mechanism of normal labour
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library does not appear to have a dedicated obstetrics textbook, so I'll answer from well-established knowledge - this is a foundational topic with no variation in current guidelines.
Mechanism of Normal Labour
Normal labour describes the series of coordinated, sequential movements a fetus makes as it negotiates the maternal pelvis during birth. These movements are collectively called the cardinal movements (mechanisms) of labour. They are passive movements of the fetus brought about by uterine contractions and the resistance offered by the birth canal.
Prerequisites: The Passengers, Passage, and Powers
Before understanding the mechanism, three key factors set the stage:
- Passenger - fetus (size, lie, presentation, position, attitude)
- Passage - bony pelvis and soft tissues
- Powers - uterine contractions + maternal pushing (bearing-down efforts)
The most common scenario - and the basis of the "normal" mechanism - is the vertex presentation, occipito-anterior position (LOA or OA) in a gynaecoid pelvis.
The Seven Cardinal Movements
1. Engagement
- The biparietal diameter (BPD) of the fetal head passes through the pelvic inlet (plane of the brim).
- In primigravidae, engagement typically occurs 2-4 weeks before labour (lightening); in multigravidae, it may occur only during labour.
- The head enters the inlet in the transverse or oblique diameter (widest diameter of the inlet = 13 cm transverse).
- The occiput is usually directed to the left or right iliac fossa (LOT or ROT most common).
2. Descent
- Descent is progressive throughout labour, accelerating during the second stage.
- It occurs throughout all other cardinal movements - no single stage is descent-exclusive.
- Caused by: uterine contractions, bearing-down efforts, fundal pressure, and the weight of the fetus.
3. Flexion
- As the head descends and meets resistance from the pelvic floor, the chin is brought closer to the chest.
- This converts the presenting diameter from the occipito-frontal (11.5 cm) to the smaller suboccipito-bregmatic diameter (9.5 cm) - the smallest diameter of the fetal head.
- Flexion is mostly passive; it occurs because the force of contractions acts eccentrically on the fetal head.
4. Internal Rotation
- The occiput rotates from its lateral position (usually LOT - left occiput transverse) to the anterior position (OA - occiput anterior), underneath the pubic symphysis.
- This rotation of 45-90 degrees occurs as the head reaches the ischial spines (mid-cavity).
- The ischial spines and the levator ani muscles guide this rotation.
- The widest transverse diameter of the fetal head now aligns with the widest antero-posterior diameter of the pelvic outlet.
- In LOT: the occiput rotates 90° forward (counterclockwise when viewed from below).
- In LOA: the occiput rotates only 45° forward.
5. Extension
- As the fully flexed, internally rotated head reaches the pelvic outlet, it must extend to negotiate the curve of the birth canal (Carus' curve).
- The occiput escapes under the pubic symphysis (the suboccipital region pivots on the inferior border of the pubic symphysis = the fulcrum).
- The head extends, and the following parts are delivered in sequence: occiput → bregma → forehead → nose → mouth → chin.
- This movement delivers the head.
6. Restitution (External Rotation - Part 1)
- Once the head is delivered, it undergoes restitution - it rotates back 45° to align with the position it occupied before internal rotation.
- This restores the natural relationship between the head and the shoulders (the neck untwists).
- If the occiput rotated to OA from LOA, it now rotates 45° back to face the left maternal thigh.
7. External Rotation (Part 2) + Expulsion
- The shoulders now undergo their own internal rotation (the anterior shoulder rotates under the pubic symphysis).
- This causes the already-delivered head to rotate a further 45°, so the occiput now faces directly laterally (toward the mother's inner thigh).
- The anterior shoulder is delivered first from under the pubic symphysis, then the posterior shoulder over the perineum.
- The rest of the body follows easily by lateral flexion.
Summary Table
| Step | Movement | What Happens |
|---|---|---|
| 1 | Engagement | BPD passes through inlet |
| 2 | Descent | Progressive downward movement |
| 3 | Flexion | Chin on chest; smallest diameter presents |
| 4 | Internal rotation | Occiput rotates to anterior (OA) |
| 5 | Extension | Head delivered under pubic symphysis |
| 6 | Restitution | Head realigns with shoulders |
| 7 | External rotation | Shoulders rotate internally; body delivered |
Key Diameters to Remember
| Diameter | Measurement | When It Matters |
|---|---|---|
| Suboccipito-bregmatic | 9.5 cm | Fully flexed vertex - ideal |
| Occipito-frontal | 11.5 cm | Deflexed vertex |
| Suboccipito-frontal | 10.5 cm | Partially flexed |
| Mento-vertical | 13.5 cm | Face presentation (brow) - cannot deliver vaginally |
| Biparietal (BPD) | 9.5 cm | Engages in transverse diameter of inlet |
Stages of Labour (Context)
The mechanism above unfolds across three stages:
- First stage - Onset of true labour to full dilation (10 cm). Divided into latent (0-6 cm) and active (6-10 cm) phases. Engagement, early descent, and beginning of flexion occur here.
