Teach me tvs with real time sonographic pictures and landmarks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough visual TVS tutorial. Let me compile the complete lesson:
Transvaginal Sonography (TVS) - Complete Illustrated Guide
Sources: Color Atlas of Ultrasound Anatomy 3e, Pfenninger & Fowler's Procedures for Primary Care 3e, Berek & Novak's Gynecology
1. What is TVS and Why Use It?
TVS (also called endovaginal ultrasound) uses a high-frequency intracavitary probe inserted into the vagina to image pelvic structures at close range. Compared to transabdominal ultrasound (TAS):
| Feature | TVS | TAS |
|---|---|---|
| Frequency | 5-10 MHz (higher) | 3.5-5 MHz |
| Resolution | Superior - near-field detail | Lower |
| Bladder prep | Empty bladder preferred | Full bladder required |
| Depth | Limited (~10 cm) | Greater depth |
| Patient comfort | Mildly invasive | Non-invasive |
| Obese patients | Better results | Poor window |
TVS is the first-line modality for evaluating the uterus, endometrium, ovaries, adnexa, early pregnancy, and pelvic pain.
2. Probe Orientation and Image Conventions
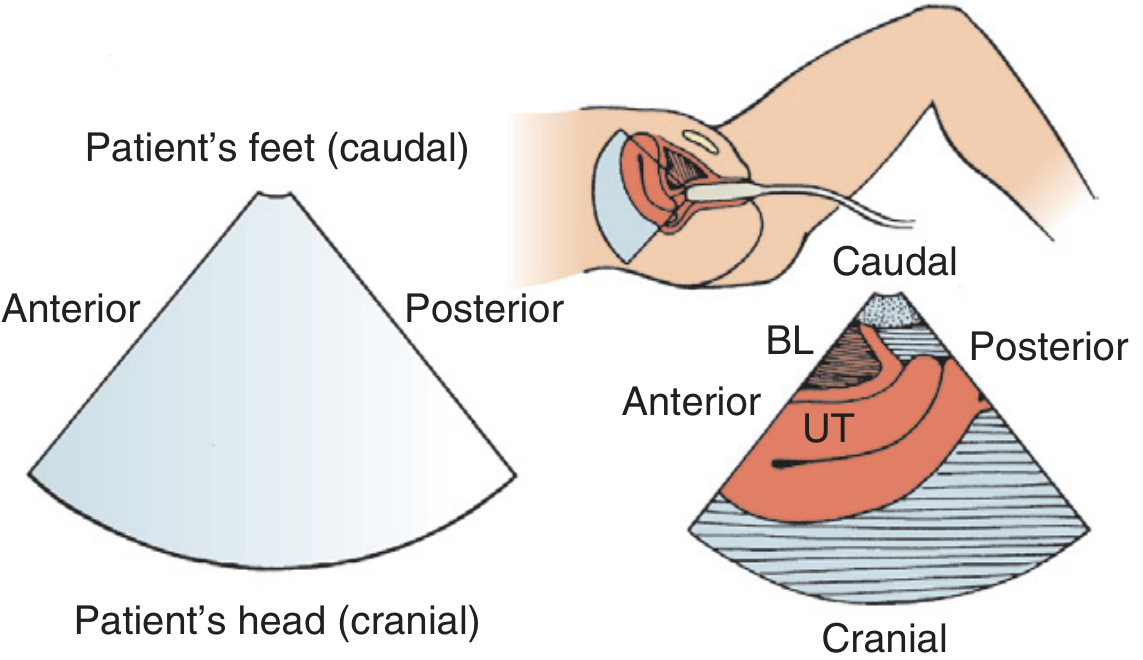
Figure 225-13 from Pfenninger & Fowler's - Longitudinal orientation with transvaginal scanning. BL = bladder, UT = uterus
Key orientation rules for TVS (different from TAS):
- With the marker dot pointing anteriorly (toward the abdominal wall), the left side of the image = anterior (not cranial as in TAS)
