Cerebellum anatomy, function, diseases, and test
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
cerebellum anatomy structure diagram lobes
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough response.
The Cerebellum
1. Anatomy
Gross Structure
The cerebellum is a foliated ("leafy") structure attached to the brainstem, lying dorsal to the pons and medulla, in the posterior fossa. Despite weighing only ~10% as much as the cerebral cortex, its surface area is about 75% of the cortex due to extensive folding (folia). — Ganong's Review of Medical Physiology, 26th ed.
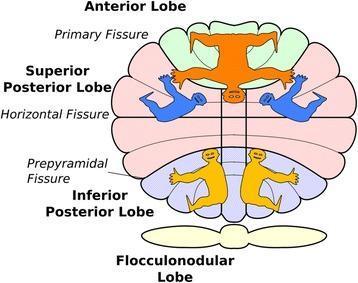
Two transverse fissures divide it into three lobes:
| Lobe | Boundaries |
|---|---|
| Anterior lobe | Anterior to the primary fissure |
| Posterior lobe | Between the primary and posterolateral fissures (largest) |
| Flocculonodular lobe | Posterior to the posterolateral fissure (phylogenetically oldest — archicerebellum) |
The vermis (midline strip) is divided into 10 lobules (I–X). The hemispheres flank it bilaterally.
Functional/Topographic Zones
| Zone | Region | Function |
|---|---|---|
| Vestibulocerebellum | Flocculonodular lobe | Balance, vestibular reflexes, eye movements |
| Spinocerebellum | Vermis + intermediate hemispheres | Gait, axial/limb coordination |
| Cerebrocerebellum | Lateral hemispheres | Planning and fine-tuning voluntary limb movements |
Midline structures control gait and axial musculature; lateral hemispheres control ipsilateral limb coordination. — Bradley & Daroff's Neurology
Cerebellar Peduncles
Three paired connections to the brainstem:
- Superior cerebellar peduncle (brachium conjunctivum) — mainly efferent: deep nuclei → red nucleus → thalamus → cerebral cortex (crosses at the inferior colliculus)
- Middle cerebellar peduncle — afferent only: contralateral pontine nuclei → cerebellum
- Inferior cerebellar peduncle — mixed: afferents from brainstem and spinal cord; efferents to vestibular nuclei
Cortical Layers (3 layers, 5 cell types)
| Layer | Key Cells |
|---|---|
| Molecular (outer) | Basket cells, stellate cells |
| Purkinje cell layer (middle) | Purkinje cells — the only output of cerebellar cortex (inhibitory to deep nuclei) |
| Granular (inner) | Granule cells, Golgi cells |
Input fibers:
- Mossy fibers → granule cells → parallel fibers → Purkinje cell dendrites (excitatory)
- Climbing fibers (from inferior olivary nucleus) → directly onto Purkinje cells (powerful excitatory drive)
Deep Cerebellar Nuclei (medial → lateral)
- Fastigial — receives vermis input; controls axial movement & balance
- Globose + Emboliform (= Interpositus) — intermediate zone input; limb coordination
- Dentate — lateral hemisphere input; voluntary movement planning
The cerebellar cortex → deep nuclei circuit is inhibitory; deep nuclei output is excitatory to thalamus and brainstem. — Adams & Victor's Principles of Neurology, 12th ed.
2. Function
The cerebellum does not initiate movement but acts as a comparator and error-corrector:
"The cerebellum monitors and modulates motor activities, responding to motor commands and inputs from sensory receptors of the joints, muscles, and vestibular system." — Bradley & Daroff's Neurology
Key functions:
- Coordination of movement (smooth, accurate trajectories)
- Planning and execution of movement
- Maintenance of posture and equilibrium
- Coordination of head and eye movements
- Motor learning — updates internal models by comparing intended vs. actual movement; dysfunction causes ataxia and improper motor predictions
- Non-motor/cognitive functions — connections to frontal, parietal, and temporal cortices underlie language, attention, and emotion; dysfunction here causes Cerebellar Cognitive Affective Syndrome (CCAS / Schmahmann syndrome)
The pathway is double-crossed: cerebellar nuclei → crossed thalamic projection → motor cortex → crossed corticospinal tract → spinal cord. Net result: a cerebellar lesion causes ipsilateral deficits. — Adams & Victor's
3. Diseases
Clinical Signs of Cerebellar Dysfunction (DANISH mnemonic)
| Sign | Description |
|---|---|
| Dysdiadochokinesia | Impaired rapid alternating movements |
| Ataxia | Wide-based unsteady gait |
| Nystagmus | End-gaze or bidirectional nystagmus |
| Intention tremor | Tremor that worsens on target approach (differs from resting tremor) |
| Scanning dysarthria | Slurred, monotone, staccato speech |
| Hypotonia | Decreased muscle tone |
Plus: dysmetria (overshoot/undershoot), decomposition of movement, rebound phenomenon, and titubation (nodding truncal tremor in midline lesions).