- Second stage - Full dilation to delivery of the baby. All cardinal movements complete during this stage.
- Third stage - Delivery of the placenta (5-30 minutes after delivery).
Mnemonic
"Every Damn Fool In England Runs Everywhere"
Engagement → Descent → Flexion → Internal rotation → Extension → Restitution → External rotation
mechanism of normal labour
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive textbook content and two clinical diagrams. Here is the full answer:
Mechanism of Normal Labour (Cardinal Movements)
Normal labour describes the series of coordinated movements the fetus makes to negotiate the maternal pelvis. These are known as the cardinal movements of labour - seven sequential, mostly passive movements driven by uterine contractions and the resistance of the birth canal. They apply to the most common presentation: vertex (occiput anterior).
"The fetus will follow the path of least resistance by adaptation of the smallest achievable diameter of the presenting part to the most favourable dimensions and contours of the birth canal."
- Roberts & Hedges' Clinical Procedures in Emergency Medicine
The Three P's - Setting the Stage
| Factor | Details |
|---|---|
| Powers | Uterine contractions + maternal bearing-down efforts |
| Passenger | Fetus - size, lie, presentation, position, attitude |
| Passage | Bony pelvis (inlet, mid-cavity, outlet) + soft tissues |
The Seven Cardinal Movements
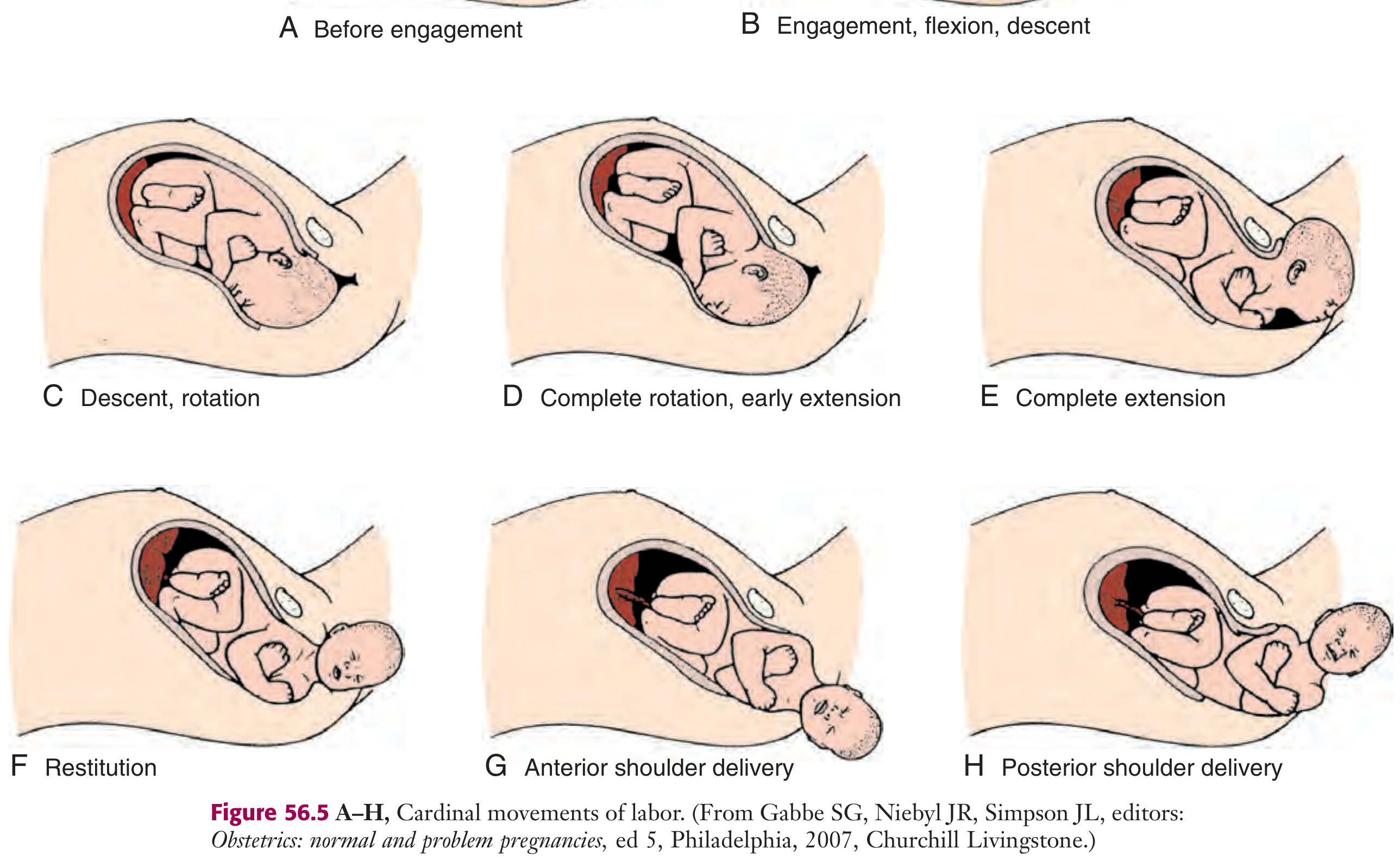
Figure: Cardinal movements A-H: Before engagement → Engagement, flexion, descent → Descent, rotation → Complete rotation, early extension → Complete extension → Restitution → Anterior shoulder delivery → Posterior shoulder delivery. From Gabbe SG et al., Obstetrics: Normal and Problem Pregnancies.
