Peripheral ulcerative keratitis
Reading File
Finding Sources
Searching PubMed
"peripheral ulcerative keratitis"
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from both Kanski's and Wills Eye Manual. Let me compile the full answer.
Peripheral Ulcerative Keratitis (PUK)
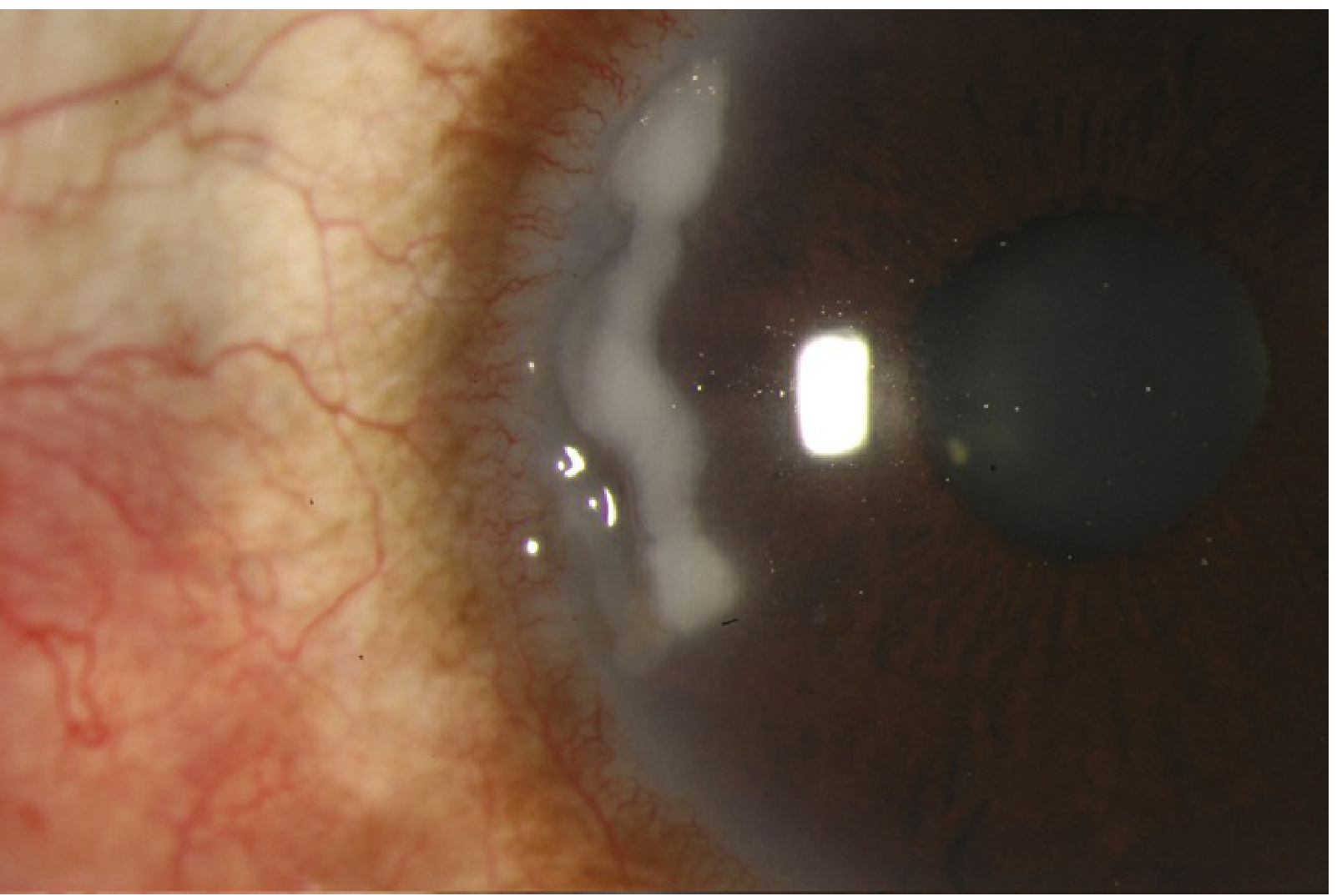
Slit lamp photograph of PUK: peripheral stromal infiltration and ulceration at the limbus (Wills Eye Manual)
Definition
PUK refers to inflammatory thinning and/or ulceration preferentially affecting the peripheral cornea, spreading circumferentially around the limbal margin. The term "PUK" is specifically used when the process is inflammatory in nature. It can precede or follow the onset of systemic disease, and its presence without apparent ocular cause is a red flag for a potentially life-threatening systemic collagen vascular disorder.
