How to fill the partograph
Reading File
Finding Sources
Searching the Web
how to fill partograph labor monitoring WHO
Finding Sources
Reading Web Page
https://medicalguidelines.msf.org/en/viewport/ONC/english/5-…
Loading Image
Finding Sources
I now have excellent material to give a thorough, well-structured answer. Here is the complete guide:
How to Fill the Partograph
The partograph is a graphical record of observations made during labour. It monitors both fetal and maternal wellbeing during the active phase of labour and serves as an early warning tool and decision-making aid.
Step 0 - Before You Start
- Only begin a partograph when the woman is confirmed to be in labour (contracting sufficiently).
- Check there are no existing complications requiring immediate action.
- The partograph covers the active phase; it is not started during the latent phase.
- According to the WHO/MSF protocol, start the graph at 5 cm dilation (or 4 cm if labour is induced), with at least 3 contractions every 10 minutes.
SECTION 1 - Patient Identification (Top of the Form)
Fill in at admission:
| Field | What to Record |
|---|---|
| Name | Full name of the woman |
| Gravida | Number of pregnancies (including current) |
| Para | Number of previous deliveries |
| Hospital number | Registration/admission number |
| Date of admission | Calendar date |
| Time of admission | Actual clock time labour began/admission time |
| Ruptured membranes | Number of hours since membranes ruptured |
SECTION 2 - Fetal Condition (Upper Graph)
Fetal Heart Rate (FHR)
- Record every 30 minutes during active labour (every 15 min in second stage).
- Normal range: 110-160 bpm.
- The graph has bold lines at 100 and 180 bpm - values outside these lines indicate fetal distress.
- Plot each reading as a dot and connect with a line.
Amniotic Fluid
- Assessed at each vaginal examination and recorded in the row below FHR.
- Use standard codes:
- I = Intact membranes
- C = Clear fluid
- M = Meconium-stained
- B = Blood-stained
- A = Absent (dry)
Moulding (Caput / Skull Overlap)
- Assessed by vaginal examination.
- Record using codes:
- 0 = No moulding
- + = Bones just touching
- ++ = Bones overlapping but reducible
- +++ = Bones severely overlapping, not reducible (dangerous - suggests cephalopelvic disproportion)
SECTION 3 - Labour Progress (Central Graph - The Most Important Section)
This is the core of the partograph.
Cervical Dilation (Plot with X)
- Assessed by vaginal examination every 4 hours (or more frequently if clinically indicated).
- Plot on the y-axis (0-10 cm) against time on the x-axis.
- Mark each finding with an "X".
- The first plot in the active phase goes directly onto the Alert Line, regardless of actual hours elapsed.
Descent of Fetal Head (Plot with O)
- Assessed by abdominal examination (rule of fifths above the pelvic brim) - always done immediately BEFORE the vaginal examination.
- Scale: 5/5 = head fully above pelvic brim; 0/5 = head fully engaged.
- Plot with an "O" at the same time as cervical dilation.
The Alert Line and Action Line
| Line | What It Represents | Action Required |
|---|---|---|
| Alert Line | Expected dilation of 1 cm/hour (drawn from 4-5 cm to 10 cm) | If cervical dilation plot crosses to the right, labour may be prolonged; consider transfer to CEmONC facility |
| Action Line | Drawn 4 hours to the right of the alert line, parallel to it | If plot reaches or crosses this line, active management is mandatory (augmentation, ARM, caesarean section) |
Normal labour: the cervical dilation plot stays on or to the left of the Alert Line.
SECTION 4 - Contractions (Below the Cervicograph)
- Record every 30 minutes.
- Count number of contractions in a 10-minute window (y-axis: 1-5 contractions).
- Each box represents one contraction; shade the box to indicate duration:
- Dotted/outline only = < 20 seconds (mild)
- Hatched/diagonal lines = 20-40 seconds (moderate)
- Solid/fully filled = > 40 seconds (strong)
SECTION 5 - Medications and Oxytocin
- Oxytocin (U/L and drops/min): Record dose and rate of infusion.