1. Engagement
- The biparietal diameter (BPD = 9.5 cm) - the greatest transverse diameter of the head - passes through the pelvic inlet.
- The fetus is engaged when the presenting part reaches 0 station (level of the ischial spines).
- In primigravidae: usually occurs 2-4 weeks before labour onset (lightening).
- In multigravidae: may occur only at the onset of labour.
- The head enters the inlet in the transverse or oblique diameter (the widest diameter of the pelvic inlet).
- Clinically confirmed when the occiput is palpated at or below the ischial spines on vaginal examination.
2. Descent (occurs throughout)
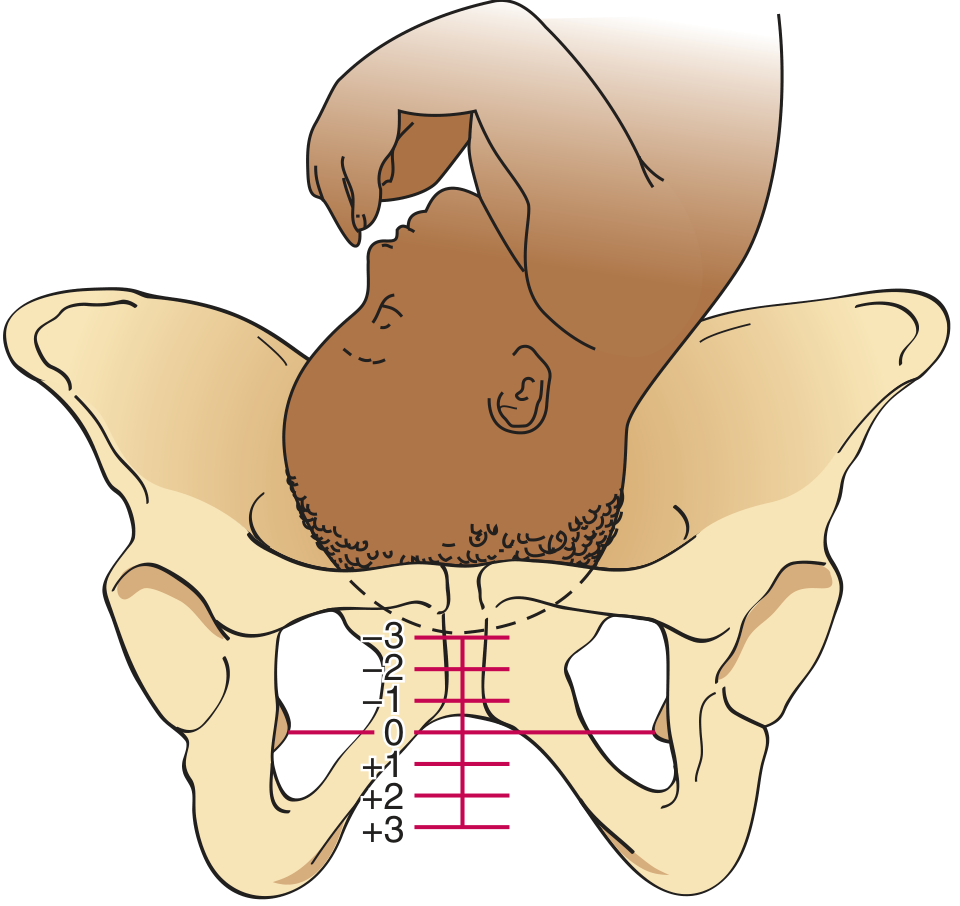
Figure: Station measurement. 0 station = fetal vertex at the level of ischial spines. Negative stations (-1, -2, -3) = above the spines; positive stations (+1, +2, +3) = below the spines.