- In longitudinal plane: fundus is typically to the left of screen, cervix to the right
- In coronal/transverse plane: patient's right side remains on the left side of the image (marker dot toward patient's right)
- The probe sits anterior to the cervix; avoid inserting too deeply or you miss the lower uterine segment
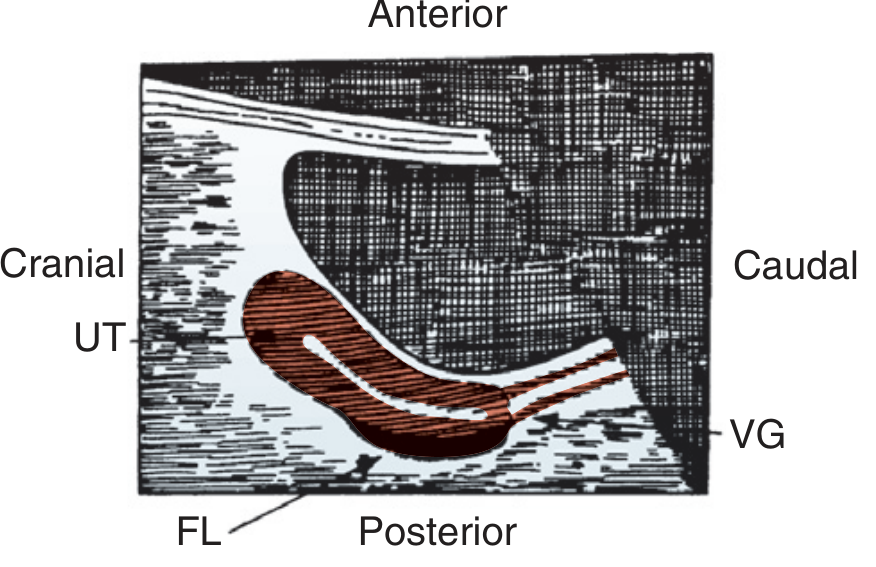
Longitudinal view: UT = uterus, FL = free fluid in posterior cul-de-sac (pouch of Douglas), VG = vaginal stripe
3. Step-by-Step TVS Technique
- Patient position: Supine or lithotomy. TVS is usually preceded by TAS to assess overall anatomy, then the bladder is emptied (some residual urine is useful as a landmark).
- Probe prep: Cover with probe sheath/condom, place adequate gel between cover and transducer, smooth out air bubbles.
- Pelvic exam first: Assess uterine size, position, tenderness. Remove tampons. Obtain verbal consent.
- Insertion: With marker dot anterior, gently insert with posterior vaginal pressure to a position anterior to the cervix.
- Scanning begins immediately on insertion - scanning starts as soon as the probe is in, avoid over-inserting.
- Systematic sweep: Obtain longitudinal, coronal, and oblique scans by rotating the probe. Oblique views are used for adnexa.
- Document: Note fluid accumulations, fetal structures (if applicable), any areas of tenderness.
