Hfpef latest guidelines
Reading File
Finding Sources
Searching PubMed
"heart failure with preserved ejection fraction" AND "guidelines"
Searching the Web
HFpEF latest guidelines 2024 2025 AHA ACC ESC treatment recommendations
Finding Sources
Reading Article
PMID: 38918060
Reading Article
PMID: 41953528
Reading Web Page
https://www.dovepress.com/clinical-advances-in-heart-failure…
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive, up-to-date summary of HFpEF guidelines incorporating the latest evidence through mid-2026.
HFpEF: Latest Guidelines and Evidence (2024-2026)
Definition and Diagnosis
HFpEF is defined as heart failure with LVEF ≥50%, supported by signs/symptoms of HF, elevated natriuretic peptides, and evidence of structural/functional diastolic abnormalities.
- NT-proBNP: ESC/AHA cut-off ≥125 ng/L; NICE uses higher thresholds (400-2000 ng/L: 6-week specialist referral; >2000 ng/L: urgent)
- Echocardiography: A 2025 update from the American Society of Echocardiography (PMID 40617625) revised recommendations for evaluating diastolic function and HFpEF diagnosis
- Scoring systems: HFA-PEFF and H2FPEF scores are used to guide diagnosis, though guideline uptake remains inconsistent
Pharmacological Treatment - Guideline Recommendations
1. SGLT2 Inhibitors (Cornerstone Therapy) - CLASS I / IIa
The most evidence-based treatment for HFpEF:
| Drug | Trial | Key Result | Guideline Class |
|---|---|---|---|
| Empagliflozin | EMPEROR-Preserved | 21% reduction in CV death/HF hospitalization (HR 0.79) | Class IIa B-R (AHA/ACC/HFSA 2022); Class I A (ESC 2023 Focused Update) |
| Dapagliflozin | DELIVER | ~20% RRR in CV death/HF hospitalization | Incorporated in ESC Class I |
The ESC 2023 Focused Update elevated SGLT2i to Class I, Level A after pooled evidence from both EMPEROR-Preserved and DELIVER. The AHA/ACC/HFSA 2022 guidelines list them as Class IIa B-R. SGLT2i should be considered in ALL HFpEF patients unless contraindicated. - Fuster and Hurst's The Heart, 15th ed.
2. Finerenone (Non-Steroidal MRA) - FDA Approved July 2025
The FINEARTS-HF trial (2024) showed finerenone significantly reduced total worsening HF events and CV death in HFmrEF/HFpEF with favorable hyperkalemia risk. The FDA approved finerenone for HFmrEF and HFpEF in July 2025. Incorporation into formal ESC guidelines (expected 2026) and AHA/ACC updates is anticipated. The ongoing REDEFINE-HF and CONFIRMATION-HF (finerenone + dapagliflozin) trials will refine its role further.
3. MRA (Spironolactone/Eplerenone) - CLASS IIb
- Spironolactone reduced HF hospitalization in HFpEF (TOPCAT trial) but did NOT reduce mortality
- AHA/ACC/HFSA 2022: Class IIb B-R (with caution given post-hoc nature of evidence)
- ESC guidelines: No formal recommendation
- Subanalysis of TOPCAT supports IIb for patients at the lower EF spectrum (45-55%), informing HFmrEF overlap
- Awaiting SPIRRIT-HFpEF trial results
4. RAAS Inhibition (ACEi / ARB / ARNI)
- ACEi, ARBs, and beta-blockers are reasonable and may reduce HF hospitalizations modestly but no mortality benefit is confirmed in HFpEF
- Sacubitril/valsartan (ARNI): PARAGON-HF did not meet its primary endpoint vs. valsartan, but FDA approved it for HFpEF based on benefit seen in patients with LVEF <normal (borderline/mildly reduced). ARNI is preferred over ACEi/ARB if LVEF is less than "normal" (see flowchart below)
- All three major guidelines (NICE, ESC, AHA) recommend ACEi/ARB/ARNI for symptom and hospitalization benefit
5. GLP-1/GIP Receptor Agonists (Emerging - Obesity-Phenotype HFpEF)
A major new therapeutic frontier, particularly for the obese HFpEF phenotype (which makes up ~80% of HFpEF cases in some cohorts):
| Drug | Trial | Key Findings |
|---|---|---|
| Semaglutide | STEP-HFpEF program | Improved symptoms, physical function, exercise capacity, weight and inflammation; reduced CV death/HF hospitalization composite in pooled analyses |
| Tirzepatide | SUMMIT trial | Clinically meaningful improvements in symptoms, exercise capacity, and composite HF/CV outcomes in obesity-related HFpEF |
These are not yet in formal HF guidelines but are strongly anticipated in the forthcoming 2026 ESC HF Guidelines update. Per the 2026 systematic review (PMID 41953528), they represent a "promising extension beyond SGLT2 inhibitors" in cardiometabolic HFpEF.
