
I think that I might be having alopecia symptoms since the hairline is receding at the temple and also hair thinning is observed.
"androgenetic alopecia" AND treatment
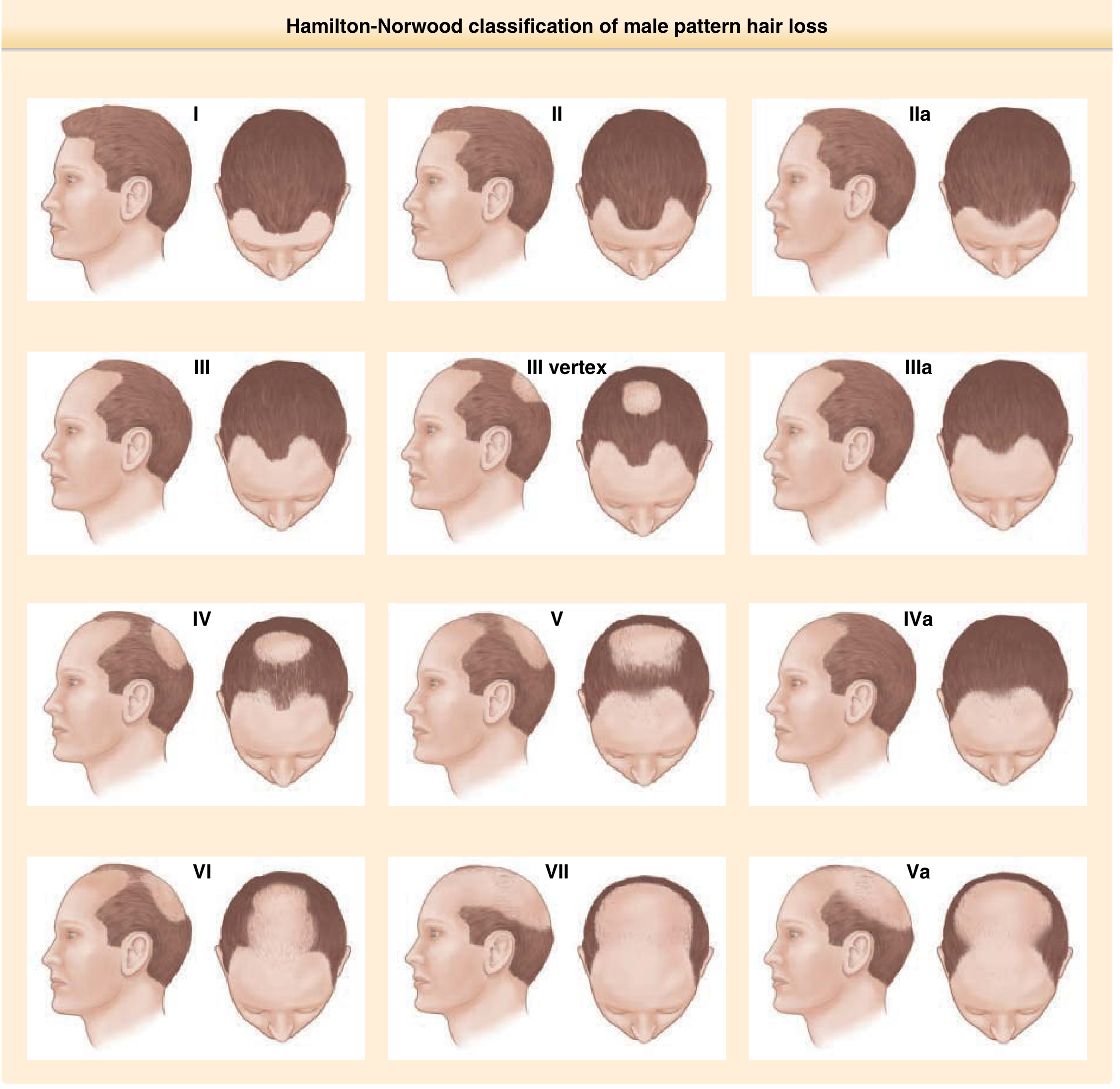
Your Hair Loss: What the Photo Shows
What is Androgenetic Alopecia (AGA)?
- Genetic predisposition (polygenic inheritance; early onset before 30 has a strong genetic component linked to the androgen receptor gene)
- Dihydrotestosterone (DHT): The scalp of balding individuals shows increased 5α-reduction of testosterone, yielding elevated DHT. This androgen signals follicles to progressively shorten their anagen (growth) phase, producing finer, lighter hairs until terminal hairs are replaced by vellus hairs
- The frontal and vertex regions are more sensitive to DHT; the occipital and parietal areas are typically spared
What Is Happening at the Follicle Level?
