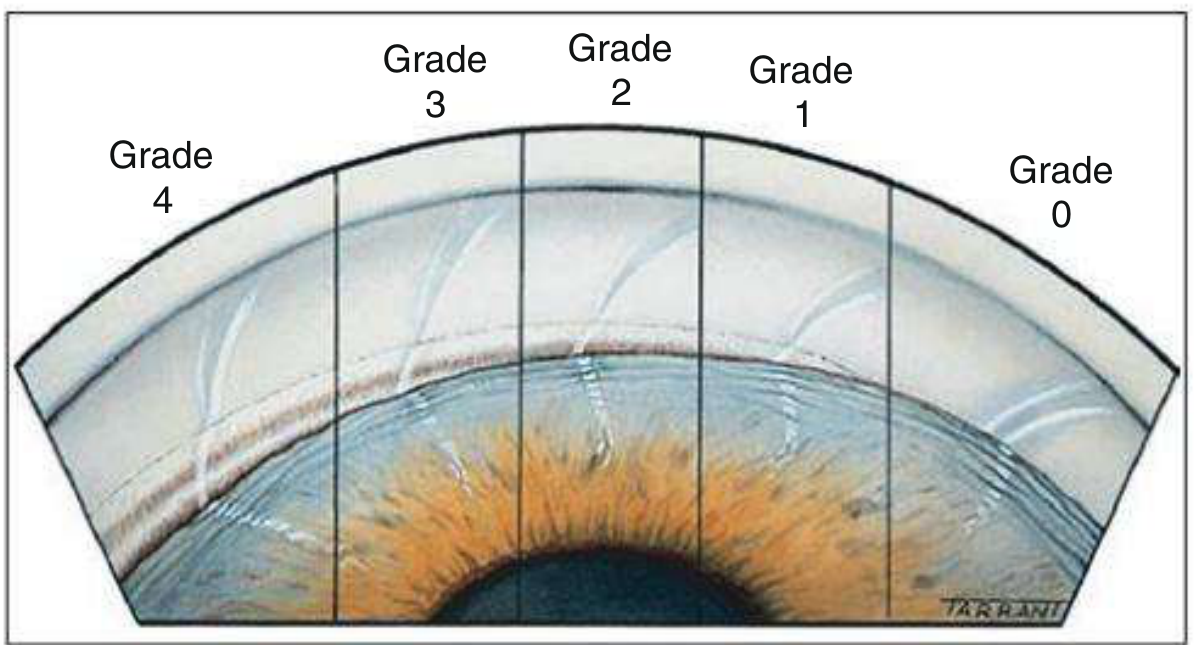
Fig. 11.31 - Shaffer grade 4 (widest) to grade 0 (closed) - Kanski's Clinical Ophthalmology
| Grade | Angle | Structures Visible | Clinical Meaning |
|---|---|---|---|
| 4 | 35-45° | Ciliary body visible | Widest; seen in myopia/pseudophakia |
| 3 | 25-35° | Scleral spur visible | Open; cannot close |
| 2 | 20° | Trabecular meshwork only (no scleral spur) | Possible closure |
| 1 | 10° | Schwalbe line + top of TM only | Dangerously narrow |
| Slit | ~5° | No contact, no structures | Pre-closure |
| 0 | 0° | Iridocorneal contact - CLOSED | Angle closure |
Exam rule: Grades 0-1 = occludable/closed. Grade 2 = needs gonioscopy regularly. Grades 3-4 = safe.
