multiple joint pain with swellings in some joints on 37yr old male with thyroid nodule which is asymptomatic
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
polyarthritis thyroid nodule differential diagnosis
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Searching PubMed
polyarthritis young male differential diagnosis workup
Searching the Web
polyarthritis joint swelling thyroid nodule 37 year old male differential diagnosis
I now have comprehensive information to provide a thorough clinical analysis. Let me synthesize everything.
Clinical Analysis: Polyarthritis with Joint Swelling + Asymptomatic Thyroid Nodule in a 37-Year-Old Male
This is a clinically significant presentation that requires a structured approach. The co-occurrence of multiple joint involvement with swelling and a thyroid nodule in a young male broadens the differential considerably.
Step 1: Characterize the Arthritis
The algorithm below should guide your initial assessment:
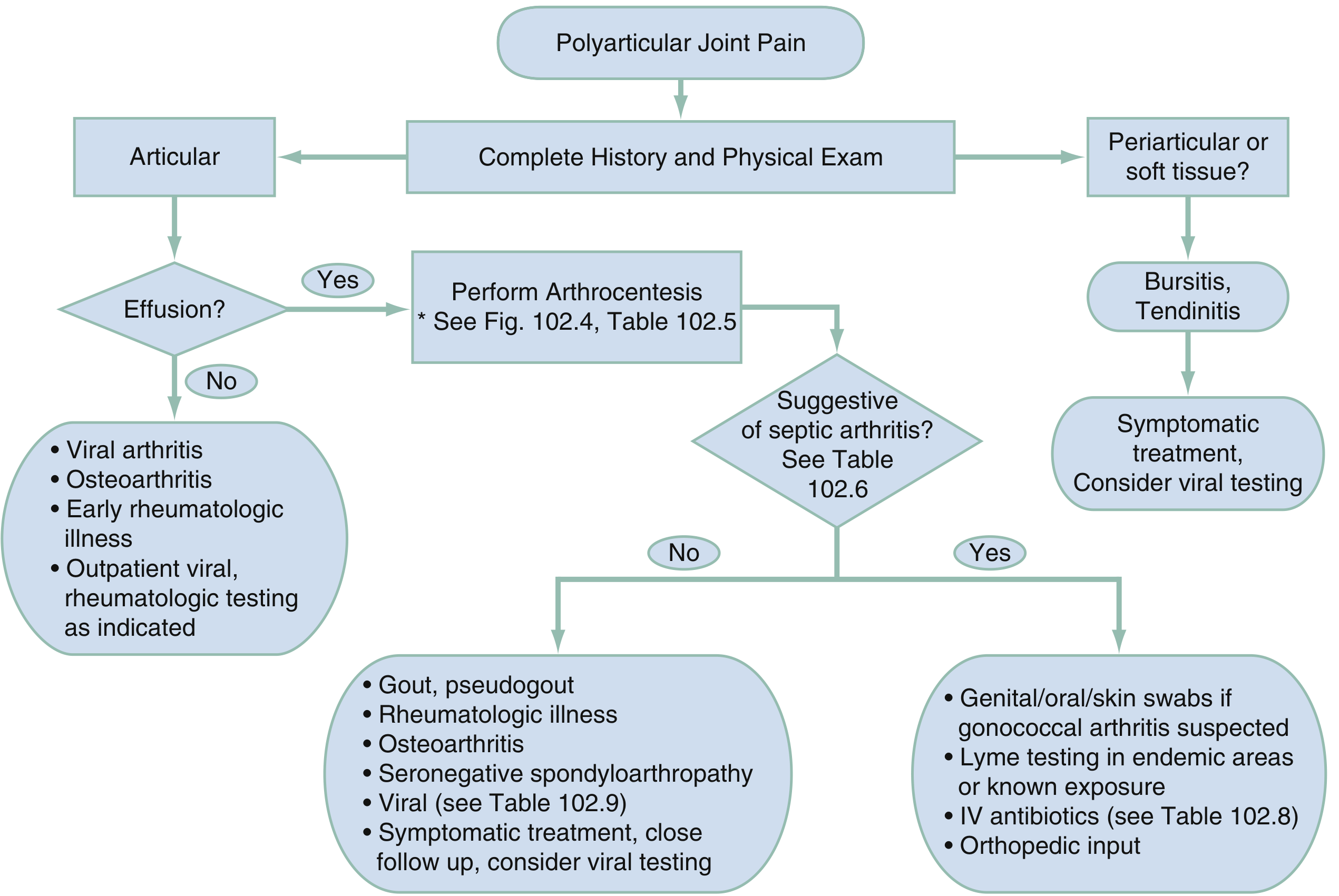
Key questions to answer first:
- How many joints? (≥5 = polyarthritis; 2-4 = oligoarthritis)
- Symmetric or asymmetric?
