/visualize anterior shoulder dislocation and reduction technique
Reading File
Finding Sources
Searching the Web
anterior shoulder dislocation anatomy reduction techniques diagram
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Searching the Web
anterior shoulder dislocation subcoracoid position X-ray clinical appearance diagram
Loading Image
Loading Image
I have excellent visual and textbook material. Now I'll compile the full response.
Anterior Shoulder Dislocation: Anatomy, Clinical Presentation & Reduction Techniques
Anatomy of the Glenohumeral Joint
The shoulder (glenohumeral) joint is a ball-and-socket joint designed for maximum range of motion at the cost of inherent bony stability. The humeral head articulates with the shallow glenoid fossa, which covers only about 1/3 of the humeral head surface. Stability depends on:
- Static stabilizers: Glenohumeral ligaments (superior, middle, inferior), the glenoid labrum, and the joint capsule
- Dynamic stabilizers: Rotator cuff muscles (supraspinatus, infraspinatus, subscapularis, teres minor)
- The coracoacromial arch (coracoacromial ligament + acromion + coracoid process) limits superior displacement
The capsule is reinforced anteriorly by the glenohumeral ligaments but is relatively thin and unsupported inferiorly - the axillary recess. This is why the vast majority of dislocations go anteriorly and inferiorly.
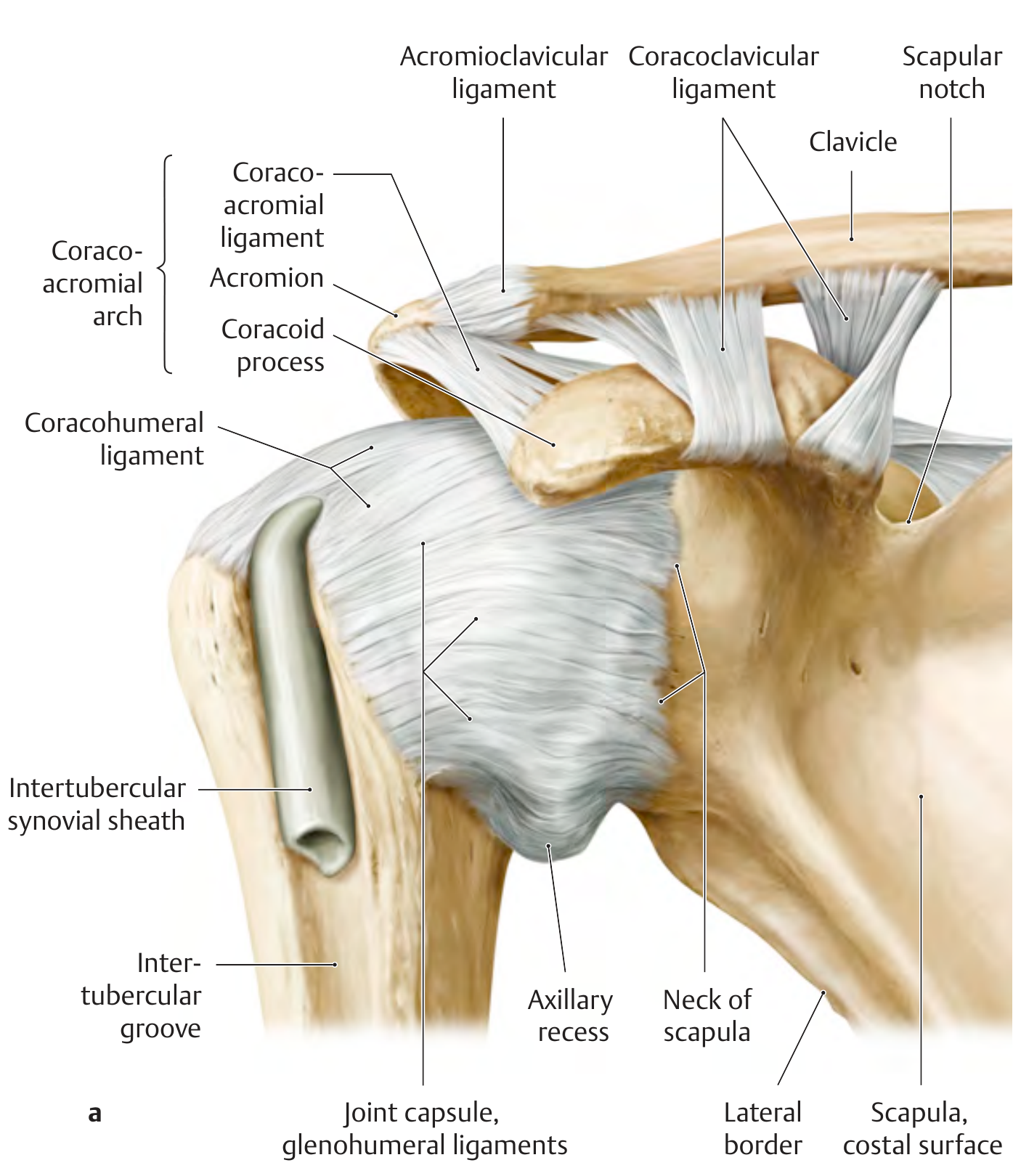
Anterior view of the right glenohumeral joint - note the glenohumeral ligaments anteriorly, axillary recess inferiorly, and the coracoacromial arch superiorly (THIEME Atlas of Anatomy)
What Is Anterior Shoulder Dislocation?
