Skin tumors in surgery final year mbbs students in exam points in hinglish with images
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Ab mere paas saara material hai. Ab main ek comprehensive Hinglish answer likhta hoon surgery final year MBBS students ke liye.
🩺 SKIN TUMORS - Surgery Final Year MBBS
Exam-Ready Points in Hinglish | Robbins + Sabiston se
📋 CLASSIFICATION (Yaad karo - EXAM FAVOURITE!)
| Category | Tumor |
|---|---|
| Benign Epithelial | Seborrheic Keratosis, Actinic Keratosis (premalignant) |
| Malignant Epithelial | Basal Cell Carcinoma (BCC), Squamous Cell Carcinoma (SCC) |
| Melanocytic Benign | Melanocytic Nevus, Dysplastic Nevus |
| Melanocytic Malignant | Melanoma |
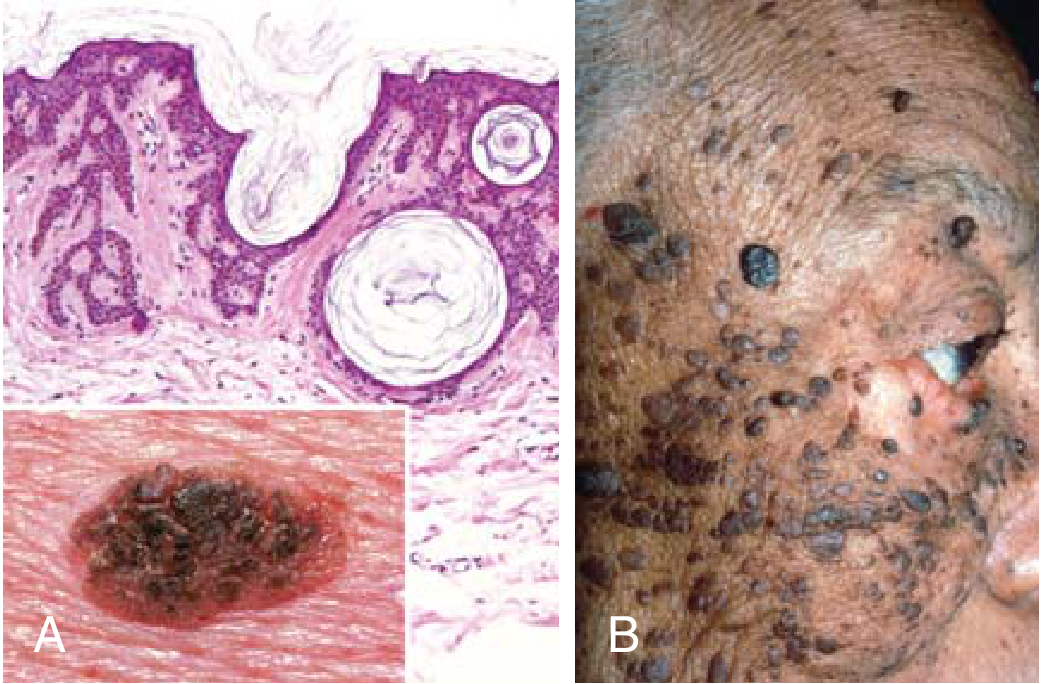
1. SEBORRHEIC KERATOSIS
Yaad karo: "Waxy, stuck-on lesion of old people"
- Kya hota hai: Middle-age/elderly mein common, pigmented epidermal tumor
- Site: Trunk sabse zyada, phir face, neck, extremities
- Mutation: FGFR3 activating mutation (RAS/PI3K pathway)
- Appearance: Tan to dark brown, "stuck-on" / waxy, granular surface, coin-like plaques
- Micro: Basaloid cells + horn cysts + pseudo-horn cysts (PATHOGNOMONIC)
⚠️ EXAM TRAP - Sign of Leser-Trelat:
Sudden eruptive seborrheic keratoses (bahut saare ek saath) = Paraneoplastic syndrome - GI tract carcinoma socho!