4. Normal Landmarks: The Uterus
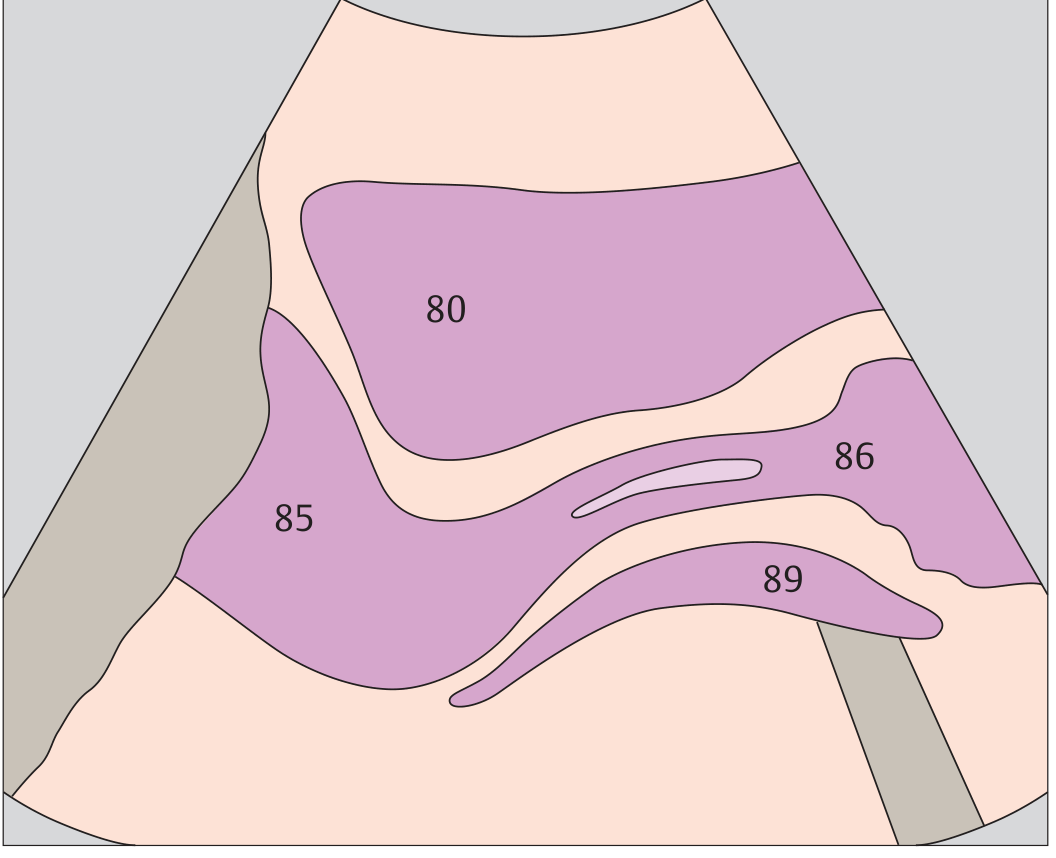
Sagittal (Longitudinal) View
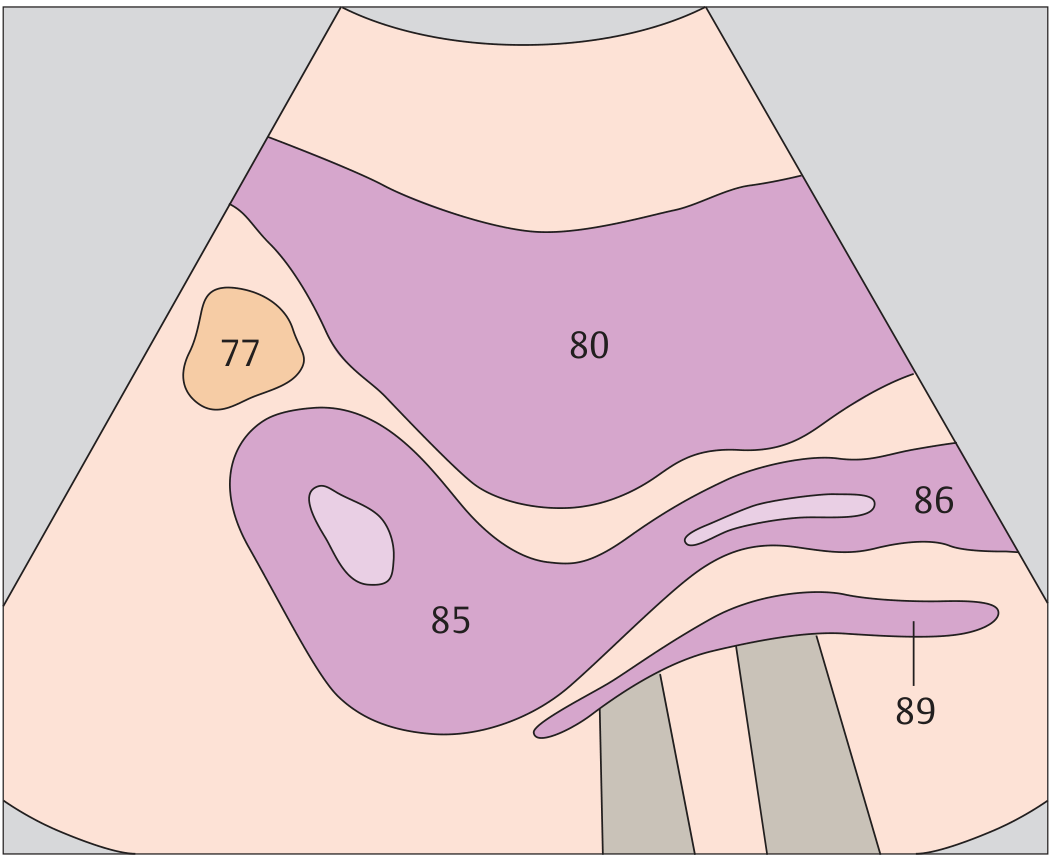
Sagittal TVS - Key: 80 = uterine body (myometrium), 85 = cervix, 86 = vagina, 77 = urinary bladder, 89 = rectum/posterior compartment
What you see on sagittal:
- The uterus = intermediate echogenicity, pear-shaped
- Endometrial stripe = hyperechoic central line; thickness varies with menstrual phase
- Myometrium = homogeneous, medium echogenicity surrounding the endometrium
- Cervix = lower, more echogenic than the fundus
- Bladder = anechoic (black) anteriorly - useful landmark even when empty on TVS
- Posterior cul-de-sac (pouch of Douglas) - look here for free fluid