Anterior dislocations account for ~95-98% of all shoulder dislocations. The humeral head is forced anteriorly and medially out of the glenoid fossa, typically coming to rest just below the coracoid process - a subcoracoid dislocation (~75% of cases).
Four Subtypes by Position

| Subtype | Position of Humeral Head | Frequency |
|---|---|---|
| Subcoracoid | Below the coracoid, anterior to glenoid | ~75% |
| Subglenoid | Below the glenoid fossa | ~20% |
| Subclavicular | Below the clavicle, medial to coracoid | Rare |
| Intrathoracic | Between ribs and thoracic cage | Very rare |
Mechanism of Injury
The classic mechanism is forced abduction + external rotation + extension - for example, a fall on an outstretched arm or a blocking/tackling injury. This levers the humeral head over the anterior-inferior glenoid rim, tearing the anterior capsule and often the labrum (Bankart lesion). The impaction of the posterolateral humeral head against the glenoid rim creates a Hill-Sachs lesion.
Clinical Presentation
| Feature | Description |
|---|---|
| Arm position | Held in slight abduction and external rotation, supported by the other arm |
| Shoulder contour | Flattened deltoid; squared-off appearance instead of normal rounded contour |
| Humeral head | Palpable anteriorly under the clavicle/coracoid region |
| Pseudo-lengthening | Arm appears slightly longer |
| Restricted ROM | Especially internal rotation and adduction are impossible |
X-ray Appearance (AP view)
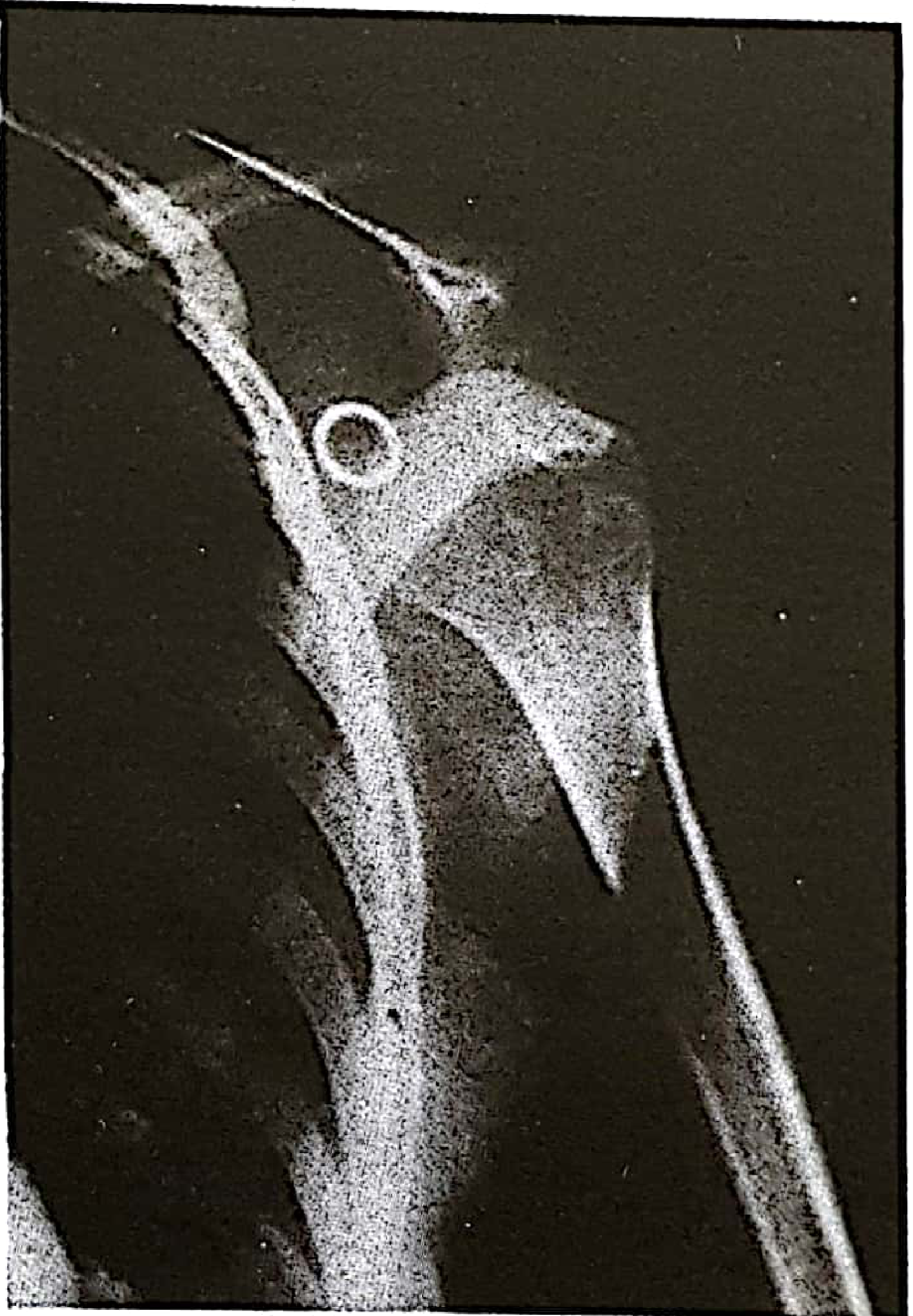
Figure 14.17: A typical anterior (subcoracoid) dislocation - Pye's Surgical Handicraft, 22nd ed.
On X-ray: the humeral head lies anterior, medial, and inferior to the glenoid. Always obtain a Y-scapular view or axillary view to confirm and rule out fracture.
Associated Injuries to Check Before Reduction
- Axillary nerve injury - Most common nerve injury (~10-20%). Test: sensation over lateral deltoid ("regimental badge" area). Paralysis of deltoid results.
- Rotator cuff tear - Especially in patients >40 years; supraspinatus most at risk.
