Tell me about fracture
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from authoritative sources. Let me compile the full answer.
Fracture
A fracture is a break in the continuity of bone. It may be subtle (a hairline crack) or obvious (complete disruption with displacement). Clinically, fractures present with a history of trauma, pain, tenderness, swelling, loss of function, abnormal motion, and deformity. - Rosen's Emergency Medicine, p. 535
Definition & Mechanism
Bone breaks when the applied force exceeds its mechanical strength. Forces can be direct (impact), indirect (torsion, bending), or repetitive (stress). Fractures also occur through pathologically weakened bone (pathologic fractures) without abnormal force.
Classification
1. Open vs. Closed
- Closed fracture: skin and soft tissue overlying the fracture are intact
- Open (compound) fracture: fracture is or has been exposed to the external environment - higher infection risk, requires urgent management. When in doubt, always treat as open. - Rosen's Emergency Medicine, p. 535
2. Direction of Fracture Line
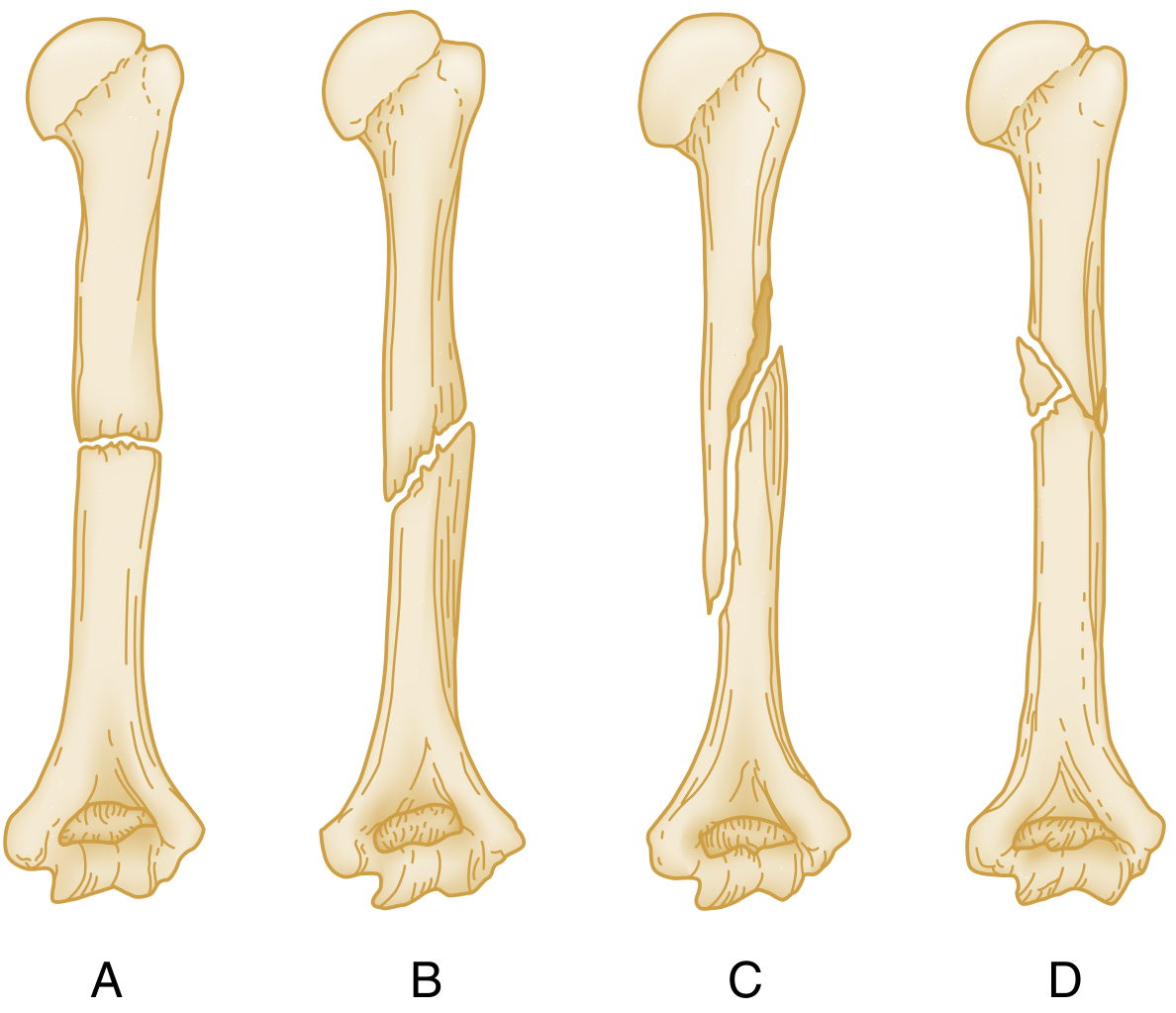
| Type | Description |
|---|---|
| Transverse | Fracture at right angles to the long axis of the bone |
| Oblique | Fracture runs oblique to the long axis |
| Spiral | Results from rotational/torque force; encircles the shaft (may suggest child abuse in children) |
| Comminuted | More than two fragments |
3. Complete vs. Incomplete
- Complete: full break through both cortices
- Incomplete: only one cortex involved (e.g., greenstick fracture in children)
4. Additional Descriptors (Box 41.1, Rosen's EM)
- Involvement of articular surface (%)
- Avulsion - bone pulled off by a tendon or ligament
- Impaction - fragments driven into each other
- Depression - seen in skull/tibial plateau
- Compression - vertebral bodies
5. Special Types
- Stress (fatigue) fracture: repetitive loading without acute trauma; common in tibia, fibula, metatarsals, femoral neck; may not be visible on initial plain films
- Pathologic fracture: through bone weakened by disease (tumor, osteoporosis, infection, Paget's)
- Epiphyseal fractures (children): classified by the Salter-Harris system (Types I-V), which describes involvement of the growth plate, epiphysis, and metaphysis
6. Fragment Position
- Displacement: deviation of the distal fragment from normal position (described as % of bone width or in mm)
- Angulation: deviation of the longitudinal axis; direction described by the apex (valgus = apex toward midline; varus = apex away from midline)