- Which joints? (small vs. large; axial vs. peripheral)
- Effusion present? → arthrocentesis if yes
- Duration? Acute (<6 weeks) vs. chronic
Step 2: Differential Diagnosis
🔴 High Priority — Must Exclude
| Condition | Key Features in This Patient |
|---|---|
| Rheumatoid Arthritis (RA) | Most likely. Incidence peaks 35–50 yrs; ~3× more common in women but occurs in men. Symmetric polyarthritis of PIPs, MCPs; morning stiffness; RF/anti-CCP positive in >80%. Can co-occur with autoimmune thyroid disease. |
| Seronegative Spondyloarthropathy | Male predominance (AS: M:F = 3:1; ReA: 10:1). Asymmetric, often lower limb, HLA-B27 associated. Ask about back pain, uveitis, psoriasis, GI/GU infections preceding joint pain. |
| Psoriatic Arthritis | Asymmetric oligo- or polyarthritis; look for skin/nail changes (may be subtle). |
| Reactive Arthritis | Post-GU or GI infection (Chlamydia, Salmonella, Shigella). Classic triad: arthritis + urethritis + conjunctivitis. |
| Adult-Onset Still's Disease (AOSD) | Quotidian fever, salmon-pink rash, arthritis, elevated ferritin. Consider in young males. |
🟡 Important to Consider
| Condition | Notes |
|---|---|
| Viral Arthritis | Parvovirus B19 (symmetric RA-like in adults), Hep B/C (symmetric or intermittent), Chikungunya/Ross River, HIV |
| Septic Arthritis / Gonococcal | Sexually active young male → GC dissemination (<3% of mucosal infections). Migratory arthritis, tenosynovitis, dermatitis. Urgent if suspected. |
| Gout / Pseudogout | Less typical at 37 without metabolic risk, but possible. Crystal analysis from synovial fluid. |
| Lyme Arthritis | Endemic area exposure; typically mono/oligoarthritis of large joints. |
🟢 Endocrine Link — The Thyroid Nodule Connection
This is where the case becomes interesting. The thyroid nodule + polyarthritis in the same patient could be:
1. Hypothyroid Arthropathy (most important endocrine cause)
"Musculoskeletal symptoms occur in 33% of patients with clinical hypothyroidism (TSH >20 μU/mL). Patients can present with carpal tunnel syndrome, Raynaud phenomenon, or muscle aching... myxedematous patients can develop a symmetrical arthropathy of the large joints, especially the knees, associated with noninflammatory synovial fluid with increased viscosity." — Goldman-Cecil Medicine, Chapter 254
- The thyroid nodule may represent Hashimoto's thyroiditis causing hypothyroidism
- Check TSH urgently — this is a treatable cause of arthropathy
2. Autoimmune Thyroid Disease + Systemic Autoimmune Disease
"Patients with autoimmune thyroid disease have an increased prevalence of nonspecific arthralgias, positive antinuclear antibodies, and possibly an increased association with systemic autoimmune rheumatic diseases such as Sjögren syndrome." — Goldman-Cecil Medicine
- Hashimoto's thyroiditis is associated with RA, SLE, and Sjögren syndrome
3. Hyperthyroidism / Graves' Disease
- Thyroid acropachy (rare, <1%): soft tissue swelling of hands, digital clubbing, periostitis
- Proximal myopathy (70%) and adhesive capsulitis (10%) more common
4. Malignancy (Paraneoplastic) — Rule Out
