Teach me thyrotoxicosis as I'm 3rd year pg resident of medicine appearing for muhs theory exam and help me write laq for same
Reading File
Finding Sources
Finding Sources
Searching the Web
thyrotoxicosis MUHS theory exam long answer question MD medicine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have more than enough material to write a comprehensive, exam-ready answer. Let me compile everything into a structured LAQ response.
Thyrotoxicosis - Complete PG Medicine Teaching + LAQ Guide
Source: Harrison's Principles of Internal Medicine 22E (2025), Tintinalli's Emergency Medicine
QUICK CONCEPTUAL FRAMEWORK (Read this first)
Thyrotoxicosis = state of thyroid hormone excess (any cause)
Hyperthyroidism = subset where the thyroid itself is overproducing hormones
Think of it this way: all hyperthyroidism is thyrotoxicosis, but not all thyrotoxicosis is hyperthyroidism (e.g., thyroiditis releases stored hormone without new synthesis).
LONG ANSWER QUESTION FORMAT
"Discuss Thyrotoxicosis - Etiology, Pathogenesis, Clinical Features, Diagnosis, and Management including Thyroid Storm"
(This is a standard 15-mark LAQ. MUHS expects a structured answer with headings, mechanism, clinical table, scoring systems, and stepwise management.)
I. DEFINITION
Thyrotoxicosis is the clinical syndrome resulting from excess circulating thyroid hormones (T3 and T4), regardless of the underlying cause. It differs from hyperthyroidism, which specifically refers to excess thyroid hormone synthesis by the gland itself.
II. ETIOLOGY / CLASSIFICATION
A. Thyrotoxicosis WITH Hyperthyroidism (increased synthesis)
| Cause | Mechanism |
|---|---|
| Graves' disease (60-80%) | TSH receptor stimulating antibodies (TRAb/TSI) |
| Toxic multinodular goiter (MNG) | Autonomous nodules with activating mutations |
| Toxic adenoma | Single autonomous nodule |
| Functioning thyroid carcinoma metastases | Ectopic hormone production |
| Activating mutation of TSH receptor | Constitutive receptor activation |
| McCune-Albright syndrome | Activating mutation of Gsa |
| Struma ovarii | Ovarian teratoma with thyroid tissue |
| Jod-Basedow phenomenon | Iodine excess in iodine-deficient subjects |
B. Thyrotoxicosis WITHOUT Hyperthyroidism (release of stored hormone)
- Subacute (de Quervain) thyroiditis - painful, post-viral
- Silent/postpartum thyroiditis - painless, autoimmune
- Drug-induced thyroid destruction: amiodarone, cytokines, tyrosine kinase inhibitors, immune checkpoint inhibitors (nivolumab)
- Radiation thyroiditis
- Infarction of adenoma
- Thyrotoxicosis factitia (exogenous ingestion)
C. Secondary Hyperthyroidism (TSH-driven)
- TSH-secreting pituitary adenoma
- Thyroid hormone resistance syndrome
- Chorionic gonadotropin-secreting tumors (gestational thyrotoxicosis, hydatidiform mole)
III. GRAVES' DISEASE - PATHOGENESIS (Most important - max marks)
Epidemiology: Most common cause (60-80%). Prevalence up to 2% in women, 10x less common in men. Peak age 20-50 years.
Genetic factors: HLA-DR, CTLA-4, CD25, CD40, PTPN22, FCRL3, CD226, and TSH-R gene polymorphisms. Monozygotic twin concordance 20-30% vs <5% in dizygotic twins.
