Why are vericose veins More common in the lower limb than in the upper limb? Explain with anatomical and physiological reasons
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Searching the Web
why varicose veins more common lower limb than upper limb anatomical physiological reasons
I have all the information needed from multiple authoritative textbooks. Let me now compose a comprehensive, well-structured answer.
Why Varicose Veins Are More Common in the Lower Limb Than the Upper Limb
Varicose veins - dilated, tortuous, elongated veins - are almost exclusively a disease of the lower limbs. This is not a coincidence; it is the direct result of a unique combination of anatomical architecture and physiological demands that the lower limb venous system faces, none of which apply to the upper limb to the same degree.
1. Hydrostatic Pressure: The Fundamental Driving Force
The single most important reason is hydrostatic pressure from the column of blood in the upright posture.
In the standing adult, the venous pressure in the foot equals the vertical distance from the foot to the right atrium - approximately 70-90 mmHg (equivalent to 90-120 cm H₂O). This is a direct consequence of gravity acting on the unbroken column of blood from heart to foot.
"Were it not for valves in the veins, the gravitational pressure effect would cause the venous pressure in the feet always to be about +90 mm Hg in a standing adult."
- Guyton and Hall Textbook of Medical Physiology
The upper limb, by contrast, is not a dependent limb in the erect posture. In most activities and rest positions, the arms are at or above heart level for significant portions of the day. Even when the arm hangs down, the vertical height from hand to heart is only ~40-50 cm, generating far less hydrostatic pressure than the 120+ cm of the lower limb column.
This sustained, high hydrostatic pressure in the lower limb veins:
- Chronically distends vein walls
- Subjects valve leaflets to enormous back-pressure
- Eventually causes valve incompetence and venous dilation
2. The Venous Valve System and Its Vulnerability
Lower limb veins have a complex three-tier valve system that must work against gravity
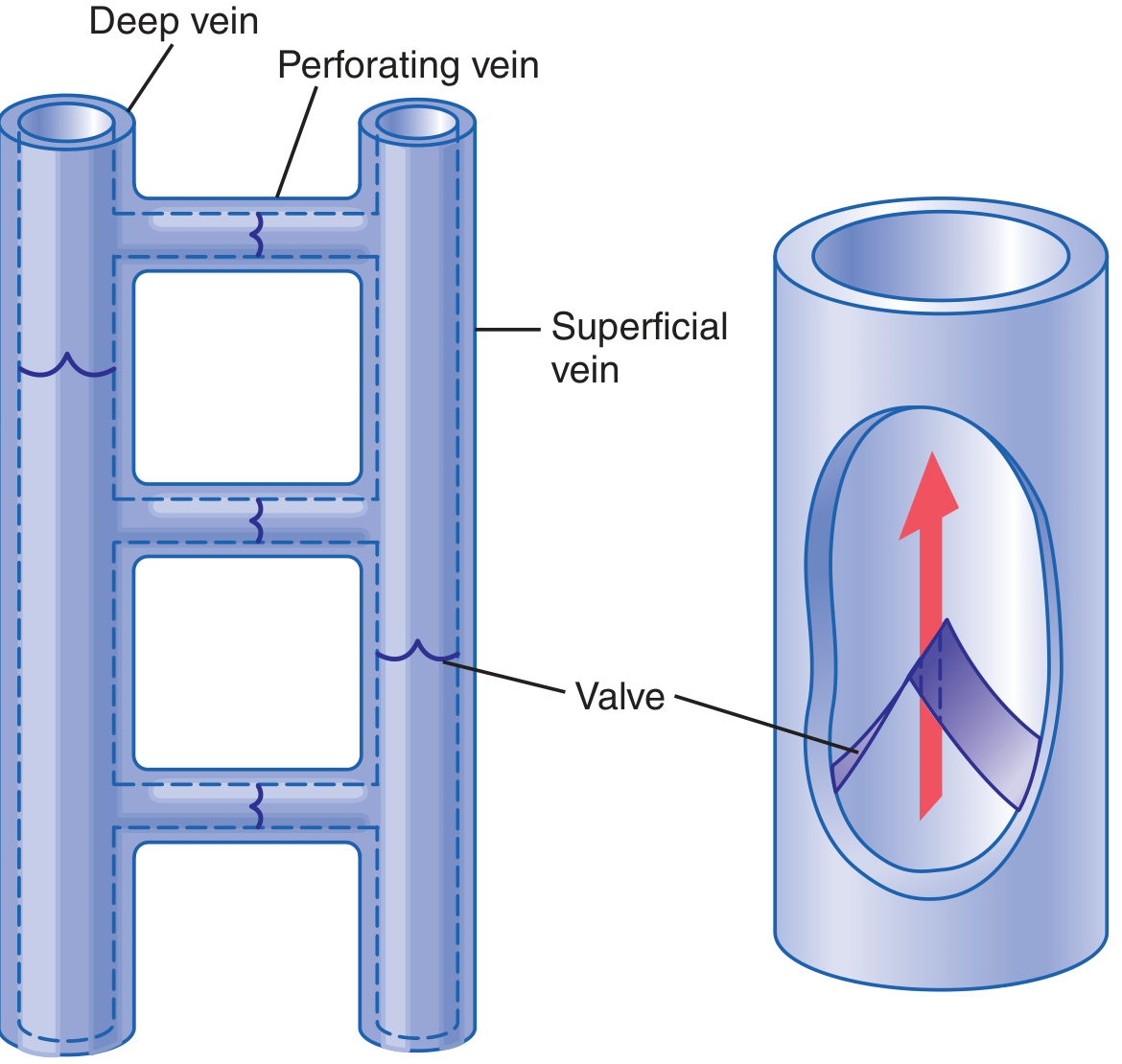
The lower limb venous drainage is organized into three interconnected compartments:
- Deep veins (femoral, popliteal, tibial) - carry ~90% of venous return
- Superficial veins (great saphenous vein, small saphenous vein)
- Perforating (communicating) veins - connect superficial to deep
Valves in these systems are arranged so blood flows only toward the heart. The perforating vein valves specifically direct blood from superficial to deep during calf muscle contraction.