- Bankart lesion - Anterior-inferior labral tear (most common soft tissue injury, predisposes to recurrence).
- Hill-Sachs lesion - Posterolateral humeral head compression fracture from impaction.
- Greater tuberosity fracture - Seen in ~15% of anterior dislocations.
- Axillary artery injury - Rare but life-threatening; suspect if absent radial pulse.
Pre-Reduction Assessment
Before any reduction attempt:
- AP + axillary (or Y-scapular) X-rays to confirm direction and rule out fracture-dislocation
- Full neurovascular exam (axillary nerve, radial pulse)
- Analgesia/sedation - essential for muscle relaxation, which is key to success
- Exclude contraindications: fracture-dislocation (particularly neck of humerus fractures), vascular injury
Reduction Techniques
Most reduction techniques work by relaxing the spasmed shoulder muscles and then guiding the humeral head back over the glenoid rim. Adequate analgesia is the most important factor for success.
1. Stimson Maneuver (Gravity-Assisted)
Position: Patient prone at the edge of the stretcher, affected arm hanging down.
Technique: Attach 5 kg (10 lb) weights to the wrist. Allow 20-30 minutes for gravity to fatigue the muscles. The shoulder often reduces spontaneously. Adding gentle external/internal rotation or scapular manipulation speeds reduction.
- Pros: Minimal force, excellent for elderly or anxious patients, very low complication risk
- Cons: Requires patient cooperation, takes time, not suitable for agitated patients
2. Scapular Manipulation
Position: Patient prone (as per Stimson) or seated.
Technique: Apply traction to the arm (or use weights). Then use your thumbs to rotate the inferior tip of the scapula medially and dorsally toward the spine. This repositions the glenoid to face the dislocated humeral head.
- Pros: Low force needed, high success rate on first attempt, well tolerated
- Cons: Requires assistant for traction in the seated position
3. External Rotation Technique (Hennepin / Minh)
Position: Patient seated or supine.