Pathogenesis
The mechanism involves several interacting steps:
- Immune complex deposition in the peripheral cornea (which is anatomically close to the limbal vasculature and hence exposed to circulating immune complexes)
- Episcleral and conjunctival capillary occlusion - leading to secondary cytokine release and inflammatory cell recruitment
- Upregulation of matrix metalloproteinases (collagenases) with reduced activity of their inhibitors, resulting in stromal digestion and ulceration
The peripheral cornea is uniquely susceptible because of its proximity to the limbal vessels and the relative lack of central corneal immune privilege at the periphery.
(Kanski's Clinical Ophthalmology, 10th ed.)
Systemic Associations
| Condition | Notes |
|---|---|
| Rheumatoid arthritis (RA) | Most common systemic cause. PUK is bilateral in ~30%; tends to occur in advanced/seropositive RA |
| Granulomatosis with polyangiitis (GPA / Wegener's) | Second most common. In contrast to RA, ocular disease is the initial presentation in ~50% of cases |
| Polyarteritis nodosa | Necrotizing vasculitis; severe PUK possible |
| Relapsing polychondritis | Notable because topical steroids may be helpful (unlike other forms) |
| Systemic lupus erythematosus (SLE) | Immune complex-mediated; often associated with retinal vasculitis |
| Crohn disease | Less common; IBD-associated |
| Others | Cataract surgery, previous HSV/VZV infection, leukemia (rare) |
Clinical Pearl: Nearly 50% of patients with PUK have an associated systemic disease - always investigate for connective tissue disease when PUK is found without obvious ocular cause.
Clinical Features
Symptoms:
- Pain, photophobia, red eye
- May occasionally be asymptomatic in early stages
Signs:
- Crescentic ulceration with an epithelial defect, stromal infiltration, and thinning at the limbus - no clear zone separates the ulcer from the limbus (this distinguishes it from marginal keratitis)
- Spread is circumferential and occasionally central
- Limbitis, episcleritis, or scleritis are usually present
- Unlike Mooren ulcer, extension into the sclera may occur
- Advanced disease: "contact lens cornea" (extreme generalized thinning) or corneal perforation
Special variant - Rheumatoid Paracentral Ulcerative Keratitis (PCUK):
- Distinct entity - punched-out lesion located more centrally
- Minimal infiltrate, quiet eye
- Perforation can occur rapidly
- Usually responds well to topical ciclosporin + bandage contact lens ± tissue glue, rather than systemic immunosuppression
(Kanski's Clinical Ophthalmology, 10th ed.)