Disease Classification by Onset
| Acute (hours–days) | Subacute (weeks–months) | Chronic (months–years) |
|---|---|---|
| Stroke (infarct/hemorrhage) | Paraneoplastic (anti-Yo, anti-Tr, anti-VGCC) | Inherited ataxias (SCAs, Friedreich's) |
| Drug toxicity (alcohol, phenytoin, lithium, barbiturates) | Alcoholic/nutritional (B1, B12, B6, E deficiency) | Multiple sclerosis |
| Viral cerebellitis (varicella, EBV) | Anti-GAD65 autoimmune ataxia | Hypothyroidism |
| Posterior fossa subdural hematoma | Gluten ataxia (anti-gliadin) | Chiari malformation |
| — | Lyme disease | Dandy-Walker syndrome |
Source: Harrison's Principles of Internal Medicine, 22nd ed. (Table 450-1)
Key Specific Diseases
Friedreich Ataxia (autosomal recessive, GAA repeat in FXN gene)
- Onset < 25 years; progressive gait ataxia, limb ataxia, dysarthria
- Associated: areflexia, posterior column sensory loss, pes cavus, scoliosis, cardiomyopathy
- Square-wave jerks on eye exam
Spinocerebellar Ataxias (SCAs) — autosomal dominant
-
40 subtypes; SCA1, SCA2, SCA3 (Machado-Joseph), SCA6 are commonest
- SCA2: slow saccades; SCA3: saccadic pursuit, parkinsonism
- Caused by CAG repeat expansions (polyglutamine diseases) or other mechanisms
Multiple System Atrophy (MSA-C) — sporadic; cerebellar + autonomic + parkinsonian features
Paraneoplastic Cerebellar Degeneration — anti-Yo (ovarian/breast), anti-Tr (Hodgkin), anti-VGCC (SCLC); often the presenting manifestation of occult cancer
Posterior Fossa Stroke — focal, ipsilateral cerebellar signs; can cause life-threatening herniation
4. Neurological Tests for Cerebellar Function
Bedside Examination
| Test | Technique | What It Detects |
|---|---|---|
| Finger-to-nose (FNT) | Patient touches their nose then the examiner's outstretched finger (moved each time) | Dysmetria, intention tremor |
| Heel-knee-shin (HKS) | Supine patient slides heel from knee down shin of opposite leg | Lower limb cerebellar coordination |
| Rapid alternating movements (RAM) | Fist-open-fist or index finger tapping on distal thumb as fast as possible | Dysdiadochokinesia |
