Rhumetaoid arthritis
Reading File
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND treatment
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND "biological therapy"[MeSH Terms]
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Harrison's 22E, Firestein & Kelley's Rheumatology, and Robbins Pathology. I have enough to compile a thorough, well-organized answer on Rheumatoid Arthritis.
Rheumatoid Arthritis (RA)
A chronic, systemic autoimmune disease characterized by symmetric, erosive polyarthritis with extra-articular manifestations. It affects approximately 0.5-1% of adults worldwide, with a 2-3:1 female predominance, peak onset in the 4th-5th decade.
Pathogenesis
The diagram below (from Robbins & Kumar) illustrates the key steps:
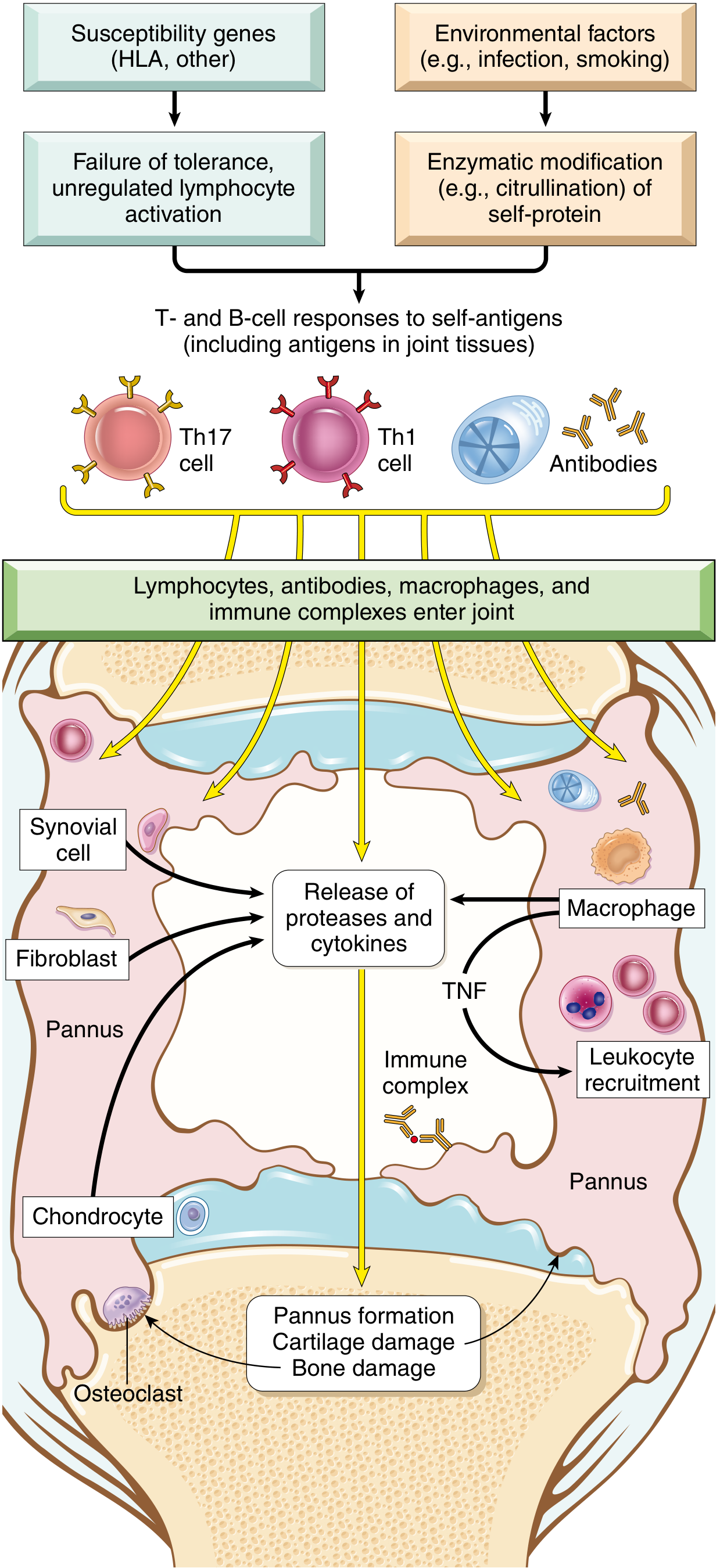
Genetic factors:
- ~50% of RA risk is inherited. The HLA-DR4 allele ("shared epitope") is strongly associated with ACPA-positive RA. HLA-DRB1 alleles that carry the shared epitope increase RA risk 4-6 fold; combined with smoking, this rises to 20-40 fold.
Environmental triggers:
- Smoking is the most reproducible risk factor: confers a relative risk of 1.5-3.5x. Risk is almost exclusively tied to RF/ACPA-positive disease and persists 15 years after cessation.
- Periodontal disease / oral microbiome: Porphyromonas gingivalis is uniquely capable of PAD (peptidyl arginine deiminase) enzyme production, catalyzing citrullination of host proteins - creating neo-antigens that trigger autoimmunity.