- Progressive shortening of the anagen phase - hairs get shorter with each cycle
- Follicular miniaturization - shaft diameter decreases over time
- A higher proportion of telogen (resting) hairs results in greater daily shedding
- Histologically: decrease in anagen follicles, increase in telogen follicles, fibromucinous fibrous tract remnants below miniaturized follicles
Treatment Options (Evidence-Based)
1. Topical or Oral Minoxidil
- Promotes survival of dermal papilla cells, prolongs anagen phase, enlarges shaft diameter
- Works best in early cases (less than 10 years duration) with limited extent
- Must be used indefinitely - benefits reverse on stopping
- Available OTC as 2% or 5% solution/foam
2. Finasteride 1 mg/day (oral)
- A type 2 5α-reductase inhibitor - blocks conversion of testosterone to DHT
- Stops further hair loss in up to 90% of men over 5 years; approximately 65% demonstrate regrowth
- Effective at vertex and frontal midscalp; temple patterning is generally not improved
- Visible results take 6+ months; if no effect by 12 months, unlikely to benefit
- Requires indefinite use; short-term side effects are infrequent but long-term monitoring is advisable
- Not suitable for women of childbearing age
3. Combination Therapy
- Studies show finasteride-containing regimens are more effective than minoxidil alone, and combining both drugs has enhanced efficacy
4. Microneedling + Minoxidil
- A 2023 systematic review and meta-analysis found the combination of topical minoxidil and microneedling superior to minoxidil alone for AGA
- A 2025 meta-analysis also confirmed combined microneedling therapy outperforms topical minoxidil alone in hair count and density
5. Dutasteride
- Blocks both type 1 and type 2 5α-reductase (broader than finasteride), shown effective in male pattern hair loss
6. Platelet-Rich Plasma (PRP)
- Shows promise as a supportive therapy; evidence continues to accumulate
7. Hair Transplantation
- A cosmetically effective option for non-progressive, stable AGA with sufficient donor area (occipital region) - typically considered at later stages
Key Points for You
| Factor | Detail |
|---|---|
| Stage | Norwood II-III (early-moderate) |
| Best window | Now - early intervention gives the best results |
| First-line | Minoxidil ± Finasteride |
| Temple recession | Less responsive to finasteride specifically; overall slowing of progression still beneficial |
| Confirmation | A dermatologist can perform trichoscopy (dermoscopy of scalp) to confirm miniaturization and rule out other causes |
When to See a Doctor
- Some other conditions (telogen effluvium, alopecia areata, tinea capitis) can mimic AGA
- Finasteride requires a prescription and baseline labs are sometimes checked
- If there is any history of hormonal issues, rapid onset, or patchy loss, further workup is warranted
Disclaimer: This information is educational, not a clinical diagnosis. A photo-based assessment cannot replace an in-person examination. Please consult a dermatologist.
My age - 22 years
"androgenetic alopecia" AND "early onset" AND treatment
PMID: 38451966
"finasteride" AND "androgenetic alopecia" AND "young men"
AGA at Age 22 - What This Means
Early Onset is a Distinct Entity
- Family history is the strongest risk factor - if your father or maternal grandfather has significant baldness, your progression is more likely
- Hormonal profile and androgen receptor gene activity are particularly active drivers in early-onset cases
- Early-onset AGA is associated with increased metabolic risk - including insulin resistance, dyslipidemia, and cardiovascular markers. This does not mean you have these conditions, but a basic metabolic screen at your next checkup is reasonable
- Young men with AGA disproportionately experience anxiety and low self-esteem - this is a recognized, documented association worth acknowledging
Earlier Onset = Faster Potential Progression
Treatment at 22 - Specific Considerations
What Works and Is Safe at Your Age
| Treatment | Relevance at 22 |
|---|---|
| Topical Minoxidil 5% (foam/solution) | First-line. Safe, OTC, no age restrictions. Apply once daily (foam) or twice daily (solution) to dry scalp |
| Oral low-dose Minoxidil (0.625-2.5 mg/day in men) | Off-label but well-documented. Monitor for cardiovascular side effects (periorbital edema, dizziness) |
| Finasteride 1 mg/day | Approved for men 18+. At 22, your prostate cancer risk from finasteride is essentially irrelevant. The main concern is sexual side effects |
| Microneedling + Minoxidil | A 2025 meta-analysis confirms this combination outperforms minoxidil alone - worth considering as an add-on |
Finasteride at 22 - Honest Risk-Benefit
- Benefits are high - early, aggressive intervention preserves the most hair long-term
- Prostate concerns are not relevant at your age
- Sexual side effects (reduced libido, erectile dysfunction) occur in approximately 2% of men and are generally reversible on stopping
- Post-finasteride syndrome (persistent sexual dysfunction after stopping) has been reported but its true incidence is uncertain. A 2026 review by Spanish dermatologists is ongoing. Discuss this with your dermatologist before starting
- Bottom line: Many dermatologists consider finasteride the most impactful single intervention for young men with AGA. The decision should be made with full information, ideally with a dermatologist
What to Avoid / Lifestyle Factors
- Smoking - independently associated with early-onset AGA; avoid if you smoke
- High BMI / unhealthy diet - associated with worse progression
- Nutritional deficiencies - a 2024 systematic review on micronutrients and AGA suggests adequate iron, zinc, vitamin D, and biotin are relevant, especially in young men
Practical Action Plan for You
- See a dermatologist soon - at 22, you want a trichoscopy to confirm the stage and rule out other causes (e.g., telogen effluvium from stress or nutritional deficiency, which can co-exist)
- Start topical minoxidil 5% now - it is OTC, safe, and you do not need a prescription. Expect 3-6 weeks of initial shedding (this is normal - old telogen hairs clearing before new anagen growth)
- Discuss finasteride with your dermatologist - given your age and early stage, the risk-benefit strongly favors its use if you are comfortable with the side effect profile
- Get basic bloods checked: ferritin, thyroid (TSH), vitamin D, zinc - deficiencies are common at your age and can compound AGA
- Consider microneedling sessions with a trained professional as an adjunct
Disclaimer: This is educational information, not a prescription or clinical diagnosis. Please consult a qualified dermatologist before starting any medication.