Upper limb veins face much less valvular stress
The basilic and cephalic veins of the upper limb do contain valves, but they are not subjected to the same continuous gravitational load. The column height is shorter, hydrostatic pressure is lower, and the arm muscles' activity is more variable - not dominated by weight-bearing, which loads the lower limb valves all day long.
3. The Calf Muscle Pump: A Critical But Failible Mechanism
The lower limb has a specialized physiological mechanism - the calf muscle pump (venous pump) - that actively propels blood upward against gravity. The gastrocnemius and soleal sinuses act like a bellows:
- During calf muscle contraction: pressures of 150-300 cm H₂O are generated, compressing deep veins and propelling blood proximally. Perforating vein valves close to prevent pressure transmission to superficial veins.
- During relaxation: pressure drops, and blood refills the deep veins from the superficial system through the perforators.
"The veins of the lower limb carry blood against the force of gravity back to the heart... when the muscles of the calf contract, they compress the soleal sinuses and the deep veins encased in fascia and muscle, achieving a pressure of up to 300 cm H₂O."
- Pfenninger and Fowler's Procedures for Primary Care
When a person stands perfectly still, the calf pump does not work, and venous pressure in the lower legs rises to the full gravitational value of ~90 mmHg in just 30 seconds. This is why prolonged standing is a major risk factor for varicose veins.
The upper limb has no comparable high-pressure dependent-limb pump requirement. Arm veins drain efficiently even with minimal muscular assistance.
4. How Valve Failure Causes Varicose Veins: The Cascade
When lower limb veins are chronically overstretched (pregnancy, prolonged standing, obesity, thrombosis), the vein diameter increases. The valve leaflets, however, do not grow proportionally. The result: leaflets fail to coapt and the valve becomes incompetent.
"Stretching the veins increases their cross-sectional areas, but the leaflets of the valves do not increase in size. Therefore, the leaflets of the valves no longer close completely. With this lack of complete closure, the pressure in the veins of the legs increases greatly because of failure of the venous pump, which further increases the sizes of the veins and finally destroys the function of the valves entirely."
- Guyton and Hall Textbook of Medical Physiology
Once a proximal valve (e.g., saphenofemoral junction) becomes incompetent, the blood column refluxes downward, placing even greater pressure on the next valve distally. This cascade of progressive valvular incompetence is unique to the lower limb because the gravitational force continuously drives blood downward.
Typical sites of valvular incompetence in the lower limb:
- Saphenofemoral junction (most common)
- Midthigh perforating veins
- Calf perforators (5, 10, 15 cm above the medial malleolus)
- Saphenopopliteal junction
5. Anatomical Differences: Superficial Vein Exposure
The great saphenous vein and small saphenous vein are embedded in the subcutaneous fat with comparatively little fascial support - they are not encased in tight muscular compartments. This means:
- High pressures generated during calf muscle contraction are transmitted to the superficial system when perforating vein valves fail
- There is no external mechanical support to resist dilation
- The superficial location makes dilated veins visible
The upper limb superficial veins (cephalic, basilic) are similarly superficial, but they never experience the magnitude of hydrostatic pressure or the same transmural pressure differentials.
6. Additional Contributing Factors Specific to the Lower Limb
| Factor | Lower Limb | Upper Limb |
|---|---|---|
| Hydrostatic column height | ~90-120 cm (heart to foot) | ~40-50 cm (heart to hand) |
| Weight-bearing/prolonged standing | Yes - daily activity | No |
| Dependency during rest | Commonly dependent | Usually elevated/horizontal |
| Hormonal effects (progesterone) | Causes smooth muscle relaxation + venous dilation; also outflow obstruction from uterus during pregnancy | Not affected by uterine compression |
| Deep vein thrombosis risk | High (DVT destroys valves on recanalization) | Much lower incidence |
| Erect posture penalty | Full gravitational load | Partial |
As S Das notes, varicose veins of the lower limb appear to be "a part of penalty of erect posture which the human beings have adopted" - a condition unique to bipedalism, not seen in quadrupedal animals (S Das - A Manual on Clinical Surgery, 13th Edition).
Summary
Varicose veins are predominantly a lower limb condition because:
- Hydrostatic pressure is 2-3x greater in the lower limb due to the long vertical column of blood in the upright posture
- Valves must work against constant gravity - they fail when chronically overstretched, and the lower limb valves carry this burden all day
- The calf muscle pump is an essential but fallible mechanism - when it fails or is inactive (prolonged standing), venous pressure soars
- Cascade of valve incompetence: once one valve fails, reflux overloads the next, progressively destroying the entire system downward
- Perforating vein valve failure transmits high deep compartment pressures (up to 300 cm H₂O during exercise) directly to the unsupported superficial veins
- Pregnancy and hormonal factors selectively affect the lower limb outflow and venous wall tone
- The upper limb simply does not experience the same combination of gravitational load, venous column height, and repeated pressure cycling that makes lower limb valves vulnerable
Sources: Guyton and Hall Textbook of Medical Physiology; Gray's Anatomy for Students; Sabiston Textbook of Surgery; Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed.; S Das - A Manual on Clinical Surgery, 13th Edition
This is a shared conversation. Sign in to Orris to start your own chat.