Pathogenesis (core mechanism):
- Loss of immune tolerance to TSH receptor (TSH-R)
- B-lymphocytes in thyroid, bone marrow, and lymph nodes produce thyroid stimulating immunoglobulins (TSI)
- TSI binds TSH-R and continuously stimulates thyroid follicular cells - mimicking TSH action
- Results in diffuse thyroid hyperplasia + unregulated hormone synthesis
- TSH-R antibodies (TRAb) detectable by immunoassay - cross placenta and cause neonatal thyrotoxicosis
- Concurrent TPO and Tg antibodies in up to 80% of cases
Ophthalmopathy mechanism:
- Activated T cells infiltrate extraocular muscles
- IFN-γ, TNF, IL-1 activate fibroblasts
- Increased glycosaminoglycan synthesis traps water → muscle swelling
- IGF-1R aberrant signaling on orbital fibroblasts (basis for teprotumumab therapy)
- Late stage: irreversible fibrosis → diplopia
Environmental triggers: Stress, smoking (major risk for ophthalmopathy), iodine excess, post-partum (3x increased risk), immune reconstitution (post-HAART, alemtuzumab, immune checkpoint inhibitors)
IV. CLINICAL FEATURES
A. General Features of Thyrotoxicosis (any cause)
| Symptoms | Signs |
|---|---|
| Hyperactivity, irritability, dysphoria | Tachycardia; atrial fibrillation (especially elderly) |
| Heat intolerance and sweating | Tremor (fine, postural) |
| Palpitations | Goiter |
| Fatigue and weakness | Warm, moist skin |
| Weight loss with increased appetite | Proximal myopathy |
| Diarrhea | Lid retraction or lid lag |
| Polyuria | Gynecomastia |
| Oligomenorrhea, loss of libido | Onycholysis (Plummer's nails) |
Remember: In elderly patients, the presentation may be subtle ("apathetic hyperthyroidism") - fatigue, weight loss, AF without classic sympathomimetic features.
B. Features Specific to Graves' Disease (the triad)
- Diffuse goiter - smooth, non-tender, bruit may be audible (due to high vascularity)
- Ophthalmopathy (Graves' orbitopathy)
- Periorbital edema, chemosis, proptosis/exophthalmos
- Lid retraction (Dalrymple's sign), lid lag (von Graefe's sign)
- External ophthalmoplegia, diplopia
- Corneal ulceration, optic neuropathy (vision-threatening)
- Dermopathy (pretibial myxedema)
- Non-pitting, indurated skin thickening over shins
- Orange-peel texture ("peau d'orange")
- Thyroid acropachy (rare) - clubbing + periosteal new bone formation
V. INVESTIGATIONS / DIAGNOSIS
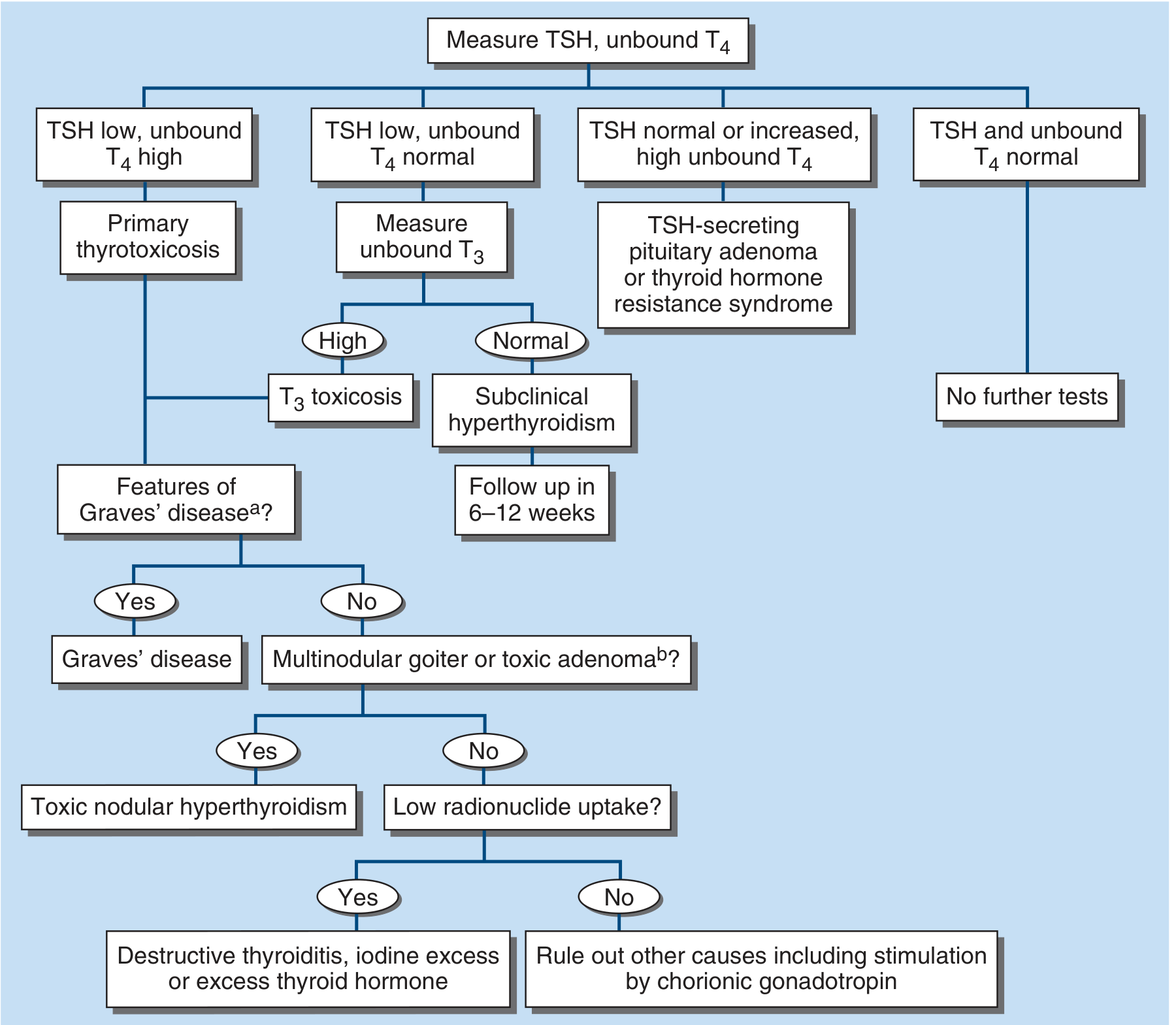
Step-by-step (follow the algorithm):
Step 1: TSH + unbound (free) T4