6. Loop Diuretics
- Used for fluid overload/congestion - mainstay for symptom relief
- No mortality benefit; titrate to euvolemia
- Does not modify disease course
Non-Pharmacological and Comorbidity Management
This is the backbone of HFpEF therapy given the high comorbidity burden:
| Comorbidity | Intervention |
|---|---|
| Hypertension | Treat aggressively; BP target <130/80 mmHg (both AHA/ACC and ESC). A 2025 meta-analysis (PMID 40410293) found SBP <130 mmHg associated with better outcomes in HFpEF |
| Atrial fibrillation | Rate or rhythm control; catheter ablation IIa for HFpEF + AF (2023 ACC/AHA/ACCP/HRS AF guidelines) |
| Obesity | Weight loss, GLP-1 RA (emerging) |
| T2DM | SGLT2i serve dual purpose (glucose + HF outcomes) |
| OSA | Screen and treat; CPAP |
| CAD | Revascularization per standard guidelines |
| Iron deficiency | FAIR-HFpEF trial (2024): ferric carboxymaltose improved exercise capacity; IV iron may be considered |
| Exercise/Rehab | Structured exercise training improves quality of life and exercise capacity (Class IIa) |
Treatment Algorithm Summary
The Washington Manual of Medical Therapeutics flowchart:
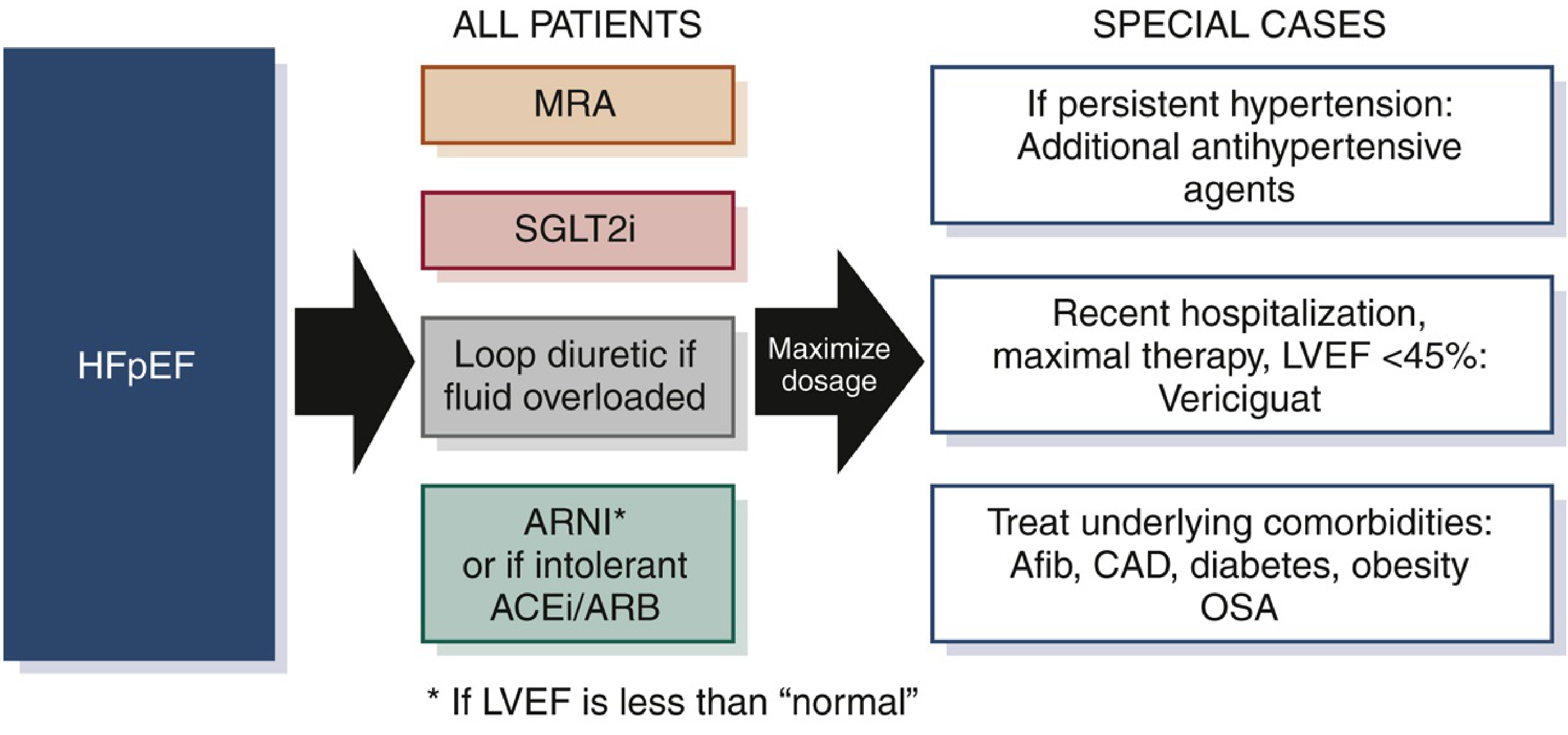
All patients: MRA + SGLT2i + Loop diuretic (if fluid overloaded) + ARNI (or ACEi/ARB if LVEF near normal)
Special cases: Persistent HTN → add antihypertensives; Recent hospitalization on maximal therapy with LVEF <45% → consider Vericiguat; Treat comorbidities (AF, CAD, DM, obesity, OSA)
