Leptopsira IgM Antibodies
Reading File
Finding Sources
Finding Sources
Searching PubMed
Leptospira IgM antibody diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a detailed, well-sourced answer on Leptospira IgM antibodies.
Leptospira IgM Antibodies
Overview
Leptospira IgM antibodies are serologic markers of acute leptospirosis infection. Their detection forms the basis of rapid immunodiagnostic testing for this widespread zoonosis. IgM antibodies typically appear during the immune (second) phase of disease, coinciding with bacterial clearance from the blood and the development of clinical complications.
When IgM Appears - Disease Phases
Leptospirosis follows a biphasic course:
| Phase | Timing | Biology |
|---|---|---|
| Leptospiremic phase | Days 1-7 | Bacteremia; spirochetes in blood, CSF, urine |
| Immune phase | Week 2 onward | Antibody rise (IgM); organisms cleared from blood; organ complications develop |
Clearing of bacteremia coincides with the appearance of circulating antibody. IgM rises during the second phase, which itself suggests an immunologic component to disease pathogenesis - this is supported by the typical failure to recover the organism from the CSF during leptospiral meningitis, and the lack of antimicrobial response when antibiotics are given at this stage. - Sherris & Ryan's Medical Microbiology, 8th Ed.
Serologic testing is often negative early in the course of the disease, which is the primary limitation of IgM-based assays.
Diagnostic Methods Using IgM
1. IgM ELISA (Most Practical Rapid Test)
An IgM-specific dot enzyme-linked immunosorbent assay (ELISA) has been found to be specific in diagnosing leptospirosis in endemic areas. - Comprehensive Clinical Nephrology, 7th Ed.
However, suboptimal sensitivity and specificity rates have been reported with IgM ELISA for acute leptospirosis. Performance varies significantly across different populations, and test kits must be evaluated in specific populations before deployment. - Brenner & Rector's The Kidney
2. Microscopic Agglutination Test (MAT) - Gold Standard
- The benchmark reference test for leptospirosis
- Detects serovar-specific agglutinating antibodies (mostly IgM in acute infection)
- Complex: requires maintenance of live Leptospira cultures
- Restricted to reference laboratories
- Diagnostic titers:
- Single indirect hemagglutination titer 1:200 to <1:800 = suggestive
- Single titer ≥1:800 = confirmed infection
- 4-fold or higher rise in convalescent sample = confirmed infection
-
- Brenner & Rector's The Kidney
3. Macroscopic Agglutination Test
Can be used as a screening test but is not specific.
4. PCR - Preferred Over Serology Early in Disease
PCR-based nucleic acid amplification of blood, urine, or CSF is much more sensitive than culture and can be performed early in the course of the disease - before IgM has risen to detectable levels. However, it is not widely available.