- Gut microbiome dysbiosis: Prevotella copri enrichment has been found in early untreated RA.
- EBV has been implicated but causation is unproven.
Autoantibodies:
- Anti-citrullinated protein antibodies (ACPA / anti-CCP): Present in ~70% of RA patients. Arginine residues in fibrinogen, type II collagen, vimentin, and α-enolase are citrullinated by PAD enzymes; these modified epitopes trigger autoimmunity. ACPAs may appear >10 years before clinical disease.
- Rheumatoid factor (RF): IgM/IgA autoantibodies against the Fc region of IgG, present in ~80% of patients. Not RA-specific.
Effector mechanisms in the joint:
- CD4+ Th1 cells secrete IFN-γ → activate macrophages and synovial cells
- Th17 cells secrete IL-17 → recruit neutrophils and monocytes
- TNF is a key mediator of inflammation and joint destruction (basis for biologic therapy)
- Macrophages and synovial fibroblasts release proteases (MMPs), prostaglandins, and cytokines (IL-1, IL-6, TNF)
- RANKL from activated T cells stimulates osteoclasts → bone resorption
- B cells and plasma cells form germinal centers in the synovium; secrete RF and ACPAs
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p.1106; Harrison's Principles 22E, pp.2891-2892; Firestein & Kelley's Textbook of Rheumatology
Pathology / Morphology
The hallmarks are synovial inflammation, proliferation, focal bone erosions, and thinning of articular cartilage.
- Synovium becomes edematous, thickened, and hyperplastic - smooth contour replaced by delicate, bulbous villi
- Pannus formation: a mass of edematous synovium, inflammatory cells, granulation tissue, and fibroblasts that invades cartilage and bone. Composed of 6 cell types: T cells, B cells, plasma cells, dendritic cells, mast cells, granulocytes
- Histologic features: (1) Synovial cell hyperplasia/proliferation; (2) dense CD4+ T cell, B cell, plasma cell, macrophage infiltrates (often forming lymphoid follicles); (3) increased vascularity (angiogenesis); (4) fibrin-rich neutrophilic exudate on synovial surfaces; (5) osteoclastic subchondral bone erosion
- Bone damage: Osteoclasts at the pannus-bone interface form resorption lacunae, especially at radial sites of MCP joints
- Periarticular osteopenia: From bone marrow inflammation; visible as MRI signal alterations ("bone marrow lesions") - a forerunner of frank erosions
- End-stage: Fibrous ankylosis → ossification → bony ankylosis (bone fusion)
Rheumatoid nodules: Occur in ~20% of RF-positive patients. Firm, nontender subcutaneous masses at forearms, elbows, occiput, and lumbosacral area. Microscopically - central zone of fibrinoid necrosis surrounded by palisading activated macrophages and lymphocytes/plasma cells.
- Robbins, Cotran & Kumar, pp.1106-1107; Harrison's 22E, pp.2890-2891
Clinical Features
Onset:
- Often insidious - malaise, fatigue, generalized musculoskeletal pain in ~50% of patients, followed by joint involvement over weeks to months
- Can also have acute polyarticular onset
Joint involvement (symmetric):
- Small joints first: MCP and PIP joints of hands (sparing DIP - key distinction from OA), MTP joints of feet
- Then: wrists, ankles, elbows, knees
- Morning stiffness >1 hour (worse after inactivity - "gelling")
- Joints are swollen, warm, tender, and painful
Characteristic deformities (late disease):
- Ulnar deviation of fingers at MCPs
- Swan-neck deformity: PIP hyperextension + DIP flexion
- Boutonniere deformity: PIP flexion + DIP hyperextension
- Z-deformity of the thumb
- Subluxation of the carpus, atlantoaxial subluxation (C1-C2, causing neck pain/myelopathy risk)
Extra-articular manifestations:
| System | Manifestations |
|---|---|
| Skin | Rheumatoid nodules, vasculitis |
| Pulmonary | Interstitial lung disease, pleuritis, nodules, Caplan's syndrome (with pneumoconiosis) |
| Cardiac | Pericarditis, accelerated atherosclerosis (major cause of excess mortality) |
| Ocular | Keratoconjunctivitis sicca (secondary Sjogren's), scleritis, episcleritis |
| Hematologic | Normocytic normochromic anemia, Felty's syndrome (RA + splenomegaly + neutropenia) |
| Neurologic | Mononeuritis multiplex (from vasculitis), entrapment neuropathies, cervical myelopathy |
| Renal | Secondary amyloidosis (AA type) |
Diagnosis
2010 ACR/EULAR Classification Criteria (score ≥6/10 = definite RA):
| Domain | Score |
|---|---|
| Joint involvement: 1 large joint = 0; 2-10 large = 1; 1-3 small = 2; 4-10 small = 3; >10 joints (including ≥1 small) = 5 | 0-5 |
| Serology: Negative RF and ACPA = 0; Low-positive = 2; High-positive (>3x ULN) = 3 | 0-3 |
| Acute phase reactants: Normal CRP & ESR = 0; Abnormal CRP or ESR = 1 | 0-1 |
| Duration of symptoms: <6 weeks = 0; ≥6 weeks = 1 | 0-1 |
Serology:
- ACPA (anti-CCP): ~70% sensitivity, >95% specificity - the most specific test; predicts erosive disease
- RF: ~80% sensitivity but low specificity (also positive in SLE, Sjogren's, chronic infections, healthy elderly)
- ~20% of RA patients are seronegative (negative for both)
- ESR and CRP: elevated in active disease
- CBC: normocytic anemia, thrombocytosis in active disease
Imaging:
- X-ray: periarticular osteopenia, joint space narrowing, marginal erosions (especially radial aspects of MCPs), deformities
- MRI: earliest detection of synovitis and bone marrow edema (precedes erosions)
- Ultrasound: detects subclinical synovitis and tenosynovitis
Disease activity assessment tools (used in clinical practice):
- DAS28 (Disease Activity Score - 28 joints)
- SDAI (Simplified Disease Activity Index)
- CDAI (Clinical Disease Activity Index)
- ACR 20/50/70 improvement criteria (used in clinical trials)
Treatment
The goal is remission or low disease activity using a treat-to-target strategy.
