From which lead should we start to interpret ecg? Explain with ecg images
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG interpretation which lead to start with systematic approach lead II
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Searching the Web
ECG interpretation start with lead II rhythm strip then 12 lead systematic order
Reading Web Page
http://www.hvt-journal.com/articles/art254
Searching the Web
12 lead ECG interpretation order lead II aVR precordial leads diagram
Loading Image
Loading Image
Loading Image
Now I have everything needed for a comprehensive, image-rich answer. Let me compose it.
Which Lead to Start ECG Interpretation From?
The Short Answer: Start with Lead II (or the Long Rhythm Strip)
The universal convention is to begin ECG interpretation with Lead II - specifically the long rhythm strip at the bottom of a standard 12-lead printout. Lead II is oriented parallel to the mean electrical axis of the heart (roughly 60°), which means:
- The P wave is tallest and most upright (best visibility)
- The QRS complex is clearly positive
- It is ideal for assessing rhythm and identifying the origin of the pacemaker
If a dedicated rhythm strip is printed (usually a 10-second Lead II strip at the bottom), start there.
The ECG Waveform - What You're Looking At
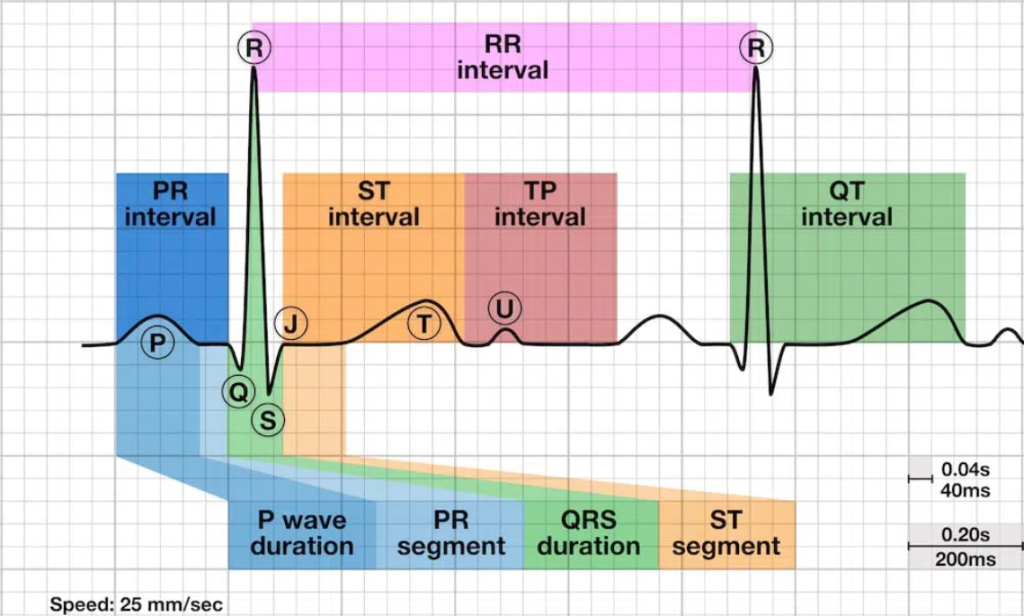
Each beat on ECG consists of:
- P wave - atrial depolarization
- QRS complex - ventricular depolarization
- T wave - ventricular repolarization
- U wave - occasionally visible, repolarization of Purkinje fibers
Lead Orientation: Why Lead II is First

The 12 leads divide into anatomical groups. Lead II sits in the inferior group (II, III, aVF), and because it runs from the right arm to the left leg, it aligns almost perfectly with normal cardiac electrical flow - giving the clearest P waves in the body.
- Lead aVR is the "mirror" lead - in normal sinus rhythm, ALL waves (P, QRS, T) are negative in aVR because all depolarization moves away from the right shoulder
- This makes aVR a useful sanity check: if it looks normal, your leads are probably not reversed
The Systematic Approach: 2 Steps, 6+ Parameters

Step 1: Descriptive Analysis (in this order)
Step 1 - Check calibration and technical quality
- Standard: 10 mm/mV, paper speed 25 mm/sec
- Check for artifact, poor contact, lead misplacement
Step 2 - Rhythm (START HERE in Lead II)

In Lead II, apply the "Watch your Ps & Qs and the 3 Rs" mnemonic:
- Are there P waves? Is the P upright in Lead II?
- Is the QRS wide or narrow?
- Is the rhythm Regular?
- What is the Rate?
- Are P waves Related to QRS? (1:1 relationship?)
Step 3 - Heart Rate
- Regular rhythm: 300 ÷ number of large boxes between R-R peaks
- Alternatively: count QRS complexes in 10-second strip × 6
Step 4 - Intervals (measured in Lead II or V1)
| Interval | Normal limit |
|---|---|
| PR interval | 0.12 - 0.20 sec (3-5 small boxes) |
| QRS duration | < 0.12 sec (< 3 small boxes) |
| QT interval | < half the R-R interval |
Step 5 - Axis (use Lead I and aVF together)
- Normal axis: Lead I positive + aVF positive (0° to +90°)
- Left axis deviation: Lead I positive + aVF negative
- Right axis deviation: Lead I negative + aVF positive
Step 6 - Hypertrophy / Chamber enlargement
- P wave in Lead II > 2.5 mm tall or > 0.12 sec wide = atrial enlargement
- R wave in aVL > 11 mm, or Sokolow-Lyon index > 35 mm = LVH
Then Go Through the 12 Leads in Anatomical Groups

After Lead II rhythm analysis, read the full 12-lead ECG by territory:
| Territory | Leads | Coronary Supply |
|---|---|---|
| Inferior | II, III, aVF | Right coronary artery (RCA) |
| Lateral | I, aVL, V5, V6 | Left circumflex artery |
| Anterior/Septal | V1, V2 | LAD (septal branch) |
| Anterior | V3, V4 | LAD |
Practical lead reading order:
- Lead II (rhythm strip) - rhythm, rate, P waves
- Lead I and aVF - axis
- aVR - confirms no lead reversal (should be all negative)
- Limb leads: I, II, III, aVR, aVL, aVF - inferior/lateral walls
- Precordial leads V1-V6 - septal, anterior, lateral walls (look for R-wave progression: small R in V1, growing through to V6; transition at V3/V4)
Harrison's 14-Parameter Systematic Checklist
From Harrison's Principles of Internal Medicine (22nd Ed):
"Accurate analysis of ECGs requires thoroughness and care. A systematic approach is essential. The following 14 parameters should be analyzed carefully in every ECG: (1) standardization/calibration and technical features; (2) rhythm; (3) heart rate; (4) PR interval/AV conduction; (5) QRS interval; (6) QT/QTc intervals; (7) mean QRS electrical axis; (8) P waves; (9) QRS voltages; (10) precordial R-wave progression; (11) abnormal Q waves; (12) ST segments; (13) T waves; and (14) U waves."
Step 2: Clinical Impression
After the descriptive analysis, correlate your findings with the clinical picture (chest pain, dyspnea, syncope, palpitations) to form the final interpretation. This is where you connect a finding like "ST elevation in II, III, aVF" to "inferior STEMI from RCA occlusion."
Key takeaway: Always start with Lead II for rhythm because it gives the clearest P waves and best represents the normal direction of cardiac electrical flow. Then work through the leads in anatomical groups. Never read leads randomly - a systematic order prevents missing subtle abnormalities.
This is a shared conversation. Sign in to Orris to start your own chat.