Atlas note: "The uterus consists of the fundus, corpus, and cervix" - Color Atlas of Ultrasound Anatomy, p. 322
Coronal (Transverse) View
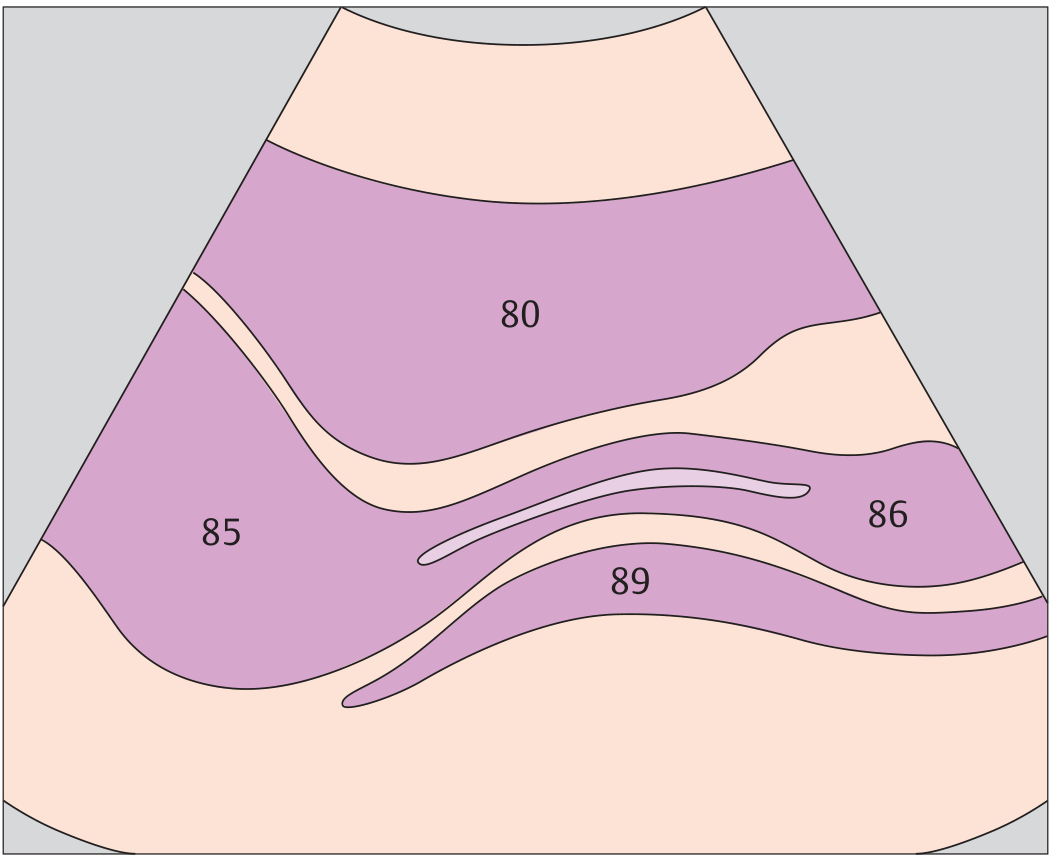
Coronal TVS - broad band of uterine myometrium (80) in the center, cervix (85) inferiorly, vaginal layers (86, 89)
5. Uterine Layers - High-Resolution TVS Detail
TVS at 7.5-10 MHz resolves the uterine wall into distinct layers:
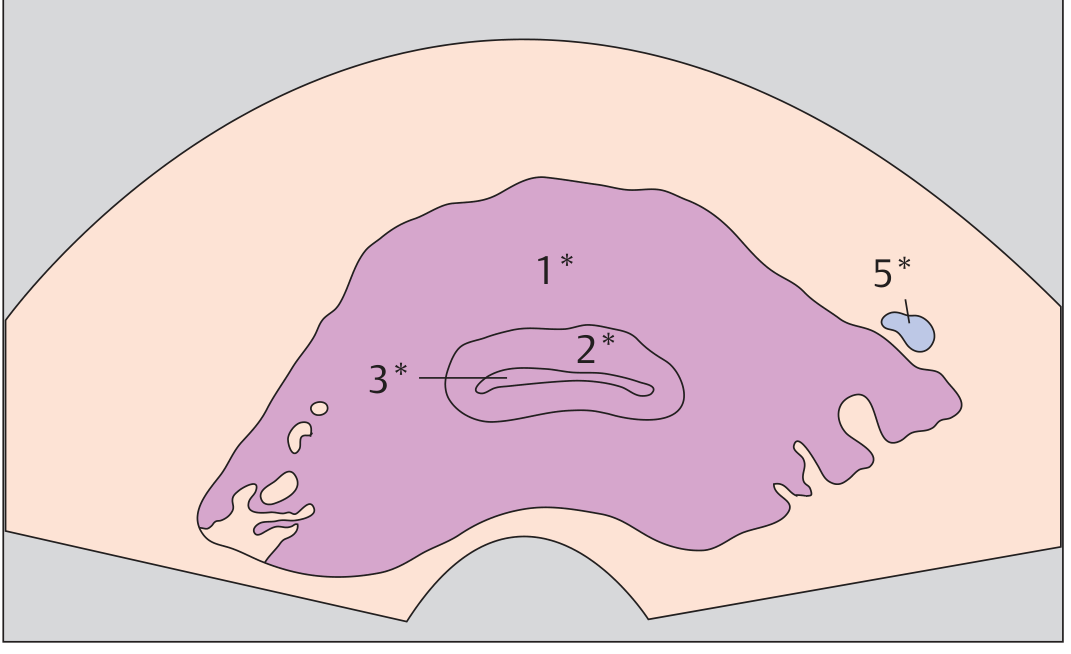
TVS cross-section of uterus: 1* = myometrium, 2* = endometrium, 3* = uterine lumen, 5* = periuterine vessels

Labeled TVS cross-section: 1* = myometrium (medium echogenicity, surrounding), 2* = endometrium (hyperechoic layer), 3* = endometrial lumen (hypoechoic line), 5* = uterine vessels
Endometrial Thickness by Cycle Phase
| Phase | Appearance | Thickness |
|---|---|---|
| Early proliferative | Thin, hypoechoic | 4-8 mm |
| Late proliferative | Triple-line pattern | 8-12 mm |
| Secretory | Thick, hyperechoic | 10-16 mm |
| Postmenopausal | Thin, echogenic stripe | ≤5 mm (normal) |
"The uterine cavity is visible sonographically only during menstruation and pregnancy" - Color Atlas of Ultrasound Anatomy, p. 323
6. Vagina Landmark
The vagina appears on TVS as an elongated, hypoechoic structure posterior to the bladder with a central band of higher-level echoes (the vaginal stripe, representing the mucosal interface).
