Anatomy of eye lid according to Vishal singh
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching the Web
Vishal Singh ophthalmology eyelid anatomy layers
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed to provide a thorough answer. Note that the library does not contain a book specifically by "Vishal Singh" - this appears to be a reference to a popular Indian ophthalmology educator/lecturer (commonly referenced on YouTube/social media for ophthalmology teaching). The content below is drawn from standard authoritative ophthalmology and surgical sources.
Anatomy of the Eyelid
Note: The library does not contain a textbook specifically authored by "Vishal Singh." The content below follows the standard eyelid anatomy framework taught in Indian ophthalmology education (as taught by Vishal Singh and others), sourced from authoritative ophthalmology and surgical references in the medical library.
Overview - The Two Lamellae
The eyelids are protective coverings of the eye. At the level of the tarsal plates, both upper and lower eyelids are divided into two lamellae:
| Lamella | Components |
|---|---|
| Anterior lamella | Skin + Orbicularis oculi muscle |
| Posterior lamella | Tarsus (tarsal plate) + Conjunctiva |
Between the two lamellae lie the finely interdigitating eyelid retractors. The two lamellae have separate blood supplies - important for eyelid reconstruction.
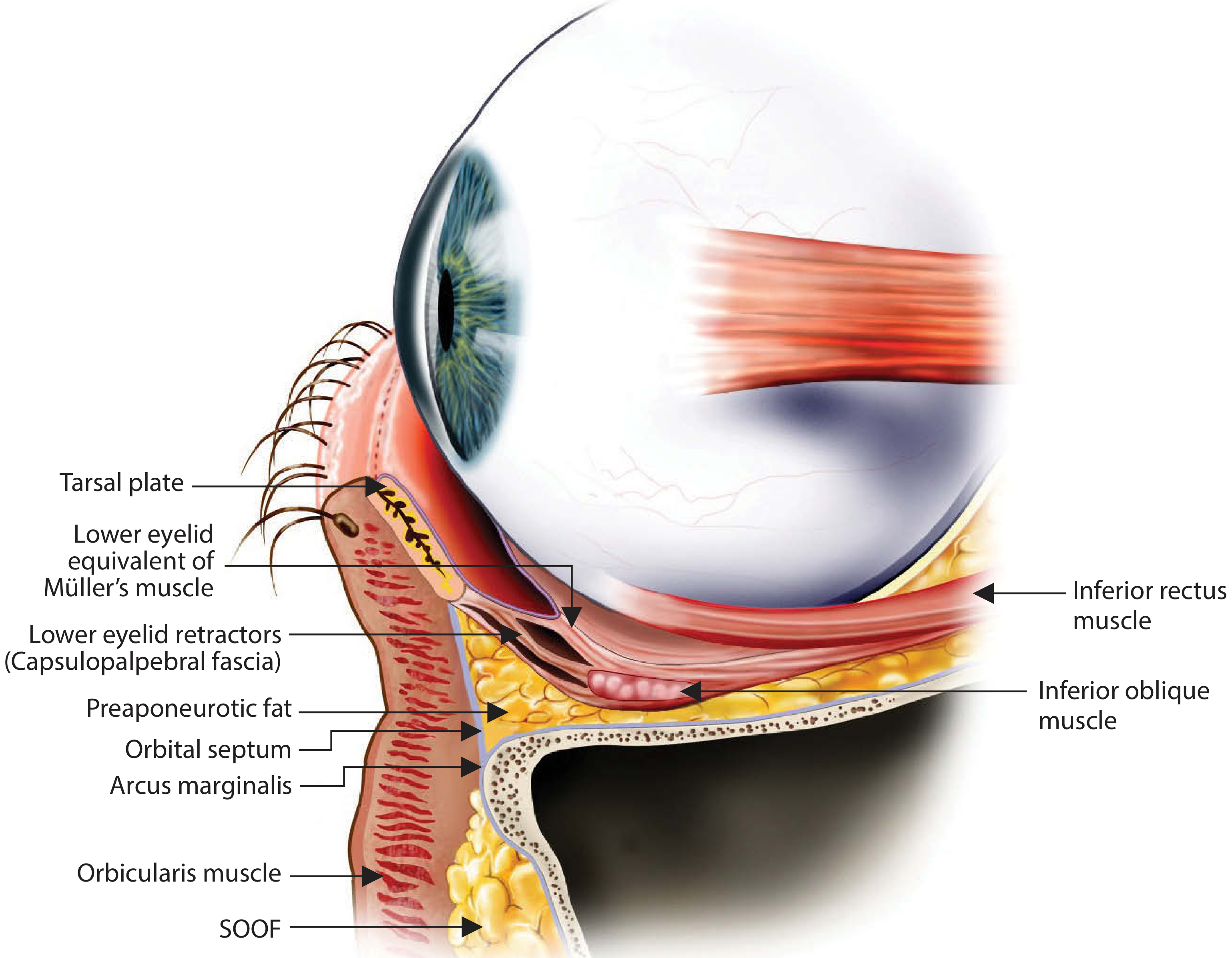
Cross-section showing eyelid layers: tarsal plate, Müller's muscle, capsulopalpebral fascia, preaponeurotic fat, orbital septum, arcus marginalis, orbicularis muscle, and SOOF.