Angle Closure Gonioscopy Findings - Stage by Stage
1. Primary Angle Closure Suspect (PACS)
- Iridotrabecular contact (ITC) in ≥3 quadrants
- No PAS (peripheral anterior synechiae)
- Normal IOP, disc, and visual field
- Eclipse sign on oblique illumination (crescentic shadow on nasal iris)
2. Primary Angle Closure (PAC)
- ITC in ≥3 quadrants
- PAS present and/or raised IOP
- Normal optic disc and visual field
- Best evaluated with indentation gonioscopy
3. Primary Angle Closure Glaucoma (PACG)
- ITC in ≥3 quadrants
- Glaucomatous optic neuropathy present
- Visual field defects
The Critical Finding: Peripheral Anterior Synechiae (PAS)
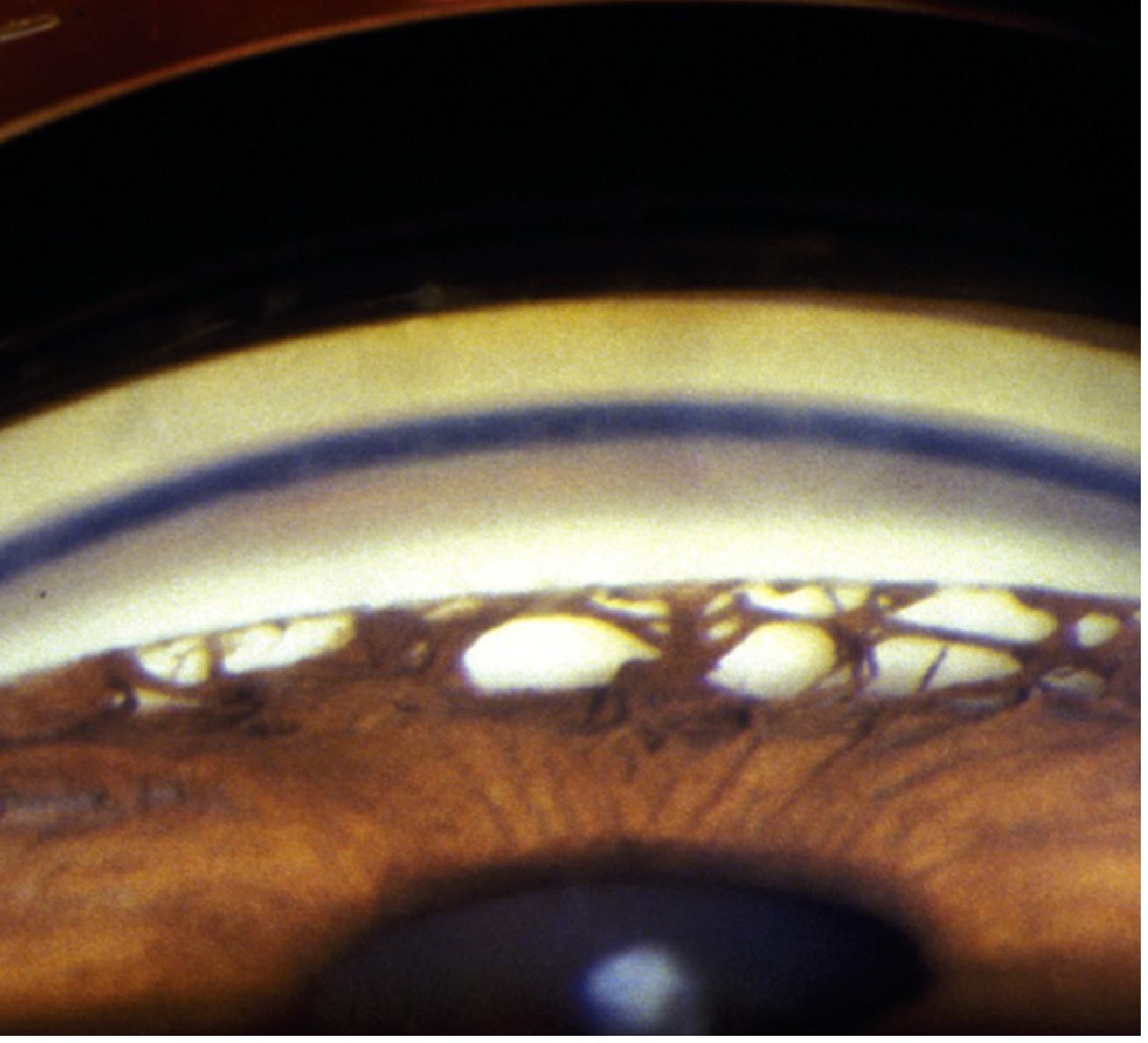
Gonioscopy in chronic angle closure glaucoma - broad bands of PAS visible, blocking the underlying trabecular meshwork - Wills Eye Manual
PAS = permanent adhesions between peripheral iris and trabecular meshwork/cornea.
