Hey I'm preparing for CVS physiology
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I have everything needed. Here is your comprehensive explanation:
CVS Physiology: Action Potentials & Conduction
1. The Resting Membrane Potential
Before any action potential, cardiac cells sit at a stable negative resting membrane potential:
- Working cells (atria, ventricles, Purkinje): about -85 to -90 mV
- SA / AV node: about -50 to -65 mV (less negative, because these cells have lower K+ permeability at rest)
The resting potential is set primarily by K+ - at rest, the membrane is highly permeable to K+, so the potential sits close to the K+ equilibrium potential (~-94 mV). Na+ contributes very little at rest because its conductance (gNa) is low.
2. Ventricular / Atrial / Purkinje Action Potential (5 Phases)
These three tissue types share the same basic ionic mechanism.
| Phase | Name | Key Ion Movement | What happens |
|---|---|---|---|
| 0 | Upstroke | Na+ in (fast, via voltage-gated Na+ channels) | Rapid depolarization from -90 mV to ~+30 mV |
| 1 | Initial repolarization | Na+ channels inactivate; K+ out (Ito) | Brief, small dip downward |
| 2 | Plateau | Ca2+ in (L-type channels) balances K+ out | Membrane stays depolarized 150-200 ms |
| 3 | Repolarization | gCa decreases; gK increases (IK) - K+ out | Rapid return to resting potential |
| 4 | Stable resting potential | K+ permeability keeps potential stable at ~-90 mV | No spontaneous firing (unlike SA node) |
Key clinical link - the plateau (Phase 2):
- The inward Ca2+ through L-type channels triggers Ca2+-induced Ca2+ release from the sarcoplasmic reticulum (SR)
- This is what couples the electrical signal to mechanical contraction (excitation-contraction coupling)
- Ca2+ channel blockers (nifedipine, diltiazem, verapamil) inhibit these L-type channels
Refractory period: From Phase 0 until the cell repolarizes back to -60 mV during Phase 3, the cell cannot fire again. This prevents tetanic contraction of the heart (unlike skeletal muscle).
Action potential durations:
- Atrium: ~150 ms
- Ventricle: ~250 ms
- Purkinje fibers: ~300 ms (longest - hence the last latent pacemaker)
3. SA Node Action Potential - The Pacemaker
The SA node is fundamentally different because it generates action potentials spontaneously (automaticity).
Three key differences from ventricular cells:
- No stable resting potential - it spontaneously depolarizes
- No fast Na+ upstroke - the upstroke uses Ca2+ (L-type + T-type channels)
- No plateau (Phases 1 and 2 are absent)
SA Node Phases:
Phase 0 (Upstroke) - Carried by inward Ca2+ current (L-type channels), NOT Na+. This is why the upstroke is slower and less steep than in ventricular cells.
Phases 1 & 2 - ABSENT.
Phase 3 (Repolarization) - Increase in gK, outward K+ current repolarizes the cell back to maximum diastolic potential (~-65 mV).
Phase 4 (Pacemaker Potential / Spontaneous Depolarization) - This is the hallmark of the SA node:
- The membrane does NOT stay at -65 mV - it slowly drifts upward toward threshold
- Driven by If ("funny current") - an inward Na+ current activated by repolarization itself
