All diseases under COPD
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, detailed content from multiple authoritative textbooks. Here is the complete answer:
Diseases Under COPD
COPD (Chronic Obstructive Pulmonary Disease) is an umbrella term for conditions that cause persistent airflow limitation due to airway and/or alveolar abnormalities, usually from exposure to noxious particles or gases (primarily cigarette smoke). Per Robbins Pathologic Basis of Disease, the COPD spectrum includes:
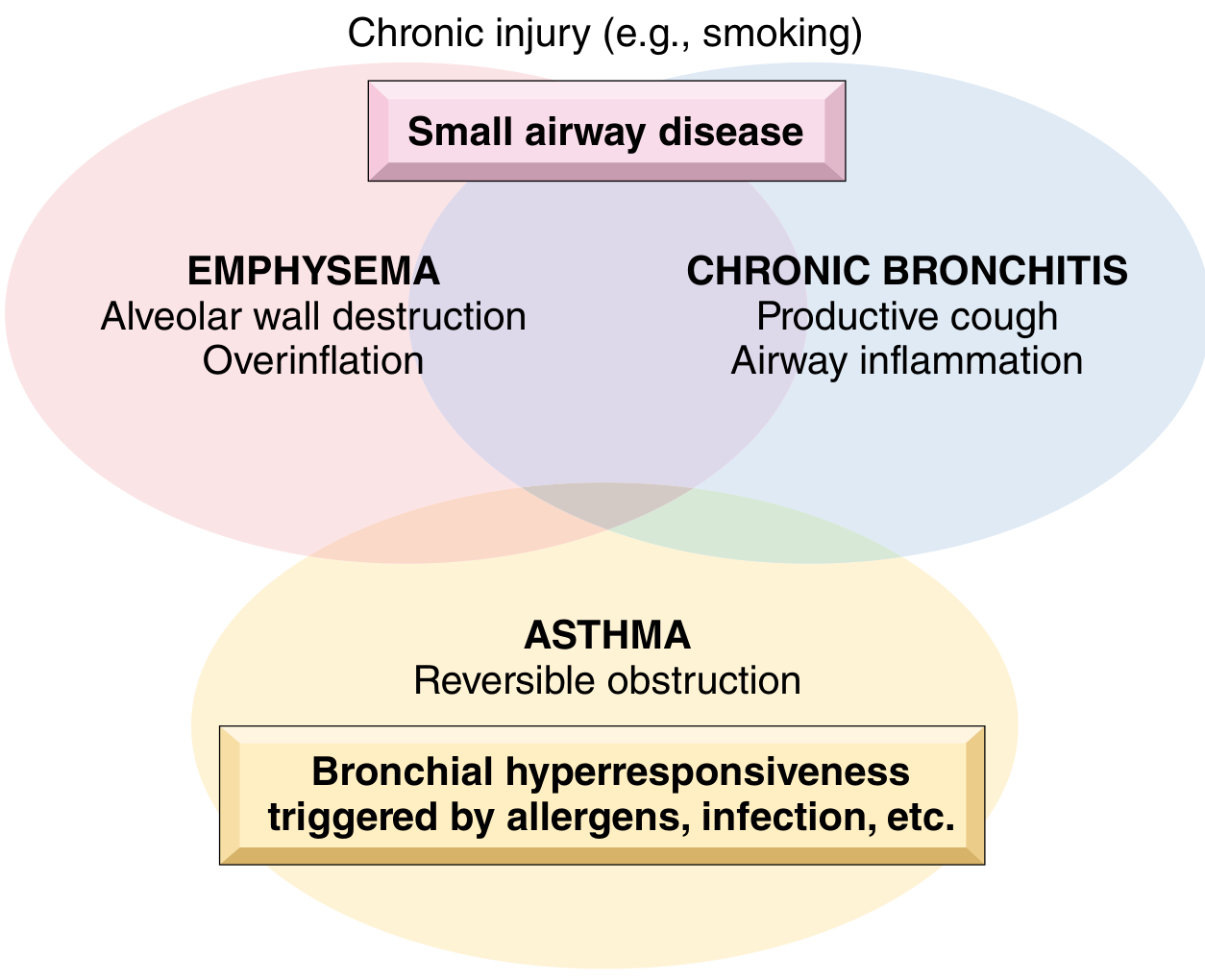
Diseases Classified Under / Associated with COPD
| Disease | Anatomic Site | Key Pathology | Etiology |
|---|---|---|---|
| Chronic Bronchitis | Bronchus | Mucous gland hyperplasia, mucus hypersecretion | Tobacco smoke, air pollutants |
| Emphysema | Acinus (alveoli) | Airspace enlargement, alveolar wall destruction | Tobacco smoke, α1-AT deficiency |
| Small Airway Disease / Bronchiolitis | Bronchiole | Inflammatory scarring, obliteration | Tobacco smoke, pollutants |
| Bronchiectasis | Bronchus | Airway dilation and scarring | Persistent/severe infections |
| Asthma (overlap) | Bronchus | Smooth muscle hyperplasia, excess mucus, inflammation | Immunologic/undefined |
(Source: Robbins Pathologic Basis of Disease, Table 16.3)
1. Emphysema
Definition: Irreversible enlargement of airspaces distal to the terminal bronchiole, with destruction of alveolar walls, without obvious fibrosis.