Uterus (80) in sagittal with cervix (85), vaginal region (86), and posterior structures (89) labeled. Note the ovaries flank the superior border of the full urinary bladder.
"The vagina appears behind the bladder as an elongated, hypoechoic structure with a central band of higher-level echoes" - Color Atlas of Ultrasound Anatomy, p. 321
7. The Ovaries
The ovaries are the most important adnexal structures to identify on TVS.
How to Find the Ovaries
- After imaging the uterus in longitudinal view, rotate the probe obliquely (clockwise for left adnexa, counterclockwise for right)
- Landmark: the iliac vessels - ovaries lie medial to the internal iliac vessels
- Use the follicles as a guide - small anechoic cysts within the ovary are a giveaway
TVS Ovary with Follicle
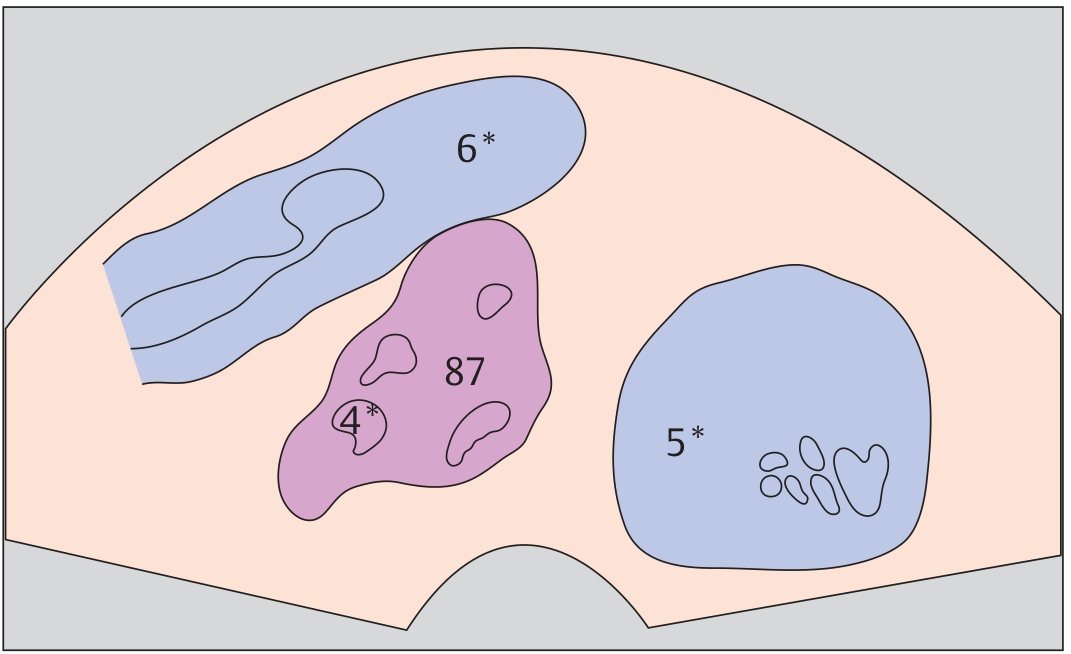
Right ovary: 87 = ovarian stroma (intermediate echogenicity), 4* = follicle (anechoic), 5* = ovarian vessels, 6* = iliac vessels. The ovary sits medial to the iliac vessels.