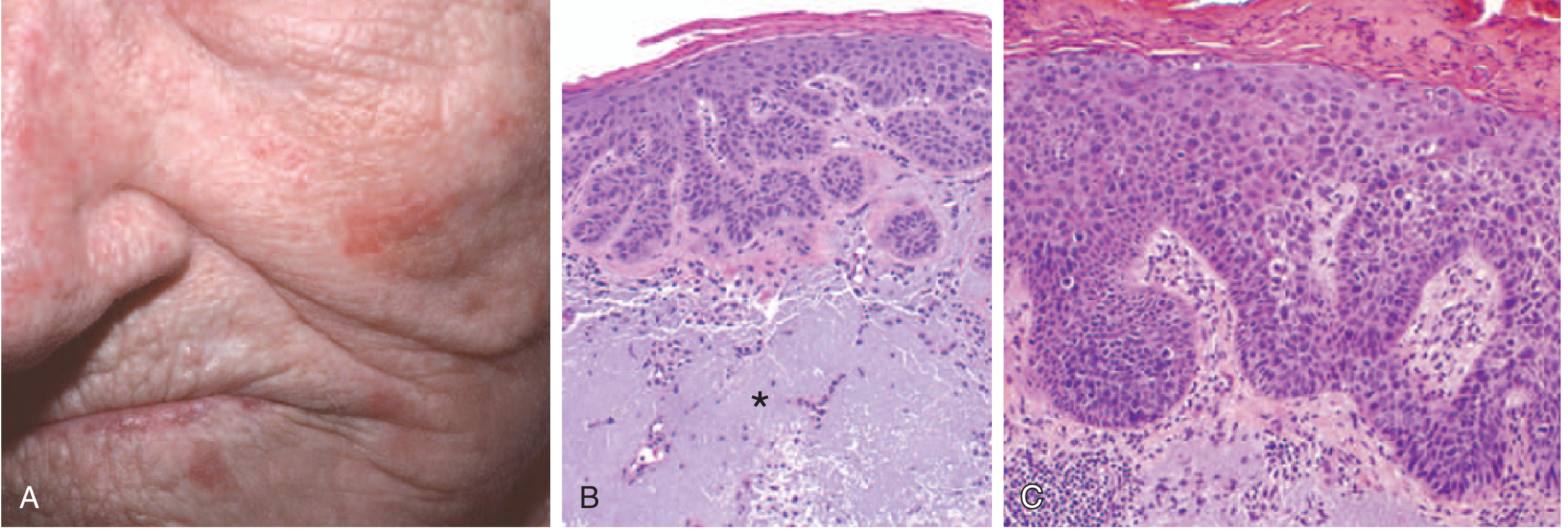
2. ACTINIC KERATOSIS (Premalignant!)
Yaad karo: "UV-damaged sandpaper lesion"
- Cause: UV-induced TP53 mutation (same mutations as SCC - isliye PREMALIGNANT)
- Site: Sun-exposed areas - face, arms, dorsum of hands, cheek/nose
- Appearance: <1 cm, tan-brown or red, rough "sandpaper" texture
- Progression to SCC: 0.1% to 2.6% per year (low, but treat karo)
- Micro: Basal cell atypia + hyperkeratosis + parakeratosis + solar elastosis (dermis mein blue-gray elastic fibers)
Treatment:
- Cryotherapy (superficial freezing) - simple and effective
- Topical agents (5-Fluorouracil, imiquimod)
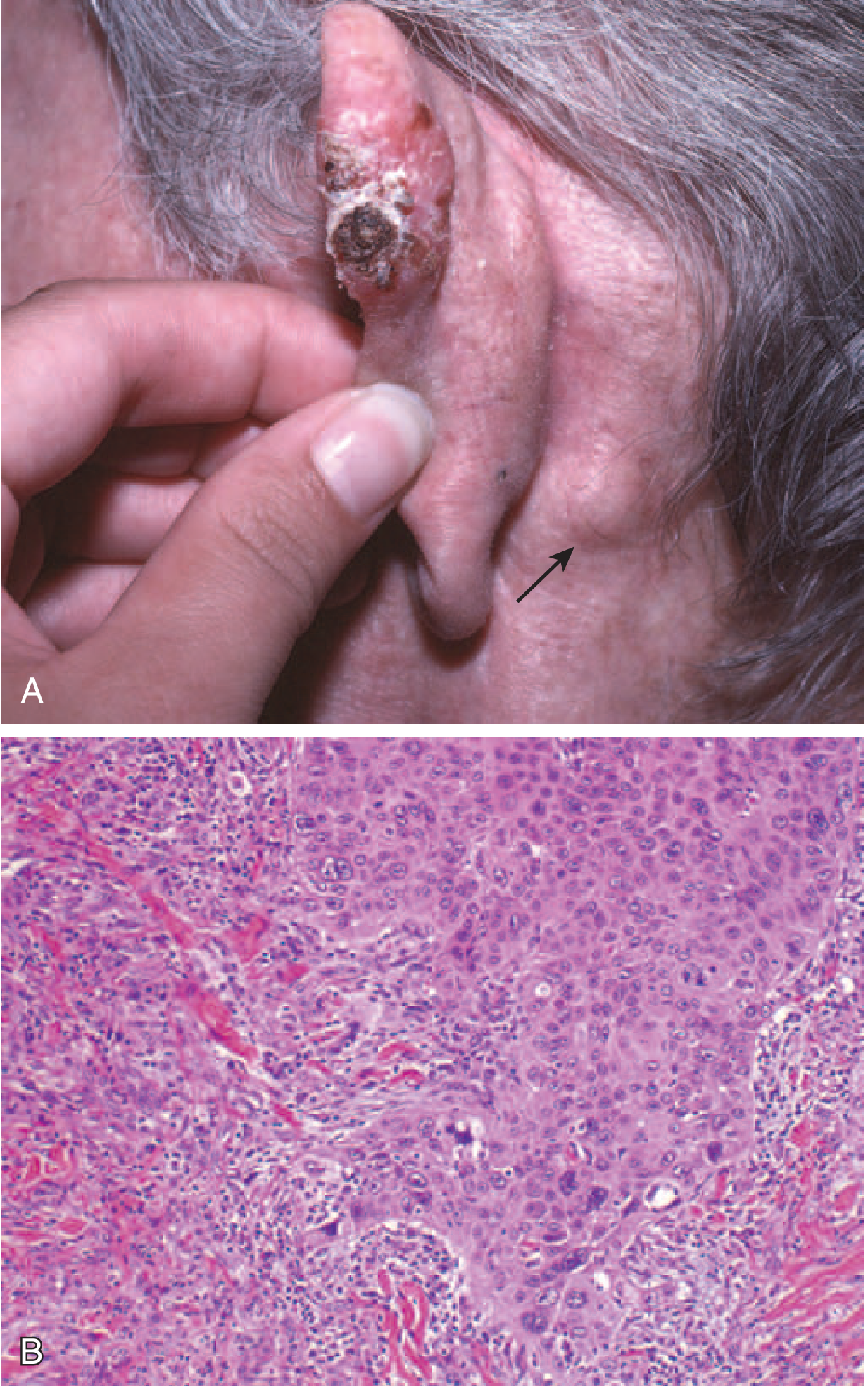
3. SQUAMOUS CELL CARCINOMA (SCC)
Yaad karo: "Nodular ulcerating lesion on sun-exposed skin"
Pathogenesis (Mutation list - exam mein aata hai!):
- UV light → TP53 mutation (most common)
- RAS activating mutation
- NOTCH receptor loss of function
- Immunosuppression (organ transplant patients - HIGH risk!)
Risk Factors:
- Sun exposure (UV), xeroderma pigmentosum
- Oncogenic HPV (genital skin)
- Industrial carcinogens (tars, oils)
- Chronic non-healing ulcers, burn scars → Marjolin's ulcer (aggressive SCC!)
- Arsenical keratoses, ionizing radiation
Clinical Features:
- Nodular, scaly, often ulcerated lesion
- Men > Women, fair skin, older adults
- ~4% mein regional lymph node metastasis at diagnosis
Bowen's Disease = SCC in situ
- Plaque-like lesion with crusting
- Full-thickness epidermal atypia
Treatment:
- <2.5 cm: Wide excision with 6mm clear margin
- Large/invasive: Radical excision, consider Mohs surgery
- Metastatic: Highly responsive to immune checkpoint inhibitors (high mutational burden ke wajah se)
Marjolin's Ulcer (EXAM FAVOURITE!):
SCC arising in chronic scar/burn wound / cicatricial tissue. Poorer prognosis, more aggressive behavior.