- In acute angle closure: angle is closed by appositional iris contact (reversible with indentation)
- In chronic angle closure: PAS are present - the angle stays closed even on indentation
- Saw-tooth/pyramidal PAS = intermittent iridotrabecular contact
- Broad flat PAS = prolonged/chronic closure
Indentation (Dynamic) Gonioscopy - The Key Differentiator
| Finding on Indentation | Meaning |
|---|---|
| Angle opens on indentation | Appositional closure - iris pushed back by aqueous, no permanent adhesion |
| Angle remains closed | Synechial closure - PAS present |
- Technique: Zeiss/Posner/Sussman 4-mirror lens pressed gently onto cornea, forcing aqueous into angle
- This is the gold standard to distinguish appositional from synechial closure
Van Herick Method (Slit Lamp Screening - No Gonioscopy Needed)
| AC Depth : Corneal Thickness Ratio | Grade | Action |
|---|---|---|
| ≥1 | 4 | Wide open |
| 1/4 - 1/2 | 3 | Incapable of closure |
| 1/4 | 2 | Perform gonioscopy |
| <1/4 | 1 | Gonioscopy shows dangerously narrow angle |
Clinical Picture: Acute Angle Closure
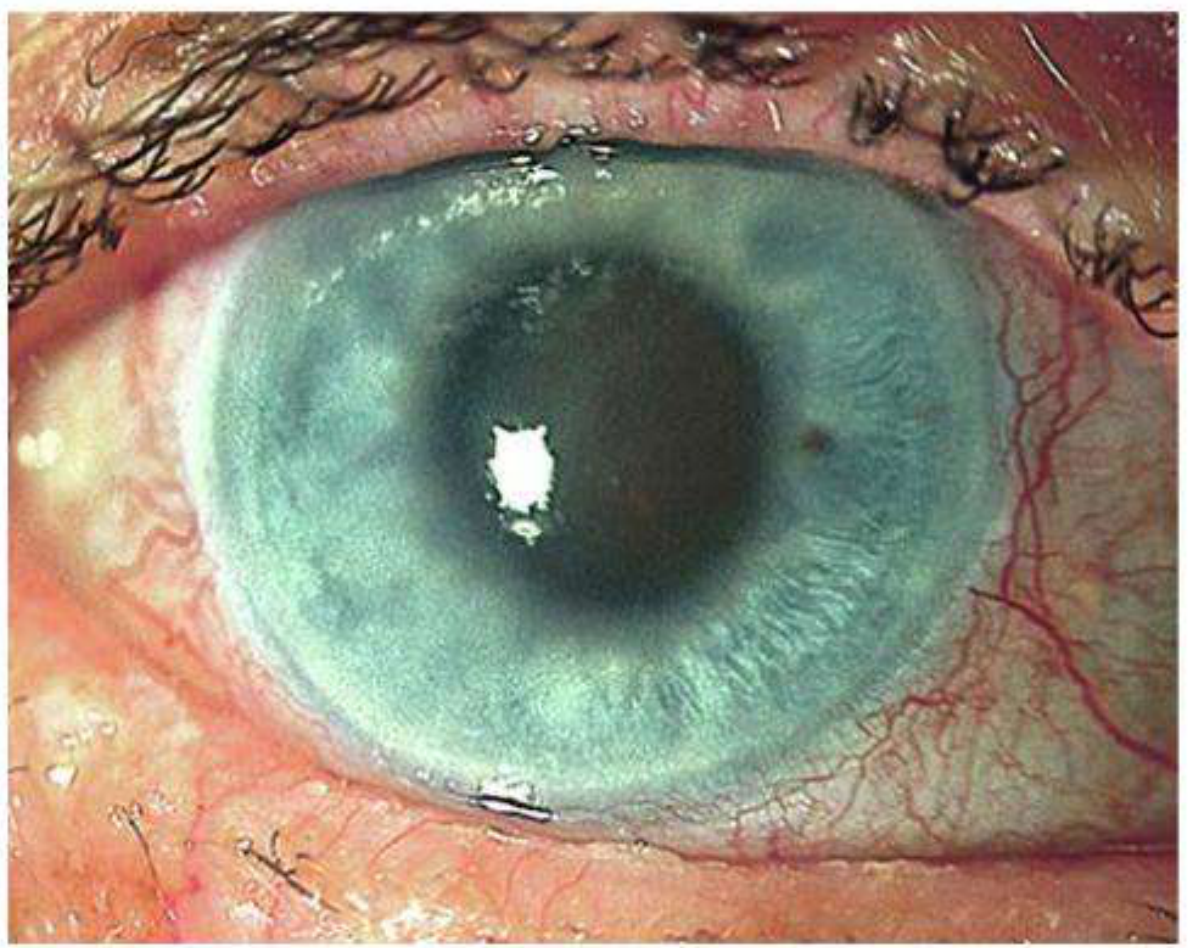
Fig. 11.36 - Acute primary angle closure: corneal edema, mid-dilated vertically oval fixed pupil - Kanski's