Technique:
- Fully adduct the arm to the patient's side
- Flex the elbow to 90 degrees
- Using the forearm as a lever, slowly and gently rotate the arm externally - 1 degree every few seconds
- Pause if patient feels pain - wait for muscle relaxation before continuing
- Continue until forearm is lying flat on the stretcher
- No traction is applied
- Pros: Requires only one operator, minimal force, excellent success rate (~80-90%), minimal sedation needed
- Cons: Slow process; requires patience
4. Milch Technique
Position: Patient supine.
Technique:
- Abduct and externally rotate the arm overhead until it is fully overhead (like raising your arm to ask a question)
- Apply gentle longitudinal traction with slight external rotation
- If not reducing, push the humeral head upward toward the glenoid with the thumb

Left: Milch method (abduction, external rotation, upward push). Right: Kocher method (now largely abandoned due to fracture risk)
- Pros: Single operator, gentle
- Cons: Full overhead abduction uncomfortable in acute setting
5. Traction-Countertraction Method
Position: Patient supine.
Technique:
- Wrap a sheet under the patient's axilla and around an assistant's waist - assistant leans back to provide countertraction
- Wrap a second sheet around the patient's flexed forearm and around your own waist
- Elevate the bed until the sheet sits at your ischial tuberosities
- Lean back using body weight (not bicep strength) for sustained, steady traction
- After traction is established, gently adduct the arm; a second assistant can apply lateral traction to the humerus
- Pros: Very high success rate, widely familiar, reliable
- Cons: Requires 2+ operators, some force needed, uncomfortable for patient, operator fatigue possible; generally requires procedural sedation
"A 2014 comparison study found modified scapular manipulation was better tolerated and had better first-attempt success; traction-countertraction was more successful on second attempt." - Roberts & Hedges' Clinical Procedures in Emergency Medicine
6. Spaso Technique
Position: Patient supine.
Technique: Grasp the wrist of the affected arm and gently lift it vertically toward the ceiling while applying gentle vertical traction. An assistant provides countertraction at the chest. Add gentle external rotation during the procedure.
- Pros: Simple, single operator, good for less muscular patients
- Cons: Less familiar technique
7. Cunningham Technique (No Sedation Needed)
Position: Patient seated, affected arm fully adducted, elbow flexed 90 degrees.
Technique: The physician massages the trapezius, deltoid, and biceps to encourage muscular relaxation. The patient is coached to relax - reduction occurs passively as the muscles let go.
- Pros: No sedation required, no force, no assistant, very safe
- Cons: Requires patient cooperation; less reliable in acute high-pain situations
Technique Comparison Summary
| Technique | Operators Needed | Sedation | Force Required | Notes |
|---|---|---|---|---|
| Stimson (gravity) | 1 | Minimal | None | Best for relaxed/elderly patients |
| Scapular manipulation | 1-2 | Minimal | Minimal | High first-attempt success |
| External rotation | 1 | Minimal | None | Excellent for ED use |
| Milch | 1 | Minimal | Minimal | Overhead abduction required |
| Traction-countertraction | 2-3 | Required | Moderate | ED standard; high 2nd attempt success |
| Spaso | 1-2 | Minimal | Minimal | Supine technique |
| Cunningham | 1 | None | None | Muscle relaxation focused |
| 1 | - | High | Abandoned - high fracture/NV injury risk | |
| 1 | - | High | Abandoned - axillary vessel injury risk |
Post-Reduction Care
- Confirm reduction with post-reduction AP + axillary X-ray
- Repeat neurovascular exam (axillary nerve, radial pulse)
- Immobilize in a sling for 1-4 weeks (duration controversial; shorter immobilization gaining favor)
- Physiotherapy early to restore rotator cuff strength
- Recurrence risk: Very high in young patients (<20 years: up to 90% recurrence). Consider surgical stabilization (Bankart repair) after first dislocation in young, active patients.
Sources:
- Roberts and Hedges' Clinical Procedures in Emergency Medicine (procedures, technique descriptions)
- Pye's Surgical Handicraft, 22nd ed. (clinical presentation, management)
- THIEME Atlas of General Anatomy and Musculoskeletal System (glenohumeral anatomy, ligaments)
- Merck Manual - Shoulder Reduction Overview
- PMC Systematic Guide to Shoulder Reduction
This is a shared conversation. Sign in to Orris to start your own chat.