- TSH suppressed + T4 elevated = Primary thyrotoxicosis (most cases)
- TSH suppressed + T4 normal → check free T3 → if elevated = T3 toxicosis (seen in early Graves', toxic adenoma)
- TSH normal/elevated + T4 elevated = TSH-secreting pituitary adenoma or thyroid hormone resistance
Step 2: Establish cause
- TRAb (TSH receptor antibody): Positive in Graves' disease - most specific test
- Radionuclide scan (99mTc, 123I, 131I):
- Diffuse high uptake = Graves' disease
- Focal hot nodule + suppressed surrounding = Toxic adenoma
- Low/patchy uptake = Destructive thyroiditis or factitial
- Color-flow Doppler USG: High blood flow = hyperthyroidism; low flow = thyroiditis (avoids radioactivity)
Step 3: Additional labs
- Elevated bilirubin, liver enzymes, ferritin (common in thyrotoxicosis)
- Microcytic anemia, thrombocytopenia may occur
- ECG: sinus tachycardia, AF
- In T4 toxicosis: iodine excess providing excess substrate → elevated T4 with normal T3
VI. MANAGEMENT OF THYROTOXICOSIS
Three main modalities:
A. Antithyroid Drugs (ATDs)
Drugs: Carbimazole / Methimazole (preferred) and Propylthiouracil (PTU)
Mechanism: Inhibit thyroid peroxidase (TPO) enzyme → block organification of iodide → block coupling of MIT and DIT → prevent new T3/T4 synthesis. PTU additionally blocks peripheral conversion of T4 to T3.
Dosing (Harrison's):
- Methimazole/Carbimazole: 10-20 mg every 12 h initially; once-daily dosing after euthyroidism
- PTU: 100-200 mg every 6-8 h (always in divided doses)
- Lower doses in iodine-deficient areas
Regimens:
- Titration regimen (preferred): Gradually reduce dose as thyrotoxicosis improves - minimizes drug dose, monitors response
- Block-replace regimen: High-dose ATD + LT4 added to prevent hypothyroidism - avoids dose adjustment, higher drug exposure
Monitoring: TFTs at 4-6 weeks; euthyroid status at 6-8 weeks; TSH may stay suppressed for months.
Duration: 12-18 months for remission (30-60% remission rate). Relapse likely in: young, males, smokers, large goiter, TRAb persistence.
Side effects:
- Minor (1-5%): rash, urticaria, fever, arthralgia
- Major (rare): Agranulocytosis (<1%) - most important; hepatitis (PTU > methimazole); cholestasis (methimazole); vasculitis
- Warn all patients: sore throat, fever, mouth ulcers = stop drug immediately, check CBC
Pregnancy: Use PTU in 1st trimester (methimazole teratogenic - aplasia cutis, choanal atresia); switch to methimazole in 2nd/3rd trimester (PTU has rare hepatic failure risk).