| Romberg test | Eyes open vs. closed standing — cerebellar ataxia present with eyes open (unlike sensory ataxia which worsens only on eye closure) | Distinguishes cerebellar from sensory ataxia |
| Tandem gait | Walking heel-to-toe | Midline (vermis) ataxia |
| Gait observation | Wide-based, irregular stride, veering | Gait ataxia |
| Rebound test | Sudden release of isometric resistance | Hypotonia, poor check reflex |
| Eye movement exam | Assess fixation, smooth pursuit, saccades | Nystagmus, dysmetric saccades, square-wave jerks |
"Asymmetry of cerebellar testing signs points toward a focal cerebellar lesion on the ipsilateral side." — Rosen's Emergency Medicine
Laboratory and Imaging Workup
Blood tests:
- Vitamins B1, B12, E (deficiency-related ataxia)
- Thyroid function (hypothyroidism)
- Paraneoplastic antibody panel (anti-Yo, anti-Tr, anti-Ri, anti-VGCC, anti-GAD65)
- Antigliadin / anti-transglutaminase antibodies
- Genetic panel for hereditary ataxias
CSF: Useful for inflammatory/paraneoplastic workup
MRI brain (modality of choice):
- Cerebellar atrophy (chronic/hereditary)
- Infarct or hemorrhage (DWI/FLAIR)
- Mass lesion, abscess, or demyelinating plaques
Genetic testing:
- CAG/GAA repeat expansion analysis (SCA1/2/3/6, Friedreich's)
- Whole exome/genome sequencing (WES/WGS) for undiagnosed cases
Diagnostic Workflow for Ataxia
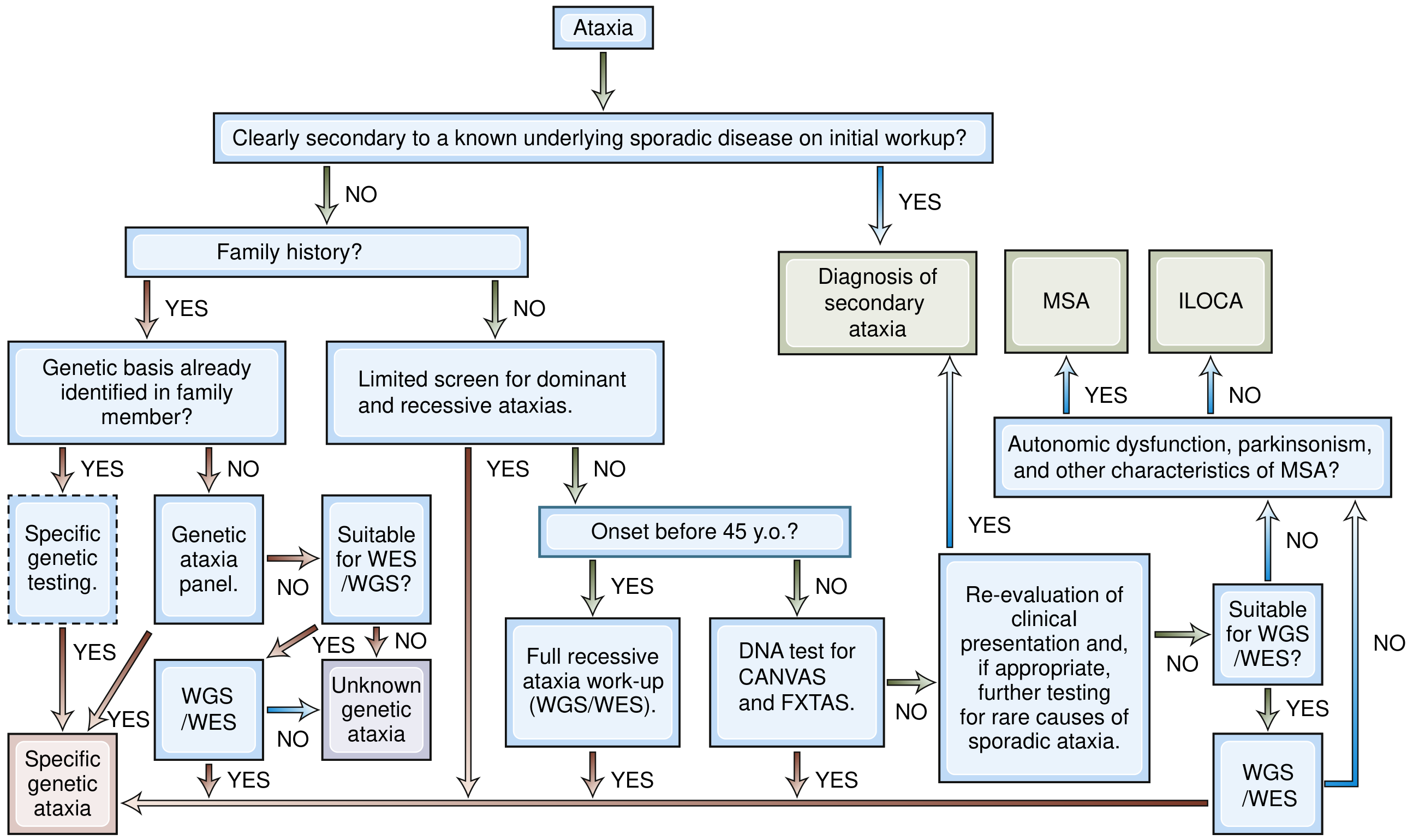
Diagnostic approach: distinguish secondary (known cause) from primary/genetic ataxia. For genetic cases, determine whether family history is present and whether onset was before or after age 45. — Bradley & Daroff's Neurology in Clinical Practice
Key clinical pearl: Cerebellar lesions cause ipsilateral incoordination (unlike UMN lesions which cause contralateral deficits). Midline/vermis lesions → predominantly gait and truncal ataxia. Hemispheric lesions → limb dysmetria and intention tremor ipsilateral to the lesion.
Sources: Costanzo Physiology 7th ed.; Ganong's Review of Medical Physiology 26th ed.; Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology 12th ed.; Harrison's Principles of Internal Medicine 22nd ed.; Neuroanatomy through Clinical Cases 3rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.