Hypernatremia evaluation & management
Reading File
Finding Sources
Searching PubMed
hypernatremia management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Hypernatremia: Evaluation & Management
Definition
Hypernatremia is defined as plasma [Na⁺] > 145 mmol/L (some sources use >144 mmol/L). It always reflects hypertonicity — an increased concentration of osmotically active solutes across all body fluid compartments. It is considerably less common than hyponatremia because even a 1% rise in serum osmolality triggers thirst. When it does occur — particularly in the ICU — it is associated with 40–60% mortality and prolonged ICU stay.
Pathophysiology
The obligate daily water loss (~500 mL insensible + ~500 mL minimum urinary) creates a continuous need for water intake. If intake is less than this obligatory loss, tonicity rises. Hypernatremia therefore nearly always implies either:
- Impaired access to water / impaired thirst, or
- Ongoing hypotonic water losses that are not replaced
Neuronal cells lose water to the ECF → cellular dehydration → neurologic symptoms. In chronic hypernatremia, CNS cells accumulate intracellular osmoles (idiogenic osmoles) as an adaptive mechanism, which protects them acutely but makes rapid correction dangerous (risk of cerebral edema).
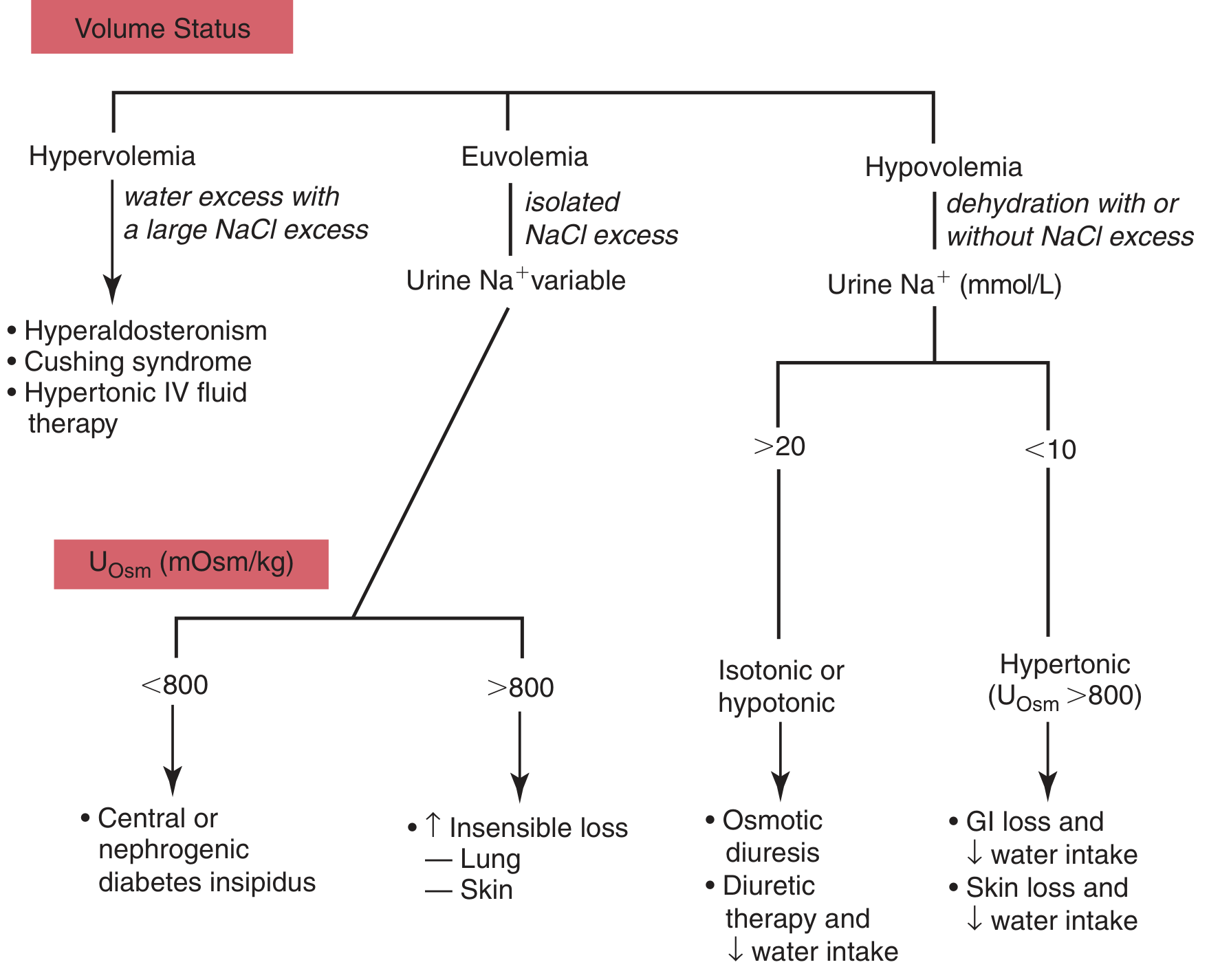
Classification & Causes
Classified by volume (ECF) status:
| Volume Status | Mechanism | Examples |
|---|---|---|
| Hypovolemic | Net loss of water > loss of sodium | GI losses (diarrhea, vomiting), skin losses (burns, fever, sweating), loop diuretics, osmotic diuresis |
| Euvolemic (Normovolemic) | Isolated water loss with NaCl excess or insensible loss | Central DI, nephrogenic DI, ↑ insensible losses (lung, skin) |
| Hypervolemic | Net Na⁺ gain > water gain | Hypertonic saline infusions, NaHCO₃, hyperaldosteronism, Cushing's syndrome, salt poisoning, AKI recovery phase |
Most cases arise in patients who cannot respond to thirst: altered mental status, infants, elderly, intubated/sedated ICU patients.
Diagnostic Algorithm
Step 1: Assess Volume Status (clinical exam)
- Skin turgor, mucous membranes, JVP, blood pressure, orthostatics, edema
Step 2: Urine Studies
If hypovolemic:
- Urine Na⁺ < 10–20 mmol/L + U_Osm > 800 mOsm/kg → extrarenal losses (GI, skin, respiratory) with intact renal conservation
- Urine Na⁺ > 20 mmol/L + U_Osm isotonic or hypotonic → renal losses (osmotic diuresis, diuretics)
If euvolemic/normovolemic with polyuria (>3 L/day):