Emphysema is classified into four types based on the part of the acinus affected:
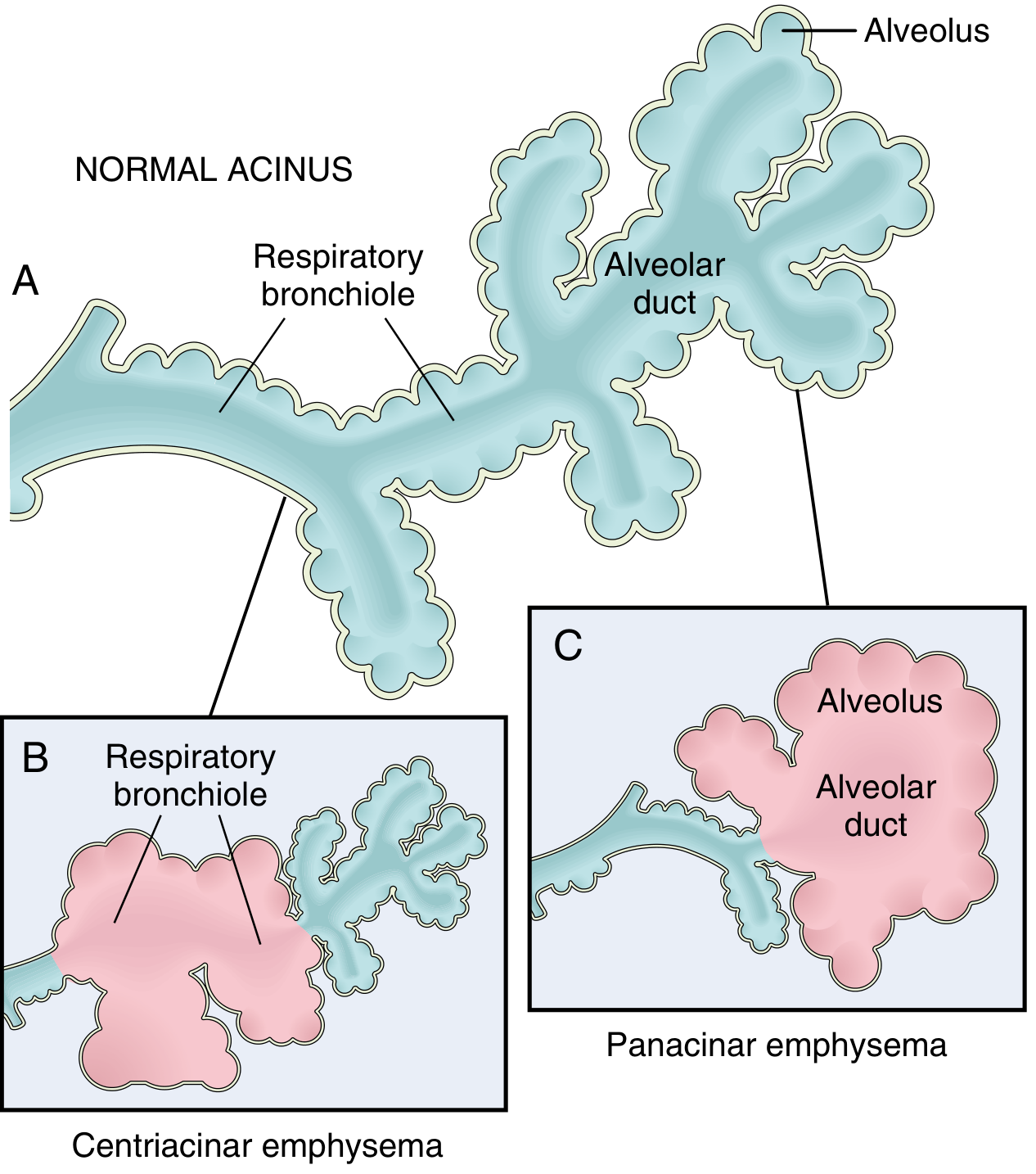
a. Centriacinar (Centrilobular) Emphysema - MOST COMMON
- Affects the central/proximal parts of the acini - the respiratory bronchioles - while distal alveoli are spared
- More than 95% of clinically significant emphysema
- Occurs predominantly in heavy smokers
- Predominantly affects upper lobes, particularly apical segments
- Both emphysematous and normal airspaces exist within the same acinus
b. Panacinar (Panlobular) Emphysema
- Acini are uniformly enlarged from the respiratory bronchiole to the terminal alveoli
- Associated with alpha-1 antitrypsin (α1-AT) deficiency; exacerbated by smoking
- Predominantly affects the lower lung zones and anterior margins
- In α1-AT deficiency, more severe in the lower lobes
c. Paraseptal (Distal Acinar) Emphysema
- Involves the distal part of the acinus - alveolar ducts and sacs - while the proximal portion is spared
- More severe in the upper half of the lungs
- Occurs adjacent to areas of fibrosis, scarring, or atelectasis
- Underlies many cases of spontaneous pneumothorax in young adults
- Typically not associated with significant airflow obstruction
d. Irregular Emphysema
- Acinus is irregularly involved and always associated with scarring (e.g., post-inflammatory scarring)
- Clinically the least important form
- Usually asymptomatic
Pathogenesis of Emphysema: Protease-antiprotease imbalance - neutrophils and macrophages release elastase and other proteases that destroy alveolar walls. In smokers, neutrophil count is increased in the lung AND antitrypsin is inactivated by tobacco smoke oxidants.