Gonioscopy in acute attack shows:
- Completely closed angle in all quadrants (Grade 0)
- No angle structures visible
- High IOP (50-80 mmHg)
- After resolution: PAS, glaukomflecken on lens, spiral iris atrophy
Post-Acute Resolved APAC (Slit Lamp Signs - Exam Favourites)
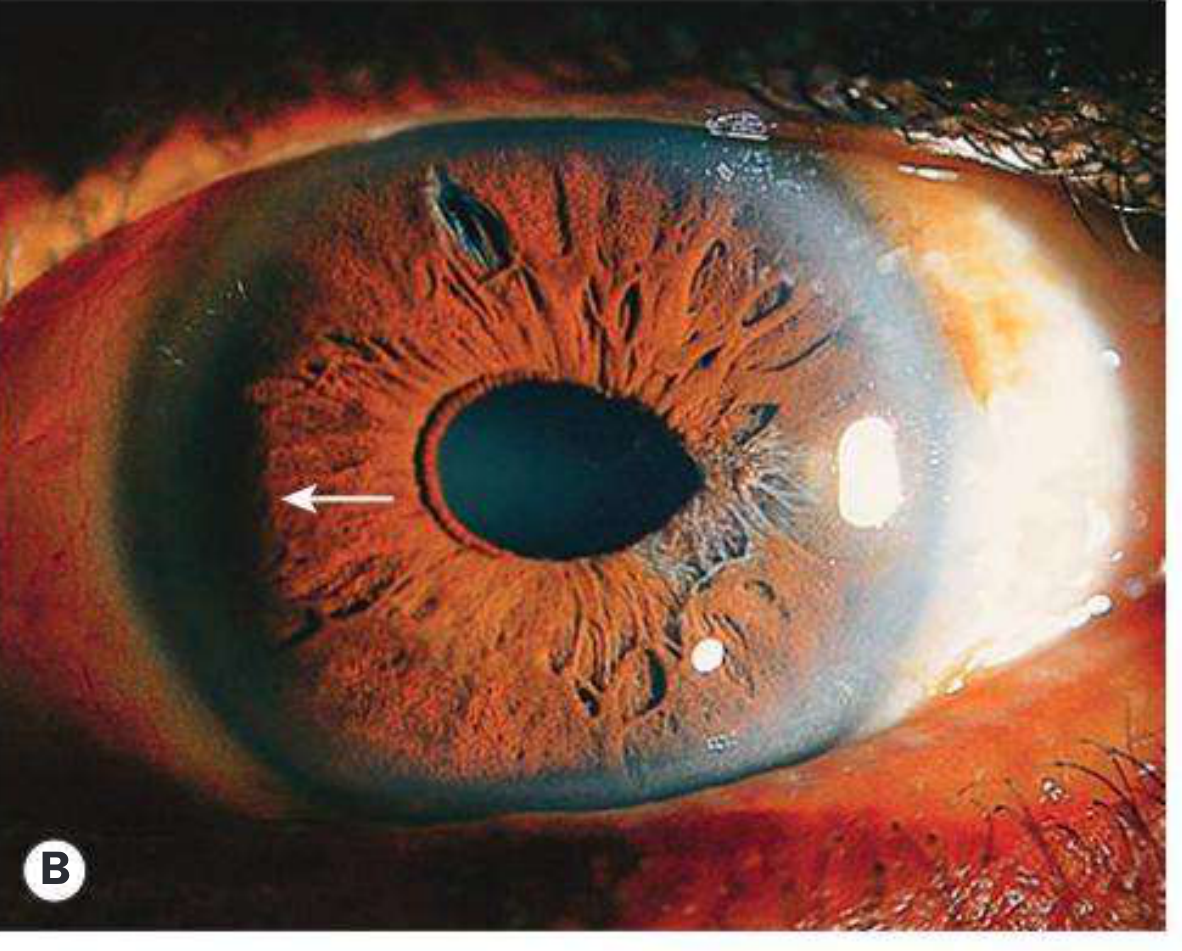
Fig. 11.32B - Iris changes (patent laser iridotomy visible) and glaukomflecken after resolved APAC - Kanski's
- Glaukomflecken: white foci of lens epithelial necrosis (anterior subcapsular) - pathognomonic of past APAC
- Spiral iris atrophy - ischaemic iris changes
- PAS on gonioscopy - marker of previous acute or chronic closure
Mechanism of Angle Closure (Exam Levels)
Relative Pupillary Block (Most Common)
- Aqueous flow through pupil is impaired
- Pressure builds in posterior chamber
- Peripheral iris bows anteriorly (iris bombe)
- Peripheral iris occludes trabecular meshwork
- Relieved by: Laser peripheral iridotomy (LPI)
Plateau Iris
- Ciliary body processes are anteriorly rotated
- Peripheral iris is pushed into the angle even after LPI
- Confirmed by ultrasound biomicroscopy (UBM)
Others (Secondary)
- Phacomorphic (swollen lens)