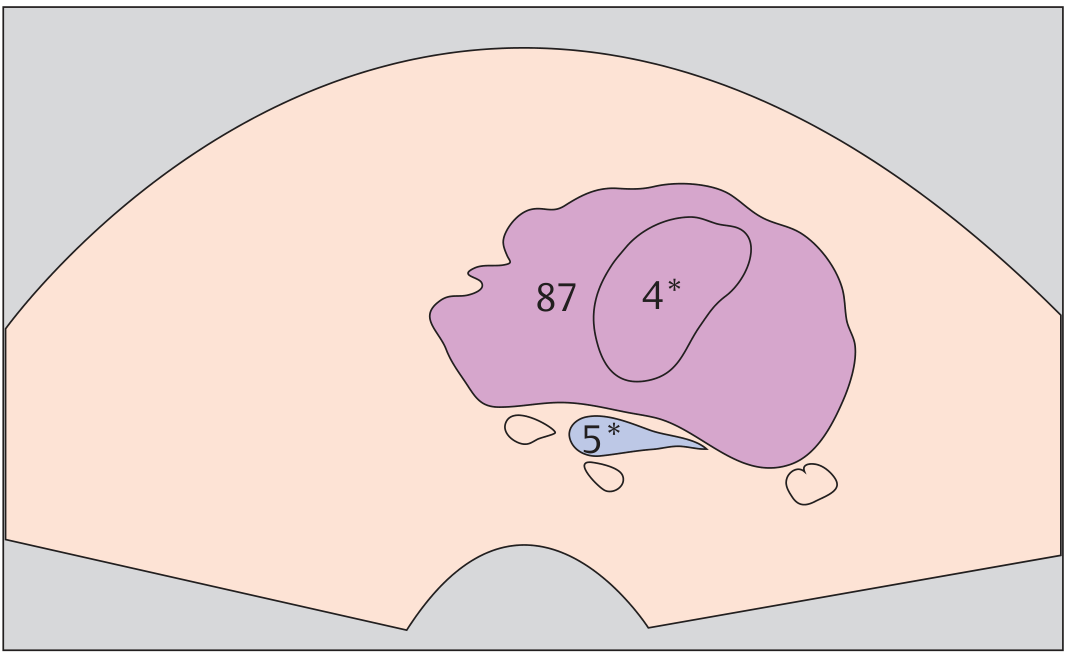
Close-up TVS of ovary: 87 = ovarian stroma, 4* = dominant follicle (anechoic cyst, pre-ovulatory can reach 18-22 mm), 5* = ovarian vessels
Normal Ovary Measurements
| Parameter | Normal |
|---|---|
| Size (adult) | 3 x 2 x 2 cm (volume ~8 mL) |
| Postmenopausal | Volume ≤3 mL |
| Follicle | Multiple small, anechoic, ≤10 mm |
| Dominant follicle | Up to 18-22 mm pre-ovulatory |
8. Uterus-Bladder-Ovary Layout (Coronal View)
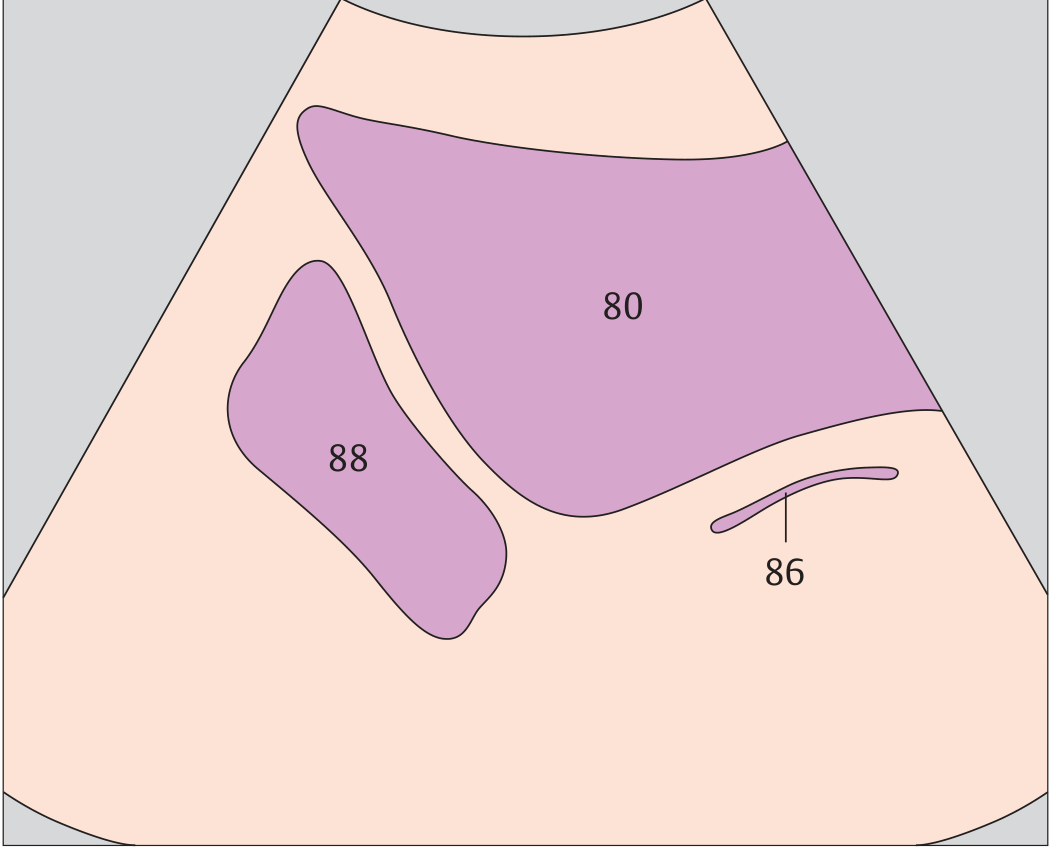
Coronal TVS: 80 = uterine body, 88 = adnexa (ovary location), 86 = cervico-vaginal region. Note the relationships - uterus centrally, ovaries flanking it laterally.
"The ovaries flank the superior border of the full urinary bladder" - Color Atlas of Ultrasound Anatomy, p. 323
9. Clinical Applications - What TVS Diagnoses
| Indication | TVS Finding |
|---|---|
| Ectopic pregnancy | Empty uterus + adnexal mass/ring; free pelvic fluid |
| Missed/threatened abortion | Absent/abnormal fetal cardiac activity |
| Endometrial polyp | Hyperechoic pedunculated lesion in cavity |
| Fibroids (leiomyoma) | Hypoechoic, well-defined intramural mass |
| Ovarian cyst | Anechoic, thin-walled adnexal structure |
| Tubo-ovarian abscess | Complex heterogeneous mass, TOC vs TOA differentiated on TVS |
| PCOS | ≥12 follicles per ovary, each 2-9 mm, or ovarian volume >10 mL |