1. SKIN
- The thinnest skin of the body - almost no reticular dermis
- Highly vascular - heals rapidly with minimal scarring
- Thickens rapidly as it approaches the orbital rim and hair-bearing periorbital areas
2. ORBICULARIS OCULI MUSCLE (Anterior lamella)
The orbicularis oculi is a subcutaneous muscle that acts as the sphincter of the eyelid.
Nerve supply: Temporal and zygomatic branches of the facial nerve (CN VII)
Three divisions:
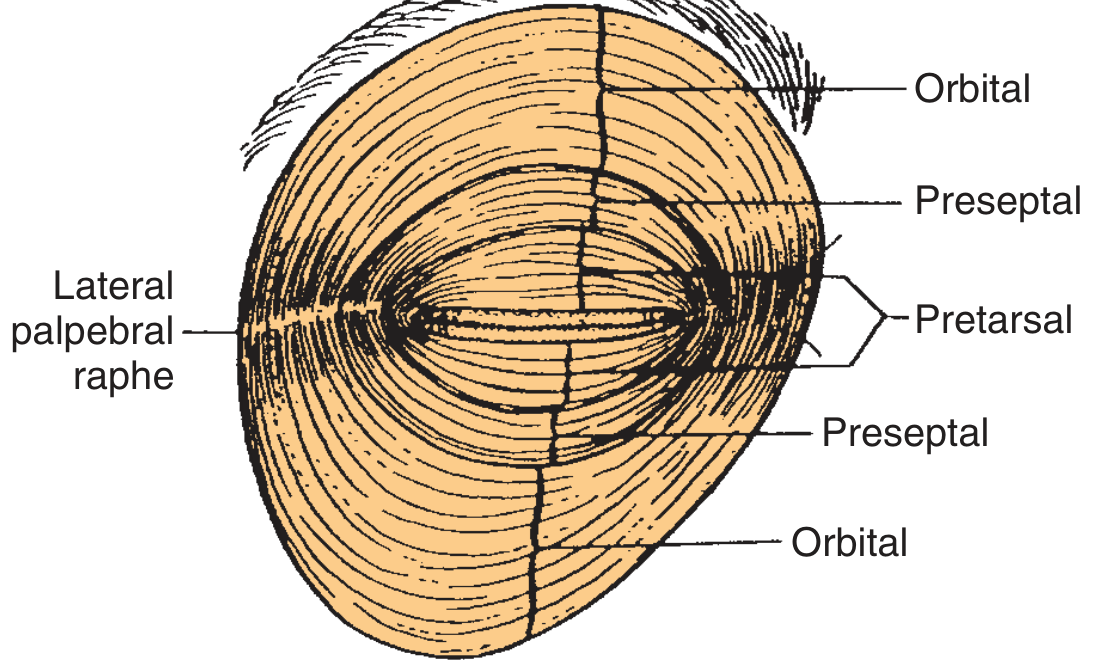
| Division | Location | Function |
|---|---|---|
| Pretarsal | Over tarsal plate | Involuntary blinking |
| Preseptal | Over orbital septum | Both involuntary & voluntary |
| Orbital | Over orbital rim | Voluntary winking/forceful closure |
- The pretarsal and preseptal portions have two heads at their origin (related to lacrimal crest and canthal tendon)
- Laterally, all three segments fuse to form the lateral canthal tendon, which inserts into the Whitnall tubercle
- The orbicularis is also essential for the lacrimal pump mechanism - propels tears into puncta, canaliculi, and lacrimal sac. Facial nerve palsy disrupts this, leading to epiphora.