Key Differences Between Major Guidelines (2022-2025)
| Recommendation | AHA/ACC/HFSA 2022 | ESC 2023 Focused Update |
|---|---|---|
| SGLT2i | Class IIa B-R | Class I A |
| MRA (spironolactone) | Class IIb B-R | No recommendation |
| Finerenone (HFpEF) | Not yet included | Expected in 2026 update |
| ARNI | Consider if LVEF < normal | Class IIb |
| Diuretics for congestion | Class I | Class I |
What's Coming: The 2026 ESC HF Guidelines
The 2026 ESC HF Guidelines are expected to include:
- Finerenone recommendation (following FINEARTS-HF and FDA approval)
- Possible GLP-1 RA recommendations for obese HFpEF phenotype
- Updated diagnostic criteria for diastolic function (ASE 2025 update)
- Phenotype-specific treatment pathways (obese, atrial fibrillation, CKD-driven HFpEF)
The iCARDIO 2025 Global Implementation Guidelines also provide a practical global framework incorporating these advances.
Key Bottom Line: No therapy has proven mortality benefit in HFpEF - the field is shifting toward HF hospitalization reduction and symptom improvement. SGLT2 inhibitors are the closest to a disease-modifying pillar (Class I per ESC). Finerenone (FDA-approved July 2025) is the next major addition. GLP-1/GIP agonists are highly promising for the obese phenotype. Aggressive comorbidity management remains essential for all patients.
This is a shared conversation. Sign in to Orris to start your own chat.