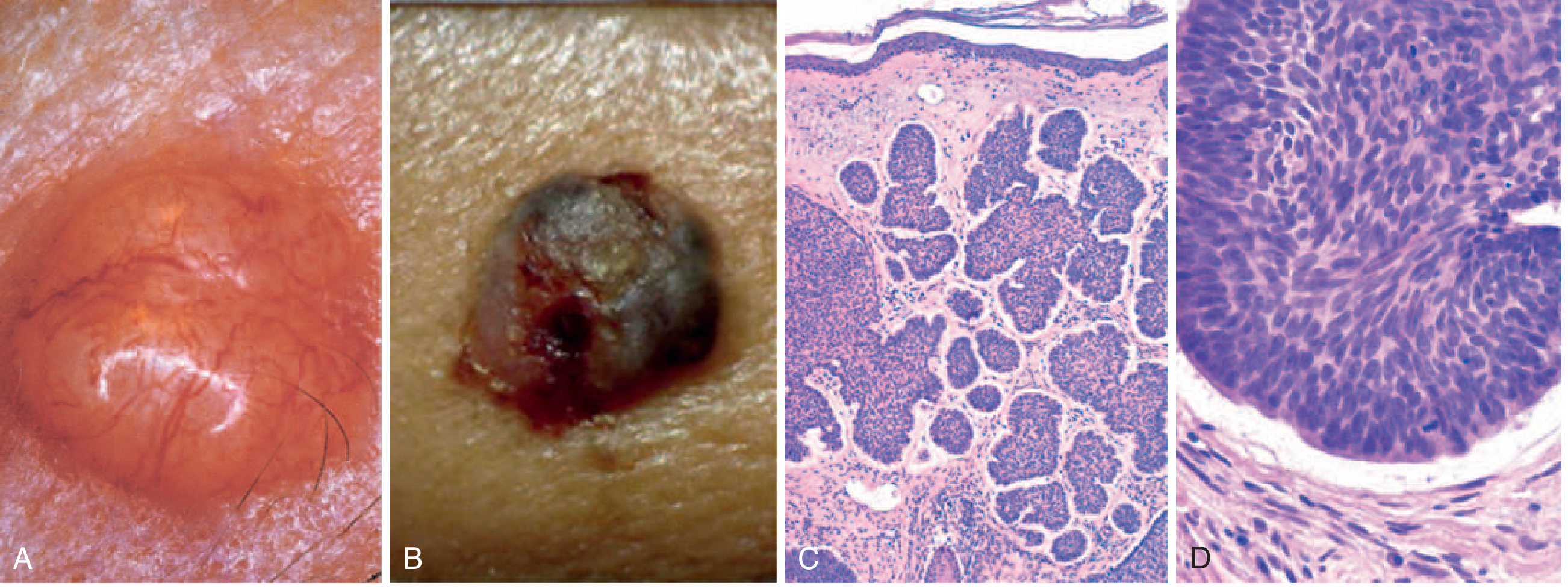
4. BASAL CELL CARCINOMA (BCC)
Yaad karo: "Most common skin cancer, slow-growing, rarely metastasizes, pearly nodule with telangiectasia"
Pathogenesis:
- PTCH1 mutation (loss of function) → Hedgehog pathway constitutively active
- Gorlin Syndrome (Nevoid BCC syndrome): Autosomal dominant, germline PTCH1 mutation → Familial BCC + odontogenic keratocysts + medulloblastoma
- TP53 mutation also common (UV-induced)
Clinical Features:
- Raised nodule/papule with rolled edges ± ulceration
- Telangiectasia (dilated subepidermal vessels) - PATHOGNOMONIC
- Light skin: erythematous; Dark skin: pigmented (melanoma jaisi dikh sakti hai)
- Most common skin cancer (>1 million cases/year US mein)
Morphology (Micro):
- Basaloid cells, peripheral palisading of nuclei
- Cleft between tumor nests and stroma (artifact of sectioning) - CHARACTERISTIC
- Fibrotic or mucinous stromal matrix
- Never on mucosal surfaces (only epidermis/follicular epithelium se arise)
Treatment:
- Local excision curative
- 40% patients mein 5 years ke andar doosra BCC develop hota hai
- Advanced: PTCH1/Hedgehog inhibitor (vismodegib)
5. MELANOCYTIC NEVI (Moles)
Yaad karo: "Benign, <5mm, uniform pigmentation, well-defined borders"
- Mutation: BRAF or RAS gain-of-function → proliferation then senescence (isliye benign rahta hai)
- Types:
- Junctional nevus: Cells at dermoepidermal junction only
- Compound nevus: Junction + dermis dono mein
- Intradermal nevus: Only dermis (most elevated)
- Micro: Superficial cells - large, pigmented, nests; Deep cells - small, no pigment, cords → "Maturation" hoti hai depth ke saath (BENIGN ka sign)