- Rotation: the distal fragment is rotated relative to the proximal
Fracture Healing
Healing proceeds through well-defined stages. The environment can be:
- Relatively stable (cast, brace, nail, external fixator) → secondary/indirect healing via callus
- Absolutely stable (rigid plate) → primary/direct healing without visible callus
Stages of Secondary (Indirect) Bone Healing
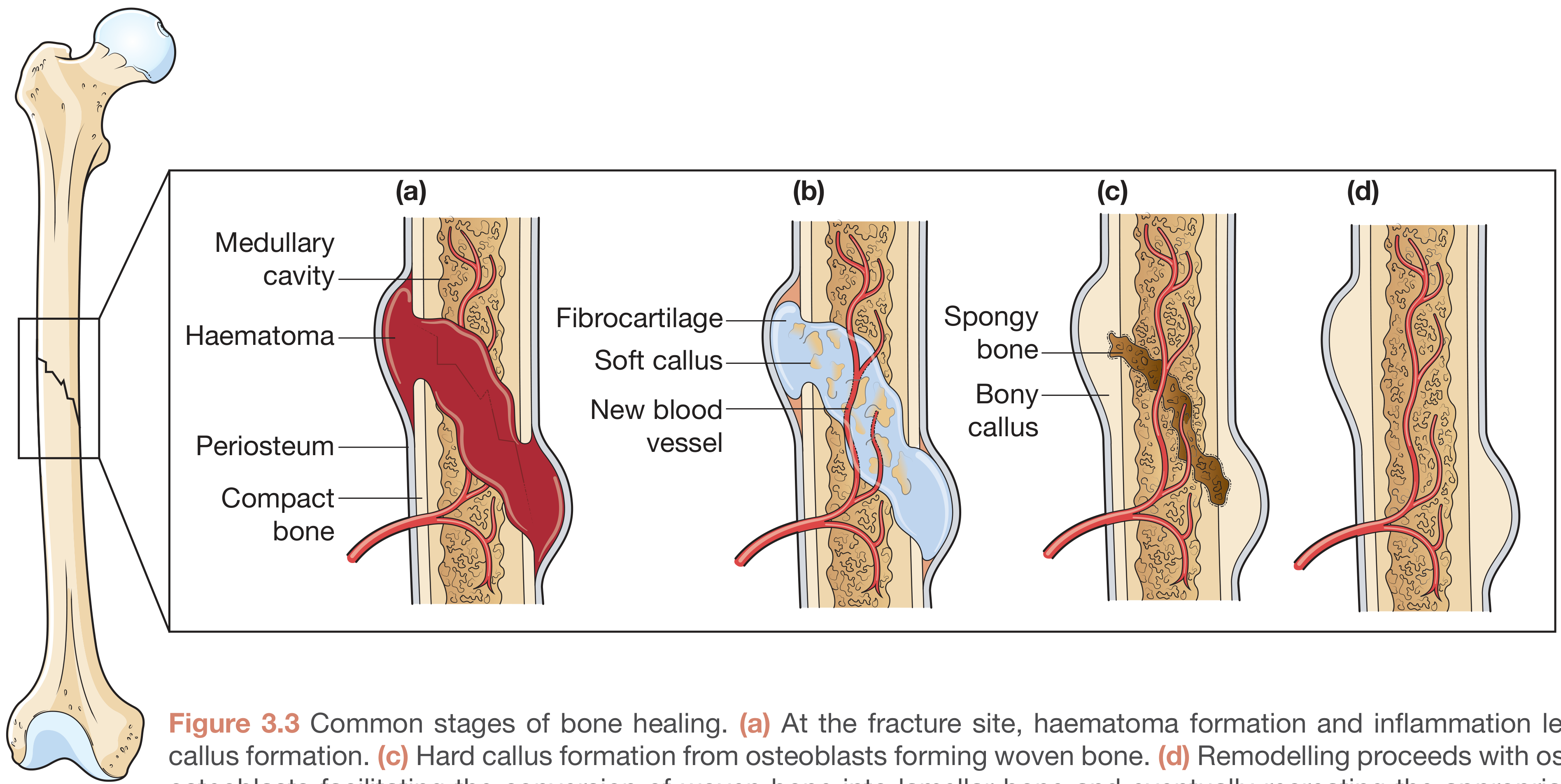
| Stage | Timing | What Happens |
|---|---|---|
| 1. Inflammatory / Haematoma | Immediate - day 3 | Ruptured vessels fill the fracture with hematoma. Fibrin clot forms. Little structural rigidity (tolerates 100% strain). Rubor, tumor, calor, dolor. |
| 2. Soft Callus | Days 3 - ~3 weeks | Granulation tissue replaces hematoma. Periosteal and endosteal intramembranous bone formation begins. Endochondral ossification deposits fibrocartilage near the fracture. The callus is flexible but adds some stability. |
| 3. Hard Callus | Weeks 3 - 12 | Soft callus mineralizes. Endochondral ossification converts cartilage to woven bone. Callus deposited away from the neutral axis greatly increases bending stiffness (stiffness ∝ 4th power of distance from neutral axis). |
| 4. Remodelling | Months - years | Osteoclasts resorb excess callus. Woven bone is replaced by lamellar bone. Normal bone architecture is gradually restored. |
- Rockwood and Green's Fractures in Adults, 10th ed 2025, p. 39
- Bailey and Love's Short Practice of Surgery, 28th ed
Primary (Direct) Bone Healing
Occurs when fracture surfaces are held in rigid anatomical contact (as after ORIF with compression plates). Haversian remodeling units (cutting cones) cross the fracture gap directly, without callus formation. This is the aim of open reduction and internal fixation surgery.
Factors Affecting Healing
Healing is impaired by: infection, poor vascular supply, severe comminution, interposed soft tissue, excessive motion at fracture site, metabolic disease (osteoporosis, diabetes), smoking, malnutrition, corticosteroids, and NSAIDs.
Clinical Assessment
History: mechanism of injury, energy level, time elapsed, neurovascular symptoms
Examination: look, feel, move; assess skin (open/closed), neurovascular status distally, compartment syndrome signs (pain on passive stretch, tense swelling, pulselessness, paresthesia, paralysis)
Imaging:
- Plain X-ray: minimum two views (AP + lateral), include joint above and below