B. Beta-Blockers (symptomatic control)
- Propranolol 20-40 mg every 6 h OR atenolol (longer-acting, selective β1)
- Control adrenergic symptoms (palpitations, tremor, anxiety) while ATDs take effect
- Also useful in thyrotoxic periodic paralysis
C. Radioactive Iodine (RAI - 131I)
- Definitive treatment for Graves', toxic MNG, toxic adenoma
- Contraindicated in: pregnancy, active/severe ophthalmopathy (worsens eye disease, especially smokers)
- May precipitate thyroid storm: ensure euthyroid state before RAI; rarely due to hormone release from damaged follicles
- Hypothyroidism is the expected outcome (15-30% at 1 year, up to 80% at 10 years) - actually desired
D. Surgery (Total/Near-Total Thyroidectomy)
- Indications: large goiter, compressive symptoms, malignancy suspected, patient preference, failed ATDs
- Advantages: rapid cure, suitable in pregnancy (2nd trimester preferred)
- Complications: recurrent laryngeal nerve palsy, hypoparathyroidism
VII. THYROID STORM (Thyrotoxic Crisis)
This is a high-yield sub-topic for LAQ.
Definition:
Life-threatening exacerbation of thyrotoxicosis characterized by multi-organ dysfunction due to extreme excess of thyroid hormones, usually precipitated by a physiologic stressor in a patient with pre-existing hyperthyroidism.
Precipitants (MNEMONIC: "SITS WIDE"):
- Surgery (thyroid or non-thyroid)
- Infection (most common precipitant)
- Trauma
- Stress (physical/emotional)
- Withdrawal of antithyroid drugs
- Iodine excess / RAI administration
- DKA / hyperosmolar coma
- Eclampsia / labor / delivery; MI, PE, CVA
Unknown cause in up to 25% of cases.
Clinical Features:
- Fever (>38.5°C) - hallmark
- Tachycardia (often >140 bpm), AF, high-output cardiac failure
- CNS: Agitation → delirium → psychosis → seizures → coma
- GI: Nausea, vomiting, diarrhea, abdominal pain, jaundice (severe - marker of bad prognosis)
- Diaphoresis, vomiting, dehydration
Diagnosis - Burch-Wartofsky Point Scale (BWPS):
| Parameter | Points |
|---|---|
| Temperature | |
| 37.2-37.7°C | 5 |
| 37.7-38.3°C | 10 |
| 38.3-38.8°C | 15 |
| 38.9-39.4°C | 20 |
| 39.4-39.9°C | 25 |
| ≥40°C | 30 |
| CNS effects | |
| Absent | 0 |
| Mild (agitation) | 10 |
| Moderate (delirium/psychosis) | 20 |
| Severe (seizures/coma) | 30 |
| GI-hepatic dysfunction | |
| Absent | 0 |
| Moderate (N/V/diarrhea) | 10 |
| Severe (jaundice) | 20 |
| Tachycardia | |
| 90-109 bpm | 5 |
| 110-119 | 10 |
| 120-129 | 15 |
| ≥140 | 25 |
| Congestive Heart Failure | Mild 5 / Moderate 10 / Severe 15 |
| AF | Present = 10 |
| Precipitating event | Present = 10 |
Interpretation:
- ≥45: Thyroid storm
- 25-44: Impending storm - treat aggressively
- <25: Unlikely storm
(Note: Japanese Thyroid Association criteria TS1/TS2 are an alternative; BWPS ≥45 is more sensitive.)
Treatment of Thyroid Storm (Stepwise - must memorize the ORDER):
Treat empirically - do NOT wait for lab confirmation.