6. DYSPLASTIC NEVI
- Sporadic ya familial
- Familial → increased melanoma risk
- Size >5 mm, variable pigmentation, irregular borders, "pebbly" surface
- Bridging of nests, lentiginous hyperplasia at junction
- Cytologic atypia + linear fibrosis in dermis
- CDKN2A (p16) mutations common
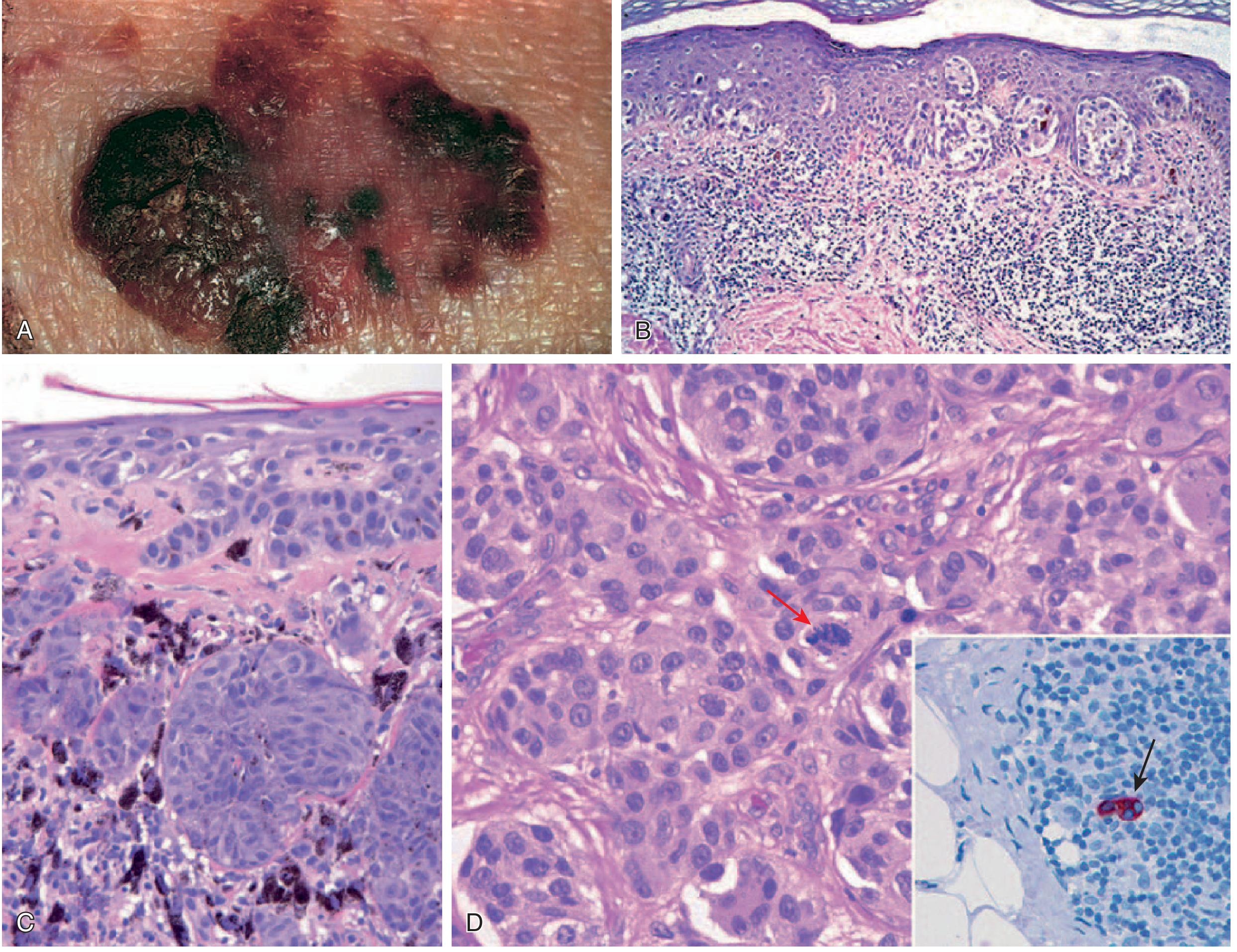
7. MELANOMA ⭐ (MOST IMPORTANT FOR EXAM!)
Yaad karo: "ABCDE rule, Breslow thickness, BRAF mutation"
Pathogenesis - Step-by-Step Mutations:
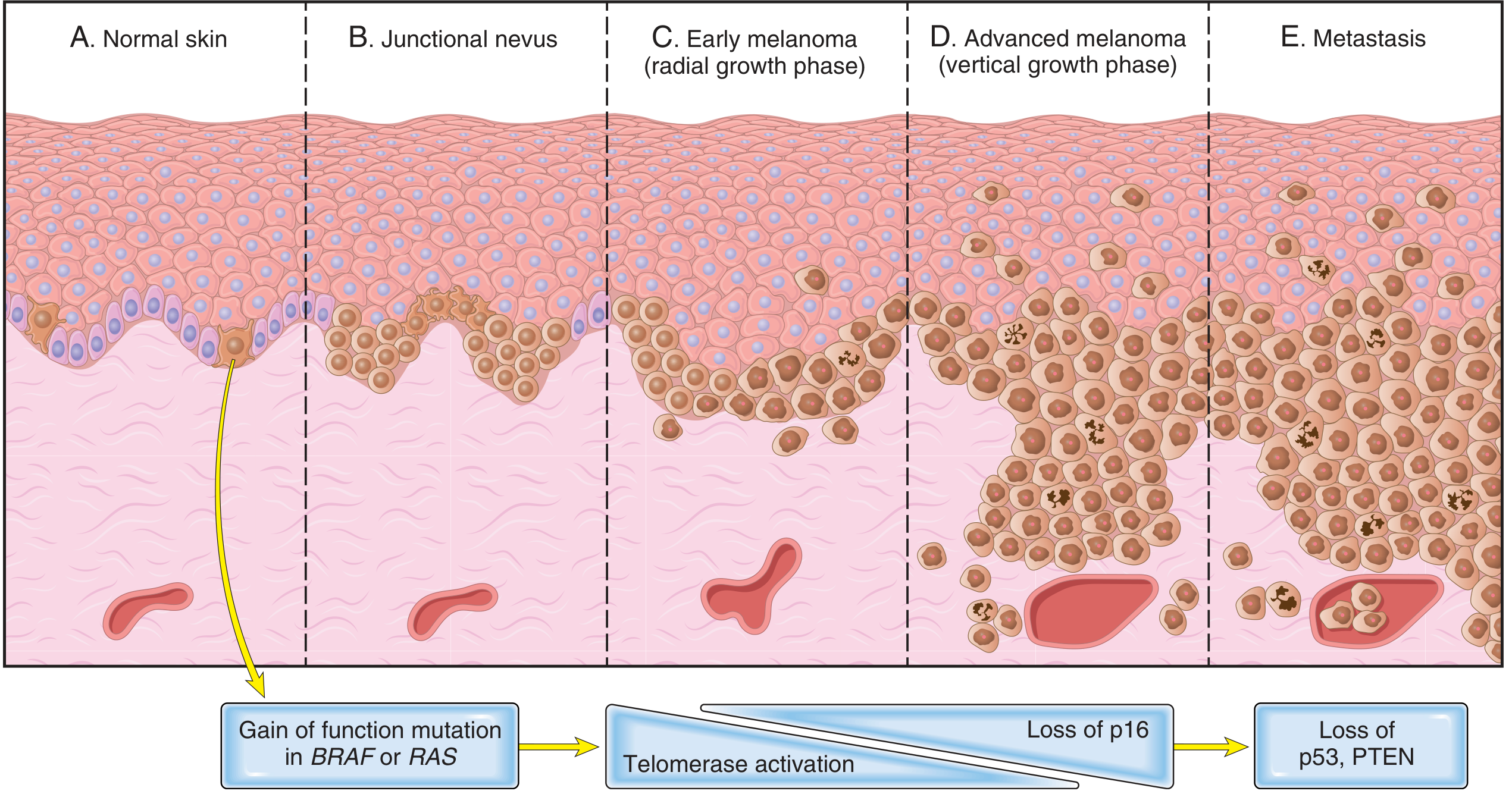
| Step | Event |
|---|---|
| 1 | BRAF/RAS gain-of-function → nevus |
| 2 | Telomerase activation → breaks senescence |
| 3 | Loss of p16 (CDKN2A) → vertical growth phase |
| 4 | Loss of TP53 + PTEN → metastasis |
Growth Phases (EXAM FAVOURITE!):
- Radial growth phase: Lateral spread in epidermis, NO metastasis capacity yet, flat lesion
- Vertical growth phase: Downward dermal invasion, nodule form karta hai, metastasis potential aata hai
ABCDE Rules (Warning Signs):
| Letter | Means |
|---|---|
| A | Asymmetry |
| B | Border irregularity |
| C | Color variegation (black, brown, red, blue, gray) |