- U_Osm < 250 mOsm/kg → water diuresis → diabetes insipidus (DI)
- Central DI: absent/reduced AVP → urine concentrates with desmopressin challenge
- Nephrogenic DI: renal resistance to AVP → no response to desmopressin
- U_Osm > 300 mOsm/kg → solute diuresis (e.g., osmotic diuresis of DM)
If euvolemic + concentrated urine → ↑ insensible losses (fever, tachypnea, sweating) without water replacement
If hypervolemic:
- U_Osm high (vasopressin release overrides hypervolemia stimulus)
- History of hypertonic fluid administration, AKI recovery, endocrine excess
Step 3: Confirm with Serum Osmolality
- Always elevated in true hypernatremia
- A spot urine osmolality < 100–200 mOsm/kg + polyuria → DI
- 24-h urine solutes > 800–1000 mOsm/day → osmotic diuresis
- 24-h urine solutes < 600 mOsm/day + dilute urine → DI
Clinical Manifestations
Primarily neurologic (due to osmotic water shift out of neurons):
| Severity | Symptoms |
|---|---|
| Mild | Thirst, irritability, tremors |
| Moderate | Ataxia, confusion, lethargy |
| Severe | Seizures, focal deficits, coma, death |
Key points:
- Acute hypernatremia: symptoms may appear at Na⁺ ~160 mmol/L
- Chronic hypernatremia: symptoms may not appear until Na⁺ > 175 mmol/L (due to idiogenic osmole accumulation)
- An awake alert patient with intact thirst who does not complain of thirst → suspect damage to hypothalamic osmoreceptors (primary hypodipsia)
Management
1. Correct Volume Depletion First (if hypovolemic)
If hemodynamically compromised or severely volume-contracted:
- Isotonic saline (0.9% NaCl) is the initial fluid of choice — restores tissue perfusion
- Rate guided by clinical parameters of volume restoration
- After perfusion is restored, switch to hypotonic replacement
2. Calculate the Free Water Deficit
$$\text{TBW deficit} = 0.4 \times \text{premorbid weight (kg)} \times \left(\frac{\text{Na}^+}{140} - 1\right)$$
(Use 0.5 for women and elderly; 0.4 for adult men)
3. Replace Water Deficit — Rate of Correction
⚠️ Never correct too fast — brain cells accumulated idiogenic osmoles; rapid water influx → cerebral edema
- Target reduction: ≤ 0.5–1.0 mmol/L/hour
- Maximum: ≤ 10–12 mmol/L in 24 hours (some sources say no more than 6–10 mmol/L/24h)
- Exception: Acute hypernatremia developing over minutes to hours (e.g., salt poisoning, iatrogenic hypertonic saline) → can be corrected more rapidly, as idiogenic osmoles have not had time to accumulate; rapid correction may prevent intracranial hemorrhage
4. Fluid Choice
| Setting | Preferred Fluid |
|---|---|