"Polyarthritis can rarely (<2%) be the presenting manifestation of an occult malignancy... Clinical features suggesting carcinomatous polyarthritis include explosive onset of RF-negative, asymmetrical polyarthritis... in a patient older than 50." — Goldman-Cecil Medicine
- Less likely at 37, but a new thyroid nodule must be evaluated for malignancy (thyroid cancer can rarely present with paraneoplastic arthritis)
Step 3: Investigations
Immediate Workup
| Test | Rationale |
|---|---|
| TSH, Free T4 | Rule out hypothyroid/hyperthyroid arthropathy |
| Anti-TPO, Anti-thyroglobulin Ab | Hashimoto's thyroiditis (autoimmune link) |
| RF, Anti-CCP | RA (most common chronic polyarthritis) |
| ANA, anti-dsDNA, anti-Sm | SLE screening |
| ESR, CRP | Inflammatory vs. non-inflammatory |
| CBC, LFTs, uric acid, BMP | Baseline; gout; hematologic malignancy |
| HLA-B27 | Spondyloarthropathy |
| Synovial fluid analysis | Mandatory if effusion present — cell count, crystals, culture |
Thyroid Nodule Workup (Standard)
| Test | Rationale |
|---|---|
| Thyroid ultrasound | Characterize nodule (size, echogenicity, vascularity, calcifications — TIRADS) |
| TSH | If suppressed → hot nodule → thyroid scan |
| FNAC (FNA cytology) | For nodules ≥1 cm with suspicious features |
If Viral Arthritis Suspected
- Parvovirus B19 IgM/IgG, Hep B sAg/sAb, Hep C Ab, HIV
- Chikungunya/dengue serology (if travel history)
Step 4: Diagnostic Framework
Young Male + Polyarthritis + Joint Swelling + Thyroid Nodule
│
├── Inflammatory? (ESR/CRP elevated, morning stiffness, warm joints)
│ ├── Symmetric small joints → RA, viral (Parvo B19)
│ ├── Asymmetric lower limbs + axial → Spondyloarthropathy
│ ├── Fever + rash + high ferritin → Adult Still's disease
│ └── Post-infection → Reactive arthritis
│
├── TSH abnormal?
│ ├── High TSH → Hashimoto's hypothyroid arthropathy
│ └── Low TSH → Graves'/hyperthyroid, evaluate for Graves' acropachy
│
├── Autoimmune panel positive? → SLE, Sjögren, overlap syndrome
│
└── Nodule suspicious on US (TIRADS ≥4)? → Consider paraneoplastic if RF-negative, asymmetric
Clinical Pearls for This Case
- Do not dismiss the thyroid nodule as coincidental — autoimmune thyroid disease is the most common cause of thyroid nodules and shares immune pathways with inflammatory arthritis.
- TSH is the single most important first test — hypothyroid arthropathy is under-diagnosed and fully reversible with thyroid hormone replacement.
- Male sex + polyarthritis shifts probability toward seronegative spondyloarthropathies (especially AS and reactive arthritis) compared to females.
- At age 37, RA is still within peak incidence and remains the most common cause of chronic polyarthritis with swelling.
- Synovial fluid analysis is mandatory for any joint with a visible effusion before labeling the diagnosis — it distinguishes inflammatory, crystal, and septic arthritis.
Sources:
- Goldman-Cecil Medicine, Chapter 254 (Arthritis Associated with Systemic Disease)
- Goldman-Cecil Medicine, Chapter 244 (Spondyloarthropathies — Differential Diagnosis Table)
- Rosen's Emergency Medicine, Chapter 102 (Polyarthritis Algorithm and Differential)
This is a shared conversation. Sign in to Orris to start your own chat.