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Mooren ulcer | No scleral involvement; undermined leading edge; idiopathic/diagnosis of exclusion |
| Marginal (staphylococcal hypersensitivity) keratitis | Clear zone between infiltrate and limbus; associated with blepharitis |
| Infectious keratitis | Cultures positive; usually central; contact lens history |
| Terrien marginal degeneration | Non-inflammatory; no epithelial defect; superior; lipid line at central edge |
| Pellucid marginal degeneration | Non-inflammatory; inferior cornea; protrusion above thinning |
| Sclerokeratitis | Scleritis is the primary lesion with secondary corneal involvement |
| Dellen | Drying artifact adjacent to elevated lesion; no true infiltrate |
| Neurotrophic/exposure keratopathy | Reduced corneal sensation; inferior interpalpebral zone |
Workup
- History - prior connective tissue disease, IBD, contact lens use, herpetic eye disease, prior surgery
- External exam - VZV scars, lagophthalmos, rosacea facies, blue scleral tinge
- Slit lamp - infiltrate, ulcer depth, scleritis, uveitis, corneal sensation
- Schirmer test - rule out severe dry eye as a contributor
- Dilated fundus exam - cotton-wool spots, posterior scleritis signs
- Corneal cultures - rule out infection first
- Systemic workup:
- ESR, CRP, CBC with differential
- Rheumatoid factor (RF), anti-CCP
- ANA, ANCA (c-ANCA / PR3-ANCA for GPA)
- ACE level, chest X-ray/CT (sarcoid, GPA)
- Refer to rheumatologist when connective tissue disease is suspected
Treatment
Topical / Local Measures
- Preservative-free lubricants (artificial tears/ointment)
- Topical antibiotics (e.g. erythromycin ointment) if epithelial defect present - prophylaxis against secondary infection
- Cycloplegic drops (cyclopentolate 1% or atropine 1% b.i.d.-t.i.d.) when anterior chamber reaction or pain present
- Topical steroids are generally avoided - they may worsen stromal thinning; relapsing polychondritis may be an exception
- Topical ciclosporin - particularly useful in PCUK variant
Adjunct Systemic Agents
- Doxycycline 100 mg b.i.d. - for its matrix metalloproteinase (MMP) inhibition properties (anti-collagenase effect)
- Ascorbic acid (Vitamin C) 1-2 g/day - collagen synthesis promoter
Immunosuppressive Treatment (mainstay for systemic PUK)
Treatment is managed in collaboration with a rheumatologist:
| Agent | Role |
|---|---|
| Systemic steroids (prednisolone 60-100 mg/day; or IV pulse methylprednisolone) | Acute control of inflammation |
| Methotrexate, mycophenolate mofetil, azathioprine | Steroid-sparing maintenance |
| Cyclophosphamide | Severe cases, especially GPA |
| Biologics (infliximab, adalimumab, rituximab) | Refractory cases - TNF inhibitors and anti-CD20 agents have shown efficacy in RA-associated and GPA-associated PUK |
Surgical Management
- Conjunctival excision/recession adjacent to the ulcer - removes a source of collagenase-secreting inflammatory cells; occasionally helpful when medical treatment fails
- Cyanoacrylate tissue adhesive - for impending perforation
- Amniotic membrane graft or conjunctival flap - for impending perforation
- Corneal transplantation (keratoplasty) - for actual perforation or visual rehabilitation once inflammation is controlled (requires immunosuppressive cover)
- Bandage contact lens + tissue glue - particularly for PCUK variant
- Patients with significant thinning should wear protective polycarbonate glasses during the day and an eye shield at night
Prognosis and Risk
- Untreated PUK associated with GPA or RA carries significant risk of corneal perforation and permanent visual loss
- The systemic disease itself (especially GPA, polyarteritis nodosa) can be life-threatening - PUK may be the presenting sign
- Mortality in RA-associated PUK was historically ~25% within 10 years if the systemic disease was not controlled
Recent Literature (2023-2026)
Recent reviews highlight the growing role of biologics in refractory PUK. A 2026 review (Guerrero-Acosta et al., J Clin Med, PMID 41682944) covers multimodal management including biologics as first-line in severe GPA-associated cases. A focused 2023 review on biologics in PUK (Clarke et al., PMID 37776666) documents TNF-alpha inhibitors (infliximab, adalimumab) and rituximab as effective options for refractory disease. A 2024 clinical review (Baquet-Walscheid et al., PMID 38776930) updates differential diagnosis criteria and therapeutic concepts.
Sources: Kanski's Clinical Ophthalmology 10th ed. (p. 241-242) | Wills Eye Manual (§4.22) | Goldman-Cecil Medicine | PubMed 2023-2026 reviews
This is a shared conversation. Sign in to Orris to start your own chat.