- Drugs given and IV fluids: Write the drug name, dose, route, and time administered in the free-text boxes.
SECTION 6 - Maternal Condition (Lower Section)
Pulse and Blood Pressure
- Pulse (marked with a dot •): Record every 30 minutes.
- Blood pressure (marked as a vertical line with arrows ↑↓): Record every 4 hours (or every 30 min if hypertensive).
- Both are plotted on the same graph (range 60-180).
Temperature
- Record every 4 hours (or 2-hourly if elevated).
- Normal: 36.5-37.5°C.
Urine
- Record each time the woman passes urine:
- Protein: None, trace, +, ++, +++
- Acetone: None, trace, +, ++
- Volume: Amount in mL
Summary: Recording Frequency
| Parameter | Frequency |
|---|---|
| Fetal heart rate | Every 30 min (15 min in 2nd stage) |
| Cervical dilation & fetal descent | Every 4 hours (vaginally) |
| Contractions | Every 30 min |
| Pulse | Every 30 min |
| Blood pressure | Every 4 hours (more if hypertensive) |
| Temperature | Every 4 hours |
| Amniotic fluid & moulding | Each vaginal examination |
Key Interpretation Rules
- Latent phase (0-3 cm): Should last no more than 8 hours; the partograph has a heavy line at 8 hours of the latent phase as a warning.
- Active phase (4-10 cm): Normal rate is at least 1 cm/hour.
- Plot crossing the Alert Line = monitor closely, consider transfer.
- Plot crossing the Action Line = intervene immediately (augment, ARM, or caesarean section).
- Moulding +++ even with adequate contractions strongly suggests cephalopelvic disproportion.
Note: The WHO has more recently introduced the Labor Care Guide (LCG) as an evolution of the partograph, integrating respectful maternity care and shared decision-making principles. However, the traditional partograph remains widely used and taught. - MSF Obstetric Guidelines, Chapter 5.2

17839638842256978810910899714439.jpg
Can you give for this partograph and please ignore the markings on it
analyse_media