- CT: for complex intra-articular, pelvic, or spinal fractures
- MRI: occult fractures, stress fractures, bone marrow edema
- Bone scan: stress fractures not visible on plain films
Management Principles
The goal is anatomical (or acceptable) reduction and stabilization to allow healing, restore function, and prevent complications.
Reduction
- Closed reduction: manipulation under anesthesia/sedation, then cast/splint immobilization
- Open reduction: surgical exposure to achieve anatomical alignment, followed by internal fixation
Fixation Methods
| Method | Examples | Principle |
|---|---|---|
| Conservative | Cast, splint, traction | Relative stability; callus healing |
| Intramedullary nail | Tibia, femur shaft | Load-sharing; relative stability |
| Plate & screws | Radius/ulna, distal femur | Absolute or relative stability |
| External fixator | Open fractures, polytrauma, temporizing | Relative stability |
| Arthroplasty | Elderly femoral neck fractures | Replaces the head instead of fixing |
Open Fracture Management
Open fractures require:
- Wound irrigation and debridement (within 6-24 hours based on Gustilo-Anderson grade)
- IV antibiotics (covering Gram-positive, with Gram-negative cover for higher grades)
- Stabilization of bone
- Wound coverage (primary, delayed primary, or flap)
Complications
| Early | Late |
|---|---|
| Hemorrhage (femur: up to 1.5L blood loss) | Malunion (healed in wrong position) |
| Nerve/vessel injury | Nonunion (failure to heal) |
| Compartment syndrome | Avascular necrosis (scaphoid, femoral head) |
| Fat embolism syndrome | Osteoarthritis (intra-articular fractures) |
| Wound infection (open) | Reflex sympathetic dystrophy |
| Venous thromboembolism | Implant failure |
Fractures in Children
Children's bones have a thicker, more osteogenic periosteum and active growth plates, which affect both fracture patterns and healing:
- Greenstick fracture: incomplete fracture, one cortex intact
- Torus (buckle) fracture: compression failure of the cortex, common in distal radius
- Plastic deformation: bone bends without a discrete fracture line
- Physis involvement: Salter-Harris classification guides management and predicts growth disturbance risk (Type V = crush of growth plate = worst prognosis)
Sources: Rosen's Emergency Medicine 9th ed, Rockwood and Green's Fractures in Adults 10th ed (2025), Bailey and Love's Short Practice of Surgery 28th ed, Campbell's Operative Orthopaedics 15th ed (2026)
This is a shared conversation. Sign in to Orris to start your own chat.