5. Rapid Diagnostic Test Kits (RDTs)
WHO-recommended diagnostics include MAT, direct culture, and PCR - but these require advanced facilities. Rapid diagnostic kits that test serum IgM antibodies are an alternative in resource-limited settings. Diversity in accuracy across different populations makes local validation essential before use. - Comprehensive Clinical Nephrology, 7th Ed.
Role of IgM in Pathogenesis and Renal Involvement
The rise in IgM coincides with the immune phase, during which renal damage becomes prominent. The immunologic mechanisms include:
- Mild and transient mesangioproliferative glomerulonephritis with IgM and C3 deposition seen on renal biopsy
- Direct tubular injury via outer membrane proteins (LipL32, LipLoa22, LipL41, Lig family) acting through TLR-2 / NF-kB pathways
- Indirect toxicity via hemodynamic instability, hyperbilirubinemia, and rhabdomyolysis
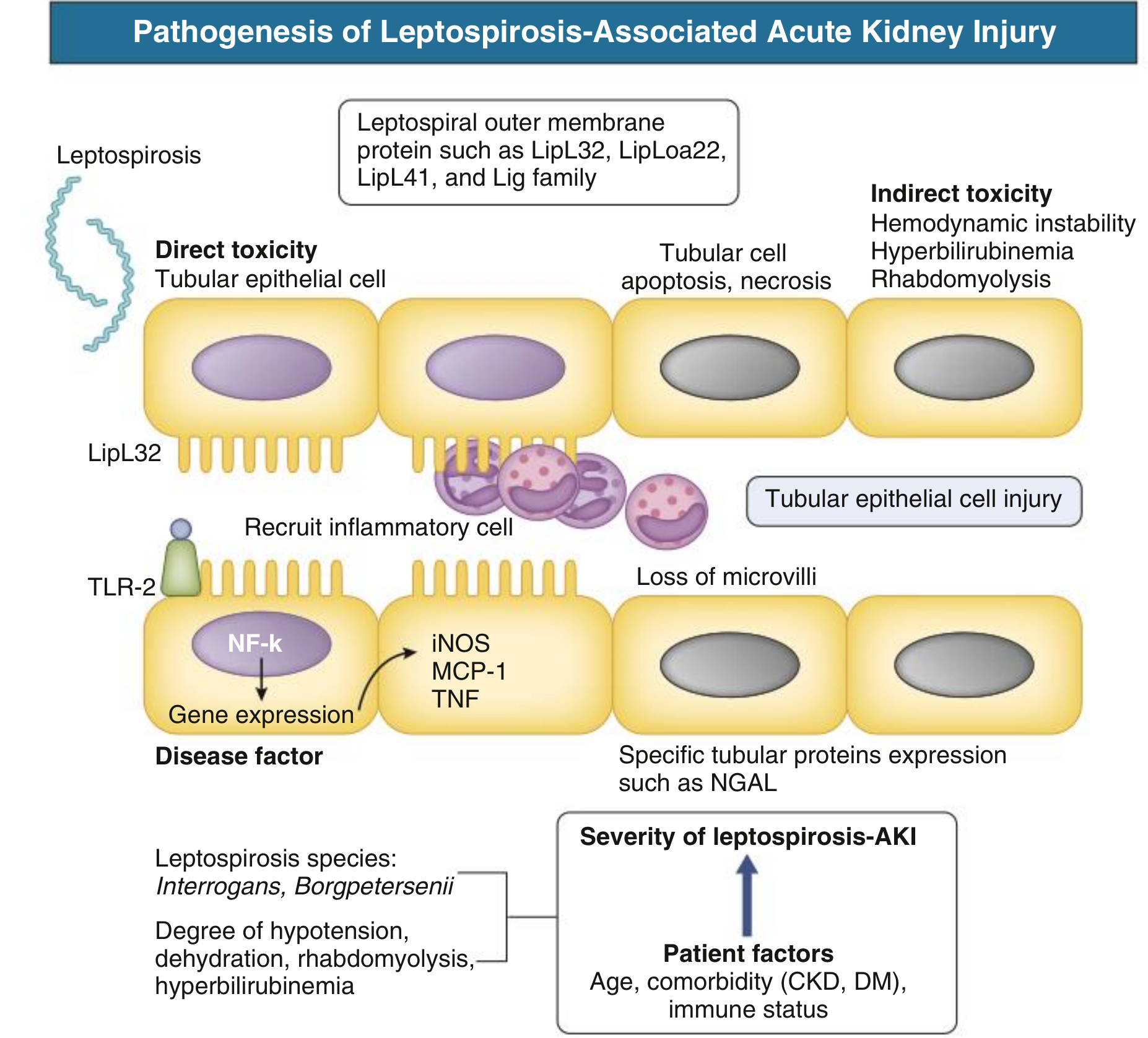
Fig. - Pathogenesis of leptospirosis-associated AKI, showing direct (LipL32/TLR-2/NF-kB) and indirect toxicity mechanisms. - Comprehensive Clinical Nephrology, 7th Ed.
Diagnostic Challenges Summary
| Challenge | Detail |
|---|---|
| Early-phase serology | IgM not yet detectable in first week; PCR preferred |
| False negatives | IgM ELISA has suboptimal sensitivity |
| Cross-reactivity | False positives can occur in other spirochetal infections (syphilis, Borrelia); aPLs (antiphospholipid antibodies) can be induced by Leptospira |
| Serovar diversity | MAT is serovar-specific; a battery of live cultures must be maintained |
| Population variability | Kit performance must be locally validated |
Clinical Context
Triad suggesting leptospirosis: fever + jaundice + AKI
Leptospirosis is the most widespread zoonosis globally, with ~1 million cases/year and ~58,900 fatalities annually. Most severe cases represent Weil disease - characterized by jaundice, renal failure, hemorrhage, and myocarditis. IgM serology is the most practical diagnostic approach in endemic and resource-limited settings. - Comprehensive Clinical Nephrology, 7th Ed.
Recent Evidence
A 2024 systematic review and meta-analysis (PMID 38326762) evaluated the diagnostic accuracy of MAT, PCR, and IgM ELISA to Leptospira fainei serovar Hurstbridge - confirming the ongoing need to assess IgM test performance across different diagnostic platforms and populations.
Key takeaway: Leptospira IgM antibodies are the practical cornerstone of leptospirosis serology but are limited by late appearance (after the first week), variable sensitivity/specificity of ELISA kits, and population-dependent performance. MAT remains the gold standard, while PCR is preferred for early diagnosis. In endemic/resource-limited settings, rapid IgM-based kits are a reasonable alternative when locally validated.
This is a shared conversation. Sign in to Orris to start your own chat.