Clinical features (Emphysema-dominant = "Pink Puffer"):
- Barrel chest, hyperinflated lungs
- Pursed-lip breathing, sits hunched forward
- Dyspnea is the dominant symptom
- Cough is minimal
- Normal/near-normal blood gases at rest
- Low diffusion capacity (DLCO)
- Weight loss common
2. Chronic Bronchitis
Definition (clinical): Persistent productive cough for at least 3 consecutive months in at least 2 consecutive years - in the absence of another defined cause.
Pathology:
- Hypertrophy and hyperplasia of mucus-secreting glands in the trachea and bronchi
- Goblet cell metaplasia in smaller airways
- Reid Index >0.4 (ratio of mucous gland thickness to bronchial wall thickness) - normally 0.4
- Chronic airway inflammation (lymphocytes, macrophages), peribronchial fibrosis
- Small airway narrowing - bronchiolitis obliterans in severe cases
Pathogenesis:
- Tobacco smoke causes direct airway epithelial damage and impairs ciliary action
- Mucus overproduction: MUC5AC increased 10-fold, MUC5B increased 3-fold in severe COPD
- Acquired CFTR dysfunction from smoking leads to dehydrated, abnormal mucus
- Infection (H. influenzae etc.) does not initiate but maintains and exacerbates disease
Clinical features (Bronchitis-dominant = "Blue Bloater"):
- Chronic productive cough with copious sputum
- Hypoxemia and hypercapnia (cyanosis = "blue")
- Cor pulmonale (right heart failure) - peripheral edema ("bloater")
- Prone to recurrent respiratory infections
3. Small Airway Disease (Chronic Bronchiolitis)
- Inflammation and fibrosis of bronchioles (<2-3 mm diameter)
- A key early driver of COPD - develops before emphysema or symptomatic airflow obstruction
- Small airways become narrowed by cellular hyperplasia, mucus, and fibrosis
- Present in nearly all COPD patients; correlates with degree of airflow obstruction
- In severe cases, leads to bronchiolitis obliterans (obliterative bronchiolitis)
4. Bronchiectasis (part of the obstructive spectrum)
- Permanent dilation and scarring/destruction of bronchial walls
- Can coexist with COPD but has a distinct etiology: persistent or severe infections, cystic fibrosis, immunodeficiency
- Presents with chronic cough, purulent (green/yellow) sputum, recurrent fever
- Considered part of the obstructive airway disease spectrum
5. Asthma-COPD Overlap (ACO)
While asthma is primarily a reversible obstructive disease (vs. COPD which is irreversible), there is meaningful overlap. Some asthma patients develop an irreversible component (airway remodeling), and some COPD patients have a reversible component - clinically labeled COPD/Asthma overlap or ACO (Asthma-COPD Overlap).
Key Distinguishing Features: "Pink Puffer" vs "Blue Bloater"
| Feature | Pink Puffer (Emphysema) | Blue Bloater (Chronic Bronchitis) |
|---|---|---|
| Main complaint | Dyspnea | Cough + sputum |
| Cyanosis | Absent or late | Present early |
| Hypoxemia | Mild (at rest) | Severe |
| Hypercapnia | Absent | Present |
| Cor pulmonale | Late | Early |
| DLCO | Reduced | Normal |
| Body habitus | Thin, barrel chest | Overweight, cyanotic |
| Breath sounds | Quiet | Rhonchi, wheezes |
Summary
Per Goldman-Cecil Medicine: "COPD is an umbrella term for a number of conditions that result in fixed airway obstruction... nearly all patients have both the air space destruction associated with emphysema as well as the pathologic airway changes that are consistent with chronic bronchitis."
The main diseases under COPD are:
- Emphysema (centriacinar, panacinar, paraseptal, irregular)
- Chronic Bronchitis
- Small Airway Disease / Chronic Bronchiolitis
- Bronchiectasis (related obstructive disease)
- Asthma-COPD Overlap (ACO) - in patients with mixed features
Sources: Robbins Pathologic Basis of Disease; Goldman-Cecil Medicine; Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine 22E.
This is a shared conversation. Sign in to Orris to start your own chat.