- Downward passage of the fetal presenting part through the birth canal.
- Gradual and progressive throughout all stages but not always continuous.
- Measured in stations: centimetres above (-1 to -3) or below (+1 to +3) the ischial spines.
- Driven by: uterine contractions, bearing-down efforts, straightening of the fetal body.
- Normal rate: ≥1 cm/hour in nulliparas, ≥2 cm/hour in multiparas during active phase.
3. Flexion
- As the head descends and meets resistance from the pelvic floor and cervix, the chin is forced onto the chest.
- Converts the presenting diameter from the occipito-frontal (11.5 cm) to the suboccipito-bregmatic (9.5 cm) - the smallest diameter.
- This is a passive movement in most cases.
- The posterior fontanelle is ideally centred in the dilating cervix, allowing optimal moulding of cranial bones.
- Infants in the occipito-posterior (OP) position are often "deflexed," presenting a larger, less favourable diameter.
4. Internal Rotation
- As the head descends through the mid-cavity and approaches the ischial spines, the occiput rotates anteriorly toward the pubic symphysis.
- In LOT (left occiput transverse): rotates 90° to OA (occiput anterior).
- In LOA (left occiput anterior): rotates 45° to OA.
- The final position is most commonly LOA, OA, or ROA; in ~5-10% of cases the vertex presents as OP (occiput posterior).
- This rotation aligns the biparietal diameter with the widest diameter (intertuberous = transverse) of the pelvic outlet.
- Guided by the shape of the levator ani muscles and the ischial spines.
5. Extension
- As the fully flexed, internally rotated head reaches the pelvic outlet, it must extend to follow the curve of the birth canal (Carus' curve).
- The suboccipital region pivots under the pubic symphysis (the inferior border of the symphysis acts as a fulcrum).
- The head extends around the pubic bone, and the following parts are delivered sequentially: occiput → bregma → forehead → nose → mouth → chin.
- Extension occurs rapidly and is clinically observed when the perineum distends.
- Immediately after birth, the head drops downward so the chin lies over the maternal anal region.
6. Restitution (External Rotation - Part 1)
- After the head is delivered, it rotates back to the transverse position it occupied at engagement (the neck untwists).
- If the occiput rotated from LOA to OA during internal rotation, it now rotates 45° back toward the left maternal thigh.
- This is a passive movement restoring the natural anatomical relationship between the head and fetal shoulders.
7. Expulsion (External Rotation - Part 2 + Delivery of Shoulders and Body)
- The shoulders undergo their own internal rotation - the bisacromial diameter rotates into the anteroposterior plane.
- This causes the already-delivered head to rotate a further 45°, so the occiput faces directly laterally.
- Anterior shoulder is delivered first from beneath the pubic symphysis.
- Posterior shoulder is then delivered over the perineum.
- The rest of the body follows easily by lateral flexion of the trunk.
Summary Table
| # | Movement | Key Point |
|---|---|---|
| 1 | Engagement | BPD passes inlet; 0 station |
| 2 | Descent | Progressive throughout; measured by station |
| 3 | Flexion | Suboccipito-bregmatic (9.5 cm) presents |
| 4 | Internal rotation | Occiput rotates to OA under symphysis |
| 5 | Extension | Head delivered around pubic symphysis |
| 6 | Restitution | Head realigns with fetal body |
| 7 | Expulsion | Anterior then posterior shoulder delivered |
Stages of Labour
| Stage | Definition | Duration (Nullipara / Multipara) |
|---|---|---|
| First (latent) | Onset of labour to ~6 cm dilation | Up to 25.1 hrs / up to 13.6 hrs |
| First (active) | 6 cm to full dilation (10 cm) | Up to 17.5 hrs / up to 13.8 hrs |
| Second | Full dilation to delivery of baby | Up to 146 mins / up to 64 mins |
| Third | Delivery of baby to delivery of placenta | Up to 30 mins (both) |
From Pfenninger & Fowler's Procedures for Primary Care
Key Fetal Head Diameters
| Diameter | Measurement | Position |
|---|---|---|
| Suboccipito-bregmatic | 9.5 cm | Complete flexion - ideal |
| Suboccipito-frontal | 10.5 cm | Partial flexion |
| Occipito-frontal | 11.5 cm | Deflexion |
| Mento-vertical | 13.5 cm | Brow presentation - cannot deliver vaginally |
| Biparietal (BPD) | 9.5 cm | Transverse diameter that engages |
Mnemonic
"Every Damn Fool In England Runs Everywhere"
Engagement → Descent → Flexion → Internal rotation → Extension → Restitution → Expulsion
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine; Creasy & Resnik's Maternal-Fetal Medicine; Pfenninger & Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.