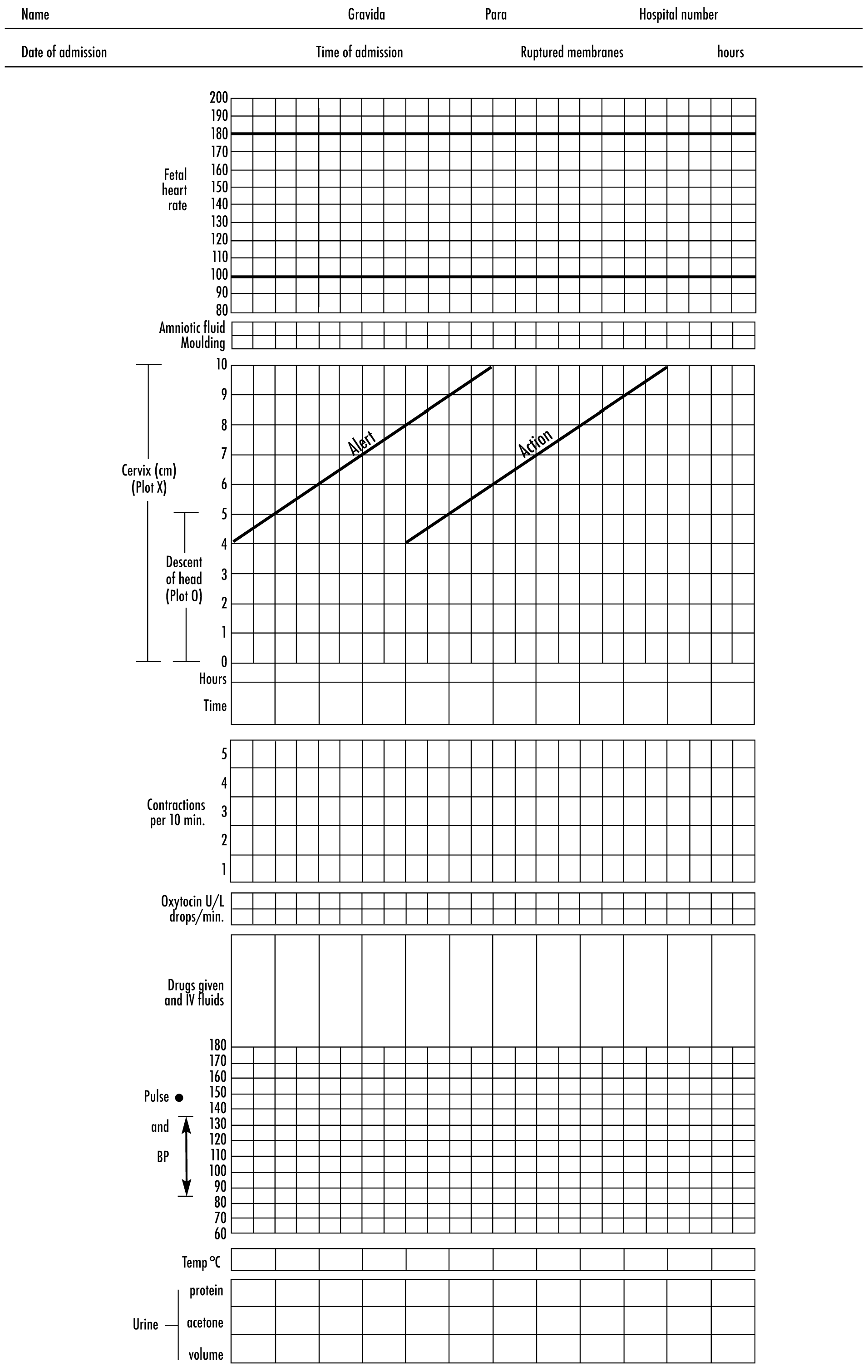
Here is a complete, step-by-step guide on how to fill this specific WHO Simplified Partograph form, based on its exact layout:
How to Fill This WHO Simplified Partograph
SECTION 1 - Header (Patient Details)
Fill these fields at the time of admission:
| Field | What to Write |
|---|---|
| Name | Patient's full name |
| Gravida | Total number of pregnancies (including this one) |
| Para | Number of previous deliveries |
| Hospital No. | Hospital registration/medical record number |
| Date of admission | Date the patient was admitted in labour |
| Time of admission | Clock time she was admitted |
| Ruptured membranes | Actual clock time when membranes ruptured |
| Hours | How many hours ago the membranes ruptured |
SECTION 2 - Fetal Condition (Upper Panel)
Fetal Heart Rate
- Y-axis: 100 to 180 bpm, in increments of 10.
- Record every 30 minutes (every 15 minutes in the second stage).
- Plot each reading as a dot, then connect dots with a line.
- Normal range: 110-160 bpm.
- The form has bold/thick lines at 100 and 180 - values outside these are danger signs.
Liquor (Amniotic Fluid)
- Record in the Liquor row at every vaginal examination.
- Use standard codes:
- I = Intact membranes (not yet ruptured)
- C = Clear fluid
- M = Meconium-stained (green/brown)
- B = Blood-stained
- A = Absent / dry
Moulding
- Record in the Moulding row at every vaginal examination.
- Codes:
- 0 = No moulding
- + = Bones just touching
- ++ = Bones overlapping but reducible
- +++ = Severe overlap, not reducible (serious - suggests cephalopelvic disproportion)
SECTION 3 - Progress of Labour (Central Graph - Most Important)
This form has a Latent Phase zone on the left (Hours 0-8 at 3 cm) and an Active Phase zone on the right with two diagonal pre-printed lines.
Understanding the Pre-printed Lines on This Form
- Alert Line: Diagonal line from 4 cm at Hour 8 to 10 cm at Hour 14 - represents 1 cm/hour dilation.