- Once If carries the membrane to threshold, L-type Ca2+ channels open and fire the next action potential
- This repeats automatically, giving the SA node its intrinsic firing rate of ~60-100/min
Heart rate control via Phase 4:
- Sympathetic (norepinephrine): Speeds up Phase 4 depolarization → threshold reached faster → heart rate ↑
- Parasympathetic (acetylcholine): Slows Phase 4 depolarization → threshold reached slower → heart rate ↓
4. Conduction Through the Heart
The action potential follows a specific, ordered pathway:
SA node → Atrial muscle → AV node → Bundle of His → Left & Right bundle branches → Purkinje fibers → Ventricular muscle
Conduction Velocities (very important for exams!):
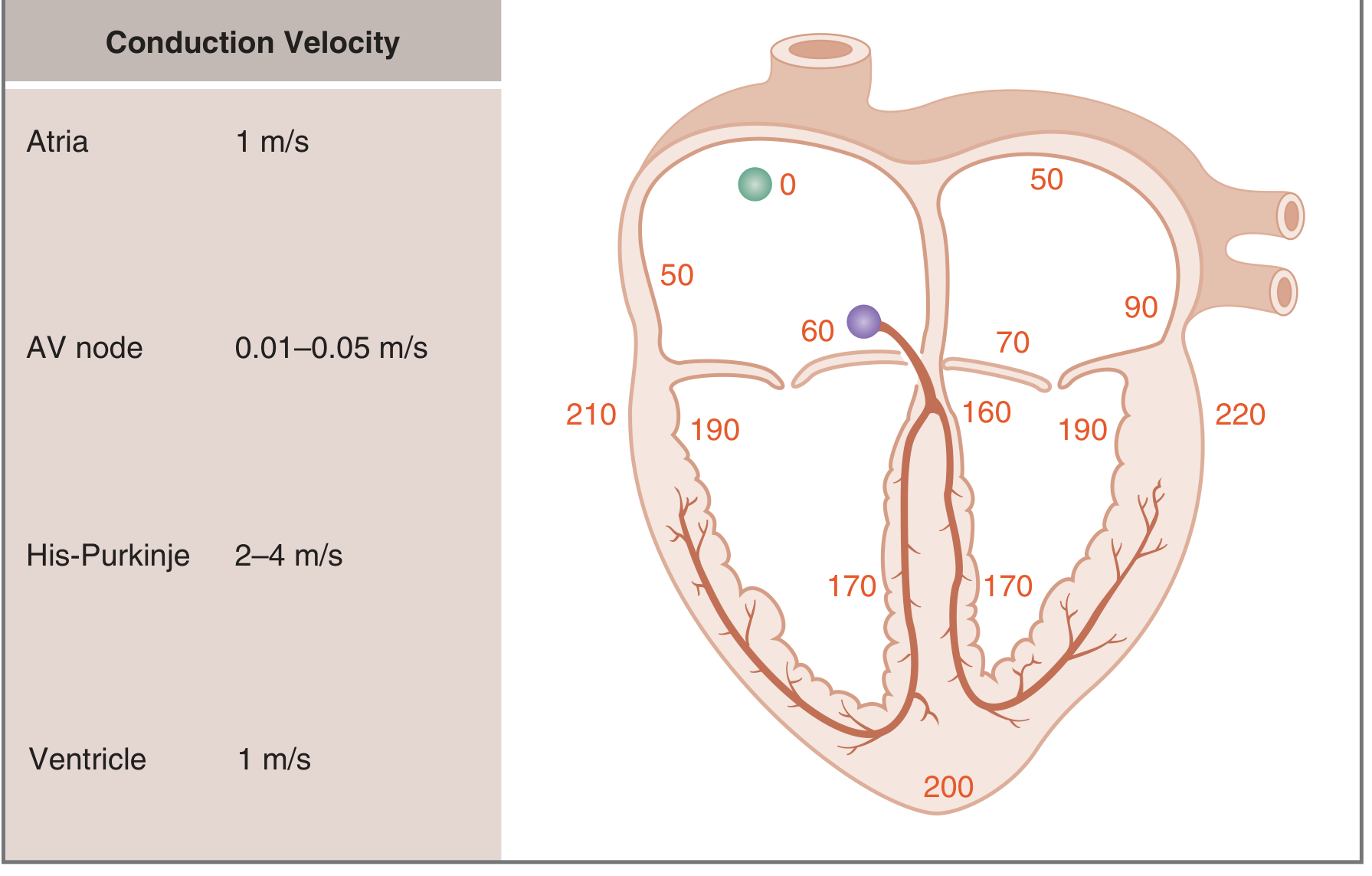
| Tissue | Conduction Velocity | Timing from SA node |
|---|---|---|
| Atria | 1 m/s | 0-90 ms |
| AV node | 0.01-0.05 m/s (slowest!) | ~100 ms delay |
| His-Purkinje | 2-4 m/s (fastest!) | 160-170 ms |
| Ventricles | 1 m/s | 170-220 ms |
Total time from SA node to furthest ventricle = ~220 ms
Why is the AV node slow on purpose?
The AV delay (~100 ms) ensures the ventricles have time to fill with blood from the atria before contracting. Without this delay, the atria and ventricles would contract simultaneously and ventricular filling would be incomplete.
Why are Purkinje fibers fast?
Their speed (2-4 m/s) ensures the entire ventricular myocardium depolarizes rapidly and synchronously so the ventricles contract as a unit and eject blood efficiently.
5. Mechanism of Propagation - Local Currents
Action potentials spread by local current flow - the same principle as in nerve fibers:
- An excited cell has an inward current during Phase 0 (Na+ in for working cells; Ca2+ in for SA node)
- This creates a voltage difference with the adjacent resting cell
- Current flows from the excited cell to the resting cell through gap junctions (connexins)
- The adjacent cell depolarizes to threshold and fires its own action potential
- The process repeats cell-by-cell
Conduction velocity depends on:
- Size of the inward current during Phase 0 (larger current = faster propagation)
- Rate of rise of Phase 0 (dV/dT) - correlates with inward current size
- Cable properties of the tissue (resistance, capacitance, gap junction density)
6. Quick Comparison Table
| Feature | SA Node | Ventricular Cell |
|---|---|---|
| Resting potential | ~-65 mV (unstable) | ~-90 mV (stable) |
| Phase 0 carrier | Ca2+ (L+T type) | Na+ (fast) |
| Phase 4 | Spontaneous depolarization (If) | Flat (no automaticity) |
| Plateau | Absent | Present (150-200 ms) |
| Automaticity | Yes - primary pacemaker | No |
7. Normal Sinus Rhythm - 3 Criteria
- Action potential originates in the SA node
- SA nodal impulses occur regularly at 60-100/min
- Activation of the myocardium occurs in the correct sequence with correct timing
Sources: Costanzo Physiology 7th Edition, pp. 138-144; Braunwald's Heart Disease, Chapter 62
Want me to go deeper on any specific part - such as autonomic effects on the SA node, the ionic currents in more detail, refractory periods and their clinical relevance, or how this connects to ECG waveforms?
This is a shared conversation. Sign in to Orris to start your own chat.