My age is 22 years height 6 ft and weight is 55 kg which I am underweight and hence have nutritional deficiencies, so that might be a good reason for these hair symptoms, also I am experiencing hair greying. I think I am Vitamin B12 deficient
"vitamin B12" AND "hair loss" AND deficiency
"premature hair graying" AND "nutritional deficiency"
"premature graying" AND "vitamin B12" AND hair
PMID: 41981836
"micronutrients" AND "androgenetic alopecia" AND deficiency
PMID: 39440586
Your Profile: BMI 16.5 - Significantly Underweight
Process 1: Telogen Effluvium from Malnutrition
Process 2: Androgenetic Alopecia (AGA) - Likely Still Present
The Nutritional Deficiencies - What the Evidence Says
Vitamin B12 and Hair Greying - Direct Evidence
- 71.5% of premature greying cases were in the 15-25 year age group - exactly your age
- Cases had significantly lower serum B12 (p=0.012), ferritin (p=0.020), and Vitamin D3 (p=0.043) compared to controls
- Family history and smoking were also significant risk factors
How B12 Deficiency Causes Hair Greying
- DNA and histones become hypomethylated
- Melanocyte function (the cells that produce hair pigment) is impaired
- Melanin synthesis in hair follicles decreases, resulting in grey/white hairs (Basic Medical Biochemistry 6e, p. 1394)
Full Micronutrient Picture for You
| Nutrient | Role in Hair | What Deficiency Causes |
|---|---|---|
| Vitamin B12 | Melanocyte function, DNA methylation, cell division | Premature greying, hair loss, neurological symptoms |
| Iron / Ferritin | Oxygen delivery to follicles, enzyme cofactor | Telogen effluvium, diffuse thinning - serum ferritin should be ≥40 ng/dL |
| Vitamin D | Follicle cycling, immune regulation | AGA worsening, telogen effluvium |
| Zinc | Protein synthesis, follicle structure | Hair fragility, shedding |
| Protein / Calories | Building keratin (hair is ~95% keratin) | Diffuse hair loss, thin brittle hair |
| B-complex (Biotin, B7) | Keratin production | Hair fragility, thinning |
Other B12 Deficiency Symptoms to Watch For
- Tingling or numbness in hands/feet (peripheral neuropathy - can be irreversible if prolonged)
- Fatigue and weakness
- Pale or yellowish skin
- Sore, smooth tongue (glossitis)
- Difficulty concentrating / brain fog
- Palpitations (from megaloblastic anemia)
Prioritized Action Plan for You
Step 1: Get These Blood Tests Done NOW
| Test | Why |
|---|---|
| Serum Vitamin B12 | Confirm deficiency |
| Serum Ferritin | Should be ≥40 ng/dL for hair health |
| Vitamin D (25-OH) | Frequently low in young Indians |
| CBC (Complete Blood Count) | Check for megaloblastic anemia |
| Thyroid function (TSH, T3, T4) | Hypothyroidism causes hair loss + greying |
| Fasting blood glucose | AGA + low BMI - rule out metabolic issues |
| Serum zinc | Often low in malnourished individuals |
Step 2: Address the Root Cause - Gain Weight
Step 3: Supplement Based on Results
- Vitamin B12: If deficient, oral cyanocobalamin 1000 mcg/day or IM injections (faster for severe deficiency)
- Vitamin D3: 60,000 IU/week for 8 weeks if deficient (common Indian protocol)
- Iron: Only if ferritin is low (excess iron is harmful)
- Zinc: 25-50 mg/day if deficient
- High-protein diet or protein supplementation
Step 4: Defer Finasteride Until Nutritional Status is Corrected
Summary
Your hair loss and greying have two likely contributors: early-onset AGA (genetically driven, temple pattern) + nutritional deficiency-driven telogen effluvium and melanocyte dysfunction (B12, ferritin, Vitamin D). The nutritional component is treatable and potentially reversible. Getting blood tests done and gaining weight are your most urgent priorities right now - more so than any hair-specific medication.
Disclaimer: This is educational information only. Please consult a physician and dermatologist for a proper clinical evaluation and treatment plan.