| Adenomyosis | Heterogeneous myometrium, asymmetric thickening, myometrial cysts |
TVS has 75% PPV and 96.5% negative predictive value for intracavitary polyps compared to hysteroscopy (Berek & Novak's Gynecology, p. 2063).
10. TVS vs. TAS: When to Choose Which
Use TVS when:
- Early intrauterine pregnancy needs confirmation (<8 weeks)
- Patient cannot fill bladder (ectopic emergency)
- Obese patient (poor TAS window)
- Detailed endometrial evaluation needed
- Ovarian pathology assessment
Use TAS when:
- Larger pelvic masses (beyond TVS depth)
- Second/third trimester pregnancy
- Patient refuses TVS
- Screening (TVS as follow-up)
Key Sonographic Numbers to Remember
| Structure | Normal Measurement |
|---|---|
| Uterus (nulliparous) | 6-8 cm length, 3-5 cm AP |
| Endometrium (secretory) | Up to 16 mm bilayer |
| Endometrium (postmenopausal) | ≤5 mm (>5 mm = investigate) |
| Cervical length (non-pregnant) | ~3 cm |
| Ovary volume (reproductive) | ≤8 mL |
| Dominant follicle pre-ovulation | 18-22 mm |
| Free fluid (small amount) | Normal in cul-de-sac mid-cycle |
All sonographic diagrams: Color Atlas of Ultrasound Anatomy, 3e (Thieme). Clinical technique: Pfenninger & Fowler's Procedures for Primary Care, 3e. Clinical applications: Berek & Novak's Gynecology.
This is a shared conversation. Sign in to Orris to start your own chat.