3. ORBITAL SEPTUM
- Lies just deep to the orbicularis oculi muscle
- Forms the anterior border of the orbit
- Confines the orbital fat
- It is a fibrous sheath formed at the orbital rims at the arcus marginalis (extension of orbital periosteum)
- In Caucasians: the septum fuses with the levator aponeurosis ~3 mm above the superior tarsal border
- In Asians: this fusion occurs more inferiorly (below the superior tarsal border), allowing orbital fat to prolapse anteriorly - this prevents a prominent upper lid crease and creates fullness of the upper eyelid
4. EYELID FAT PADS
Upper eyelid: Two fat compartments - medial (nasal) and central preaponeurotic fat pads
Lower eyelid: Three fat compartments - medial, central, and lateral
5. EYELID RETRACTORS
Upper Eyelid Retractors
a) Levator palpebrae superioris (LPS)
- Main retractor of the upper eyelid
- Inserts into the upper third of the tarsal plate via the levator aponeurosis
- Some fibers fuse with the orbital septum 2-5 mm above the superior tarsal border and insert into the skin, forming the upper eyelid crease
- Attaches medially to the medial canthal tendon and laterally to the lateral canthal tendon
- Suspended by Whitnall's ligament superiorly
b) Müller's Muscle (Superior tarsal muscle)
- Arises from the undersurface of the levator aponeurosis just below Whitnall's ligament
- Courses inferiorly 10-12 mm to attach to the superior tarsal plate
- Nerve supply: Sympathetic (loss causes 2-3 mm ptosis in Horner's syndrome)
- Produces 2-3 mm of eyelid elevation
- Anteriorly adherent to levator aponeurosis; posteriorly loosely adherent to conjunctiva
Lower Eyelid Retractors
a) Capsulopalpebral fascia - the lower lid equivalent of levator aponeurosis
- Originates from the fascia of the inferior rectus muscle
- Inserts on the inferior tarsal border
- Mimics movement of the inferior rectus muscle
b) Inferior tarsal muscle - the lower lid equivalent of Müller's muscle
- Arises from the undersurface of the capsulopalpebral fascia
- Sympathetically innervated
6. TARSUS (Tarsal Plate - Posterior lamella)
- Dense fibrous connective tissue forming the skeleton of the eyelids
- Each plate is 25-30 mm in horizontal dimension
- Vertical height:
- Upper eyelid tarsus: 10-12 mm
- Lower eyelid tarsus: 3-5 mm
- Contains Meibomian glands (modified sebaceous glands - ~25 in upper, ~20 in lower lid) that open at the lid margin
7. CONJUNCTIVA (Posterior lamella)
- Innermost surface of the eyelid
- Nonkeratinized stratified squamous epithelium with goblet cells (produce mucous layer of tear film)
- Palpebral conjunctiva: lines the eyelid
- Bulbar conjunctiva: lines the globe
- They meet at the fornix
Surface Anatomy - Key Measurements
| Parameter | Measurement |
|---|---|
| Horizontal palpebral fissure | 28-30 mm |
| Vertical palpebral fissure | 9-10 mm |
| Intercanthal distance | 25-30 mm |
| Upper lid crease (women) | 10-12 mm above lid margin |
| Upper lid crease (men) | 7-8 mm above lid margin |
| Upper tarsal plate height | 10-12 mm |
| Lower tarsal plate height | 3-5 mm |
- Upper eyelid margin: rests midway between the superior corneal limbus and the pupil
- Lower eyelid margin: abuts the inferior corneal limbus
- The lateral canthal angle is more acute and sits 2 mm higher than the rounded medial canthal angle
Glands of the Eyelid (Summary)
| Gland | Location | Secretion |
|---|---|---|
| Meibomian glands | Within tarsus | Lipid (oily) layer of tear film |
| Glands of Zeis | Associated with eyelash follicles | Sebaceous |
| Glands of Moll | Between eyelash follicles | Sweat (modified apocrine) |
| Krause glands | Fornix | Accessory lacrimal |
| Wolfring glands | Superior tarsal border | Accessory lacrimal |
Sources: Cummings Otolaryngology Head and Neck Surgery, Ch. 26; Kanski's Clinical Ophthalmology 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.