1. NSAIDs
- Adjunctive only; provide symptomatic relief but do not alter disease course
- Inhibit COX-1 and COX-2; risk of GI and renal toxicity with chronic use
2. Glucocorticoids
- Bridge therapy while awaiting DMARD effect (onset may take weeks-months)
- Low-dose prednisone 5-10 mg/d for active disease
- Short bursts for flares
- Minimize long-term use due to osteoporosis, infection, metabolic effects
3. Conventional (csDMARDs)
| Drug | Dose | Key Toxicities | Monitoring |
|---|---|---|---|
| Methotrexate (first choice) | 10-25 mg/week PO or SQ + folic acid 1 mg/d | Hepatotoxicity, myelosuppression, pneumonitis, teratogen | CBC, LFTs, creatinine q2-3 months |
| Hydroxychloroquine | 200-400 mg/d (≤5 mg/kg) | Irreversible retinopathy, cardiotoxicity | Annual OCT + visual field |
| Sulfasalazine | 1000-1500 mg/d (start 500 mg BD) | Granulocytopenia, hemolytic anemia (G6PD deficiency) | CBC q2-4 weeks x 3 months, then q3 months |
| Leflunomide | 10-20 mg/d | Hepatotoxicity, myelosuppression, teratogen (Category X) | CBC, LFTs q2-3 months |
Triple therapy (MTX + HCQ + SSZ) is as effective as biologic therapy in many patients.
4. Biologic DMARDs (bDMARDs)
Used when csDMARDs fail (typically after 3-6 months of adequate MTX):
| Class | Examples | Notes |
|---|---|---|
| TNF-α inhibitors | Infliximab, Etanercept, Adalimumab, Certolizumab, Golimumab | First-line biologics; screen for TB before starting; risk of reactivation of latent TB, fungal infections, lymphoma (controversial) |
| IL-6 receptor inhibitor | Tocilizumab, Sarilumab | Also used for cytokine release syndrome; may mask fever/CRP |
| T cell costimulation blocker | Abatacept (CTLA-4-Ig) | Blocks CD28-CD80/86 interaction |
| B cell depletor | Rituximab (anti-CD20) | Preferred in RF/ACPA-high disease or with comorbid lymphoma |
| IL-1 inhibitor | Anakinra | Less commonly used for RA |
5. JAK Inhibitors (targeted synthetic DMARDs - tsDMARDs)
- Tofacitinib, Baricitinib, Upadacitinib
- Oral agents; inhibit Janus kinase signaling
- Used when bDMARDs fail or as alternatives; black box warnings for infection, malignancy, thromboembolism, MACE in patients >50 with CV risk factors
- Harrison's Principles of Internal Medicine 22E (2025), pp.2892-2896
Prognosis
- Chronic, waxing-and-waning course in most patients; progressive joint damage without DMARD therapy
- ~20% of seronegative patients may stabilize or remit
- Major causes of excess mortality: accelerated cardiovascular disease (most common), infections, cervical myelopathy
- Poor prognostic factors: high ACPA/RF titers, high disease activity at onset, early erosions on imaging, extra-articular disease, functional disability
Key Distinguishing Points (RA vs OA)
| Feature | RA | OA |
|---|---|---|
| Joint type affected | MCP, PIP, wrists | DIP, PIP, first CMC, weight-bearing |
| Symmetry | Symmetric | Often asymmetric |
| Morning stiffness | >1 hour | <30 minutes |
| Inflammation | Prominent | Mild |
| Systemic features | Yes | No |
| Serologic markers | RF, ACPA | Negative |
| X-ray | Erosions, osteopenia | Osteophytes, sclerosis, joint space narrowing |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22E (2025); Firestein & Kelley's Textbook of Rheumatology 2-Volume Set
This is a shared conversation. Sign in to Orris to start your own chat.