Step 1: Supportive care
- ICU admission
- IV fluids, cooling blankets, paracetamol (avoid aspirin - displaces T4 from TBG)
- Treat arrhythmias
Step 2: Beta-blockade (adrenergic control)
- Propranolol IV: 0.5-1 mg/min slow IV up to 10 mg; OR 60-80 mg PO every 4-6 h
- Alternatively: esmolol infusion (titratable, short-acting - preferred in cardiac compromise)
Step 3: Inhibit NEW thyroid hormone synthesis (ATDs FIRST)
- PTU 500-1000 mg loading dose PO, then 250 mg every 4 h (preferred over methimazole in storm - also blocks T4→T3 conversion)
- OR Methimazole 20-40 mg PO every 6-8 h (if PTU unavailable)
Step 4: Inhibit thyroid hormone RELEASE (at least 1 hour AFTER ATDs)
- Lugol's iodine: 8-10 drops PO every 6-8 h
- OR SSKI (saturated KI): 5 drops every 6 h
- OR Lithium carbonate 300 mg every 6 h (if iodine allergy or agranulocytosis)
- (Must give ATDs FIRST - otherwise iodine provides substrate for more hormone synthesis - "Wolff-Chaikoff vs Jod-Basedow paradox")
Step 5: Block peripheral T4 → T3 conversion
- Hydrocortisone 300 mg IV bolus, then 100 mg IV every 8 h (also corrects relative adrenal insufficiency from hypermetabolism)
- OR Dexamethasone 2 mg IV every 6 h
Step 6: Prevent free thyroid hormone reabsorption
- Cholestyramine 4 g every 6 h (binds TH in enterohepatic circulation)
Step 7: Treat the precipitating event (antibiotics for infection, etc.)
Step 8: Definitive therapy - RAI or thyroidectomy after stabilization
Last resort: Plasmapheresis/dialysis for refractory cases
VIII. SPECIAL SITUATIONS
Subclinical Hyperthyroidism
- Suppressed TSH, normal free T4 and T3
- Treat if: age >65 years, AF, osteoporosis risk, or TSH persistently <0.1
Thyrotoxic Periodic Paralysis
- More common in Asian males
- Episodic hypokalemia + muscle weakness
- Trigger: high carbohydrate meal, exercise
- Treat: propranolol + KCl replacement; definitive = treat thyrotoxicosis
Amiodarone-induced Thyrotoxicosis (AIT)
- Type 1: Jod-Basedow (iodine-induced excess synthesis) - treat with ATDs
- Type 2: Destructive thyroiditis - treat with prednisolone
- Distinguish by color Doppler (Type 1: high flow; Type 2: low/absent flow)
IX. KEY DIFFERENTIALS TO REMEMBER FOR EXAM
| Feature | Graves' | Toxic MNG | Toxic Adenoma | Thyroiditis |
|---|---|---|---|---|
| Goiter | Diffuse, smooth | Nodular | Single nodule | Tender (subacute) |
| Ophthalmopathy | Yes | No | No | No |
| TRAb | Positive | Negative | Negative | Negative |
| Radionuclide scan | Diffuse high uptake | Patchy high + hot nodules | Single hot nodule | Low/absent uptake |
| RAIU | High | High | High | Low |
X. HIGH-YIELD EXAM POINTS FOR MUHS
- PTU is preferred in thyroid storm (not methimazole) - because it also blocks T4→T3 conversion
- Iodine must be given AFTER ATDs (1 hour gap) - not before
- Avoid aspirin in thyroid storm - displaces thyroid hormone from TBG
- BWPS ≥45 = thyroid storm confirmed
- Teprotumumab - monoclonal antibody targeting IGF-1R for Graves' ophthalmopathy (new)
- T3 toxicosis - suppressed TSH, normal T4, elevated T3 - seen in early Graves' and toxic adenoma
- Apathetic hyperthyroidism in elderly - AF + weight loss without classic features
- Agranulocytosis - most dangerous ATD side effect; onset idiosyncratic and abrupt; stop drug immediately if sore throat/fever
- Block-replace vs titration - titration preferred to minimize drug exposure
- Remission rate of ATDs: 30-60% at 18 months
SAMPLE LAQ ANSWER OUTLINE (Exam format, 15 marks)
Introduction (1 mark): Define thyrotoxicosis and distinguish from hyperthyroidism
Etiology (2 marks): Table with three categories - WITH hyperthyroidism / WITHOUT hyperthyroidism / Secondary
Pathogenesis (3 marks): Focus on Graves' - TRAb/TSI mechanism, ophthalmopathy cytokine cascade
Clinical features (2 marks): General table + Graves'-specific triad
Diagnosis (2 marks): TSH/T4 algorithm + TRAb + radionuclide scan
Management (3 marks): ATDs with doses + RAI + surgery indications
Thyroid storm (2 marks): BWPS scoring system + stepwise 8-point management protocol
Total: 15 marks
Sources: Harrison's Principles of Internal Medicine 22E (2025), pp. 3075-3082 | Tintinalli's Emergency Medicine, Chapter 229
This is a shared conversation. Sign in to Orris to start your own chat.