- Neovascular glaucoma (fibrovascular membrane - PAS)
- Posterior synechiae 360° (seclusio pupillae) - iris bombe
- Malignant glaucoma (aqueous misdirection/ciliolenticular block)
Key Exam Points Summary
| Point | Answer |
|---|---|
| Most important gonioscopy finding in angle closure | ITC (iridotrabecular contact) and PAS |
| How to distinguish appositional vs synechial closure | Indentation gonioscopy |
| Angle grade in acute angle closure | Grade 0 (Shaffer) |
| Pathognomonic sign of past APAC on lens | Glaukomflecken |
| Treatment to break pupillary block | Laser peripheral iridotomy (LPI) |
| Best investigation when plateau iris suspected | Ultrasound biomicroscopy (UBM) |
| Laser contraindicated in chronic angle closure | Laser trabeculoplasty (LT) |
| Risk factors for PACG | Female, hypermetropia, Asian race, age ~62 yrs, short axial length |
| The "eclipse sign" | Crescentic shadow on nasal iris = shallow AC in PACS |
| Provocative test for angle closure | Dark room/prone provocative test - IOP rise ≥8 mmHg = significant |
Sources: Kanski's Clinical Ophthalmology 10th ed., pp. 389-394; Wills Eye Manual, pp. 575-576
This is a shared conversation. Sign in to Orris to start your own chat.