- Action Line: Diagonal line from 4 cm at Hour 12 to 10 cm at Hour 18 - drawn 4 hours to the right of the alert line.
How to Plot Cervical Dilation (use X)
- During the latent phase (0-3 cm), plot dilatation in the latent phase area against actual hours elapsed.
- When the woman enters the active phase (4 cm+), plot the first active-phase reading directly on the Alert Line at 4 cm - do NOT plot it at the actual hour spent so far.
- All subsequent readings are plotted every 4 hours (or as needed) moving to the right.
- Mark each reading with an "X".
How to Plot Descent of Fetal Head (use O)
- Assessed by abdominal examination (fifths of head palpable above pelvic brim) - done just BEFORE each vaginal exam.
- Scale: 5/5 = head fully above brim; 0/5 = fully engaged/delivered.
- Mark with an "O" at the same time column as the cervical dilation reading.
Time Row
- In the Hours row: write 1, 2, 3... sequentially from left.
- In the Time row: write the actual clock time (e.g., 08:00, 08:30, 09:00...) under each column.
Interpreting the Graph
| Plot position | Meaning | Action |
|---|---|---|
| On or to the LEFT of Alert Line | Normal progress | Continue monitoring |
| Crosses to the RIGHT of Alert Line | Labour slowing (<1 cm/hr) | Increase monitoring; consider transfer to higher facility |
| Reaches or crosses the Action Line | Abnormal labour | Intervene immediately - augmentation, ARM, or caesarean section |
SECTION 4 - Contractions (Below the Main Graph)
- Y-axis: 1 to 5 contractions per 10 minutes.
- Record every 30 minutes.
- Count the number of contractions felt in a 10-minute window and shade that many boxes in the column.
- Shade the box differently to indicate strength/duration:
- Outline only (dotted) = < 20 seconds (mild)
- Hatched = 20-40 seconds (moderate)
- Solid/fully shaded = > 40 seconds (strong)
SECTION 5 - Oxytocin & Medications
Oxytocin U/L / drops per min
- Two rows: write the concentration (U/L) in the top row and the infusion rate (drops/min) in the bottom row.
- Update whenever the rate changes.
Drugs given and IV fluids
- In the open section below oxytocin, write:
- Drug name, dose, route, and time given
- Type and volume of IV fluids running
SECTION 6 - Maternal Condition (Lower Panel)
Pulse and Blood Pressure
- Y-axis: 60 to 180 (same scale for both).
- Pulse (dot •): Record every 30 minutes.
- Blood Pressure (vertical arrow ↑↓ with top = systolic, bottom = diastolic): Record every 4 hours (or every 30 min if hypertensive - as noted "4 hourly" on this form).
- Plot both on the same grid and connect pulse dots with a line.
Temperature (Temp °C)
- Record in the Temp °C row every 4 hours (or 2-hourly if raised).
- Write the numeric value in the box (e.g., 37.2).
Urine
Record each time the woman passes urine in the three rows:
- Protein: Nil / Trace / + / ++ / +++
- Acetone: Nil / Trace / + / ++
- Volume: Amount in mL (e.g., 200)
Quick Reference Summary
| Parameter | Plotted With | Frequency |
|---|---|---|
| Fetal heart rate | Dot + line | Every 30 min |
| Liquor/Moulding | Letter code | Every vaginal exam |
| Cervical dilation | X | Every 4 hours |
| Fetal descent | O | Every 4 hours (abdominal exam) |
| Contractions | Shaded boxes | Every 30 min |
| Pulse | Dot • | Every 30 min |
| Blood pressure | Arrow ↑↓ | Every 4 hours |
| Temperature | Number in box | Every 4 hours |
| Urine | Codes/volume | Each void |
Key rule for this form: The Active Phase plotting always starts at the Alert Line (4 cm). If the woman is admitted already at 6 cm, that 6 cm reading goes on the Alert Line at the 6 cm mark - not at whatever hour she spent in labour before admission. All subsequent plots move rightward in real time from that starting point.
This is a shared conversation. Sign in to Orris to start your own chat.