| D | Diameter >6mm |
| E | Evolution (change in existing nevus) |
Histology:
- Pagetoid spread (cells at all levels of epidermis)
- Large nuclei, hyperchromatic, chromatin peripherally clumped
- "Cherry red" prominent nucleoli (PATHOGNOMONIC!)
- Atypical mitotic figures
Prognosis - Breslow Thickness:
Breslow thickness = depth of invasion in mm from granular layer to deepest tumor cell
- Thin lesion = curable surgically
- Thick + high mitotic rate + no lymphocytic response = poor prognosis
- Sentinel lymph node biopsy - routine at time of excision
Sites:
- Sun-exposed skin (most common)
- Acral melanoma: Sole, palm, nail bed (in darker skin individuals - KIT mutation)
- Subungual melanoma: Nail bed - diagnosis delay hoti hai! Biopsy karo
- Uveal melanoma: GNAQ/GNA11 mutations
Treatment:
- Surgery: Wide local excision + sentinel LN biopsy
- BRAF-mutated (V600E): Vemurafenib/dabrafenib (dramatic response, but resistance ho sakta hai)
- Immunotherapy: Immune checkpoint inhibitors (anti-PD1, anti-CTLA4) - metastatic disease mein "remarkable tumor regression"
🔥 QUICK COMPARE TABLE (Copy karo apni notes mein!)
| Feature | BCC | SCC | Melanoma |
|---|---|---|---|
| Mutation | PTCH1 | TP53, RAS | BRAF, RAS → then p16, PTEN, p53 |
| Appearance | Pearly + telangiectasia | Nodular, scaly, ulcerated | Variable color, irregular |
| Metastasis | Rare | ~4% at diagnosis | Very common if thick |
| Marjolin's | No | YES | No |
| Gorlin Syndrome | YES | No | No |
| Prognostic factor | Local recurrence | Thickness, depth | Breslow thickness |
| Treatment | Excision, vismodegib | 6mm margin, Mohs | WLE + SNBx + BRAF inhibitor/immunotherapy |
💡 MNEMONICS FOR EXAM
"BCC ke liye PTCH (Patch lagao)" - PTCH1 = BCC
"SCC se MARJOLIN" - Marjolin's ulcer = Malignant degeneration in burn scar/chronic ulcer
"ABCDE hai MELANOMA ka pehchaan ka tarika"
"BRAF bahut BURA hai melanoma mein" - BRAF V600E mutation = targeted therapy target
Breslow moti = buri prognosis - thickness badhegi to prognosis kharab hogi
Sources: Robbins & Kumar Basic Pathology (9780323790185) + Sabiston Textbook of Surgery (9780443124341)
This is a shared conversation. Sign in to Orris to start your own chat.