| Hypovolemia (hemodynamically unstable) | 0.9% NaCl initially, then transition |
| Water deficit replacement | D5W (free water) or 0.45% NaCl (half-normal saline) |
| Enteral access available | Oral tap water or hypotonic fluids via NGT |
| Hypervolemic hypernatremia | Hypotonic solutions + loop diuretic infusion ± extracorporeal removal |
5. Account for Ongoing Losses
In addition to the calculated deficit:
- Add ≥ 1 L/24h for insensible losses
- Add estimated ongoing renal or GI losses
- Total fluid requirement may reach 5–10 L over the correction period
6. Specific Cause Treatment
| Cause | Specific Treatment |
|---|---|
| Central DI | Intranasal or IV desmopressin (DDAVP) |
| Nephrogenic DI | Remove offending drug (lithium, demeclocycline); correct hypercalcemia/hypokalemia; thiazide diuretics + low-Na diet |
| Osmotic diuresis (DKA/HHS) | Insulin + fluid therapy |
| Hypervolemic (salt poisoning) | Hypotonic IV fluids ± loop diuretics; rapid correction acceptable in acute cases |
| Intradialytic hypernatremia | Cease dialysis; IV D5W; resume dialysis with dialysate Na⁺ ~2 mmol/L below plasma Na⁺ |
7. Monitoring
- Serum sodium every 4 hours during active correction
- Monitor for signs of volume overload (especially in cardiac/renal patients)
- Neurologic reassessment with each check
- Once Na⁺ is normalized, a patient with intact thirst will self-correct with oral intake
Key Causes of Diabetes Insipidus (Normovolemic Hypernatremia)
Central DI (↓ AVP secretion):
- Head trauma, neurosurgery/hypophysectomy, pituitary tumor, granulomatous disease, hypoxia
Nephrogenic DI (renal AVP resistance):
- Drugs: lithium, demeclocycline, foscarnet, cidofovir, vaptans, amphotericin
- Electrolytes: hypercalcemia, hypokalemia
- Systemic: sickle cell disease, Sjögren syndrome, amyloidosis
- Genetic: mutant V2 receptor or aquaporin-2
Summary Table
| Feature | Hypovolemic | Euvolemic | Hypervolemic |
|---|---|---|---|
| Volume exam | ↓ BP, dry mucosae | Normal | Edema, ↑ JVP |
| Urine Na⁺ | < 20 (extrarenal) or > 20 (renal) | Variable | High |
| Urine Osm | > 800 (extrarenal) or ↓ (renal/DI) | < 250 (DI) or > 800 (insensible) | High |
| Treatment | NS → D5W/0.45%NS | DDAVP (central DI); treat cause | Hypotonic + loop diuretic |
Sources:
- Goldman-Cecil Medicine, 27th Ed., pp. 1204–1206
- Tietz Textbook of Laboratory Medicine, 7th Ed., pp. 1940–1942
- Comprehensive Clinical Nephrology, 7th Ed., p. 1308
- Sabiston Textbook of Surgery and Miller's Anesthesia, 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.