44 year old lady presented with complaints of intermittent pain in right lower abdomen. She gives history of laparoscopic ovarian cystectomy 1 and half years back, which was reported as serous cystadenoma right ovary and endometriotic cyst left ovary. now, on examination pelvic mass present.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
recurrent ovarian cyst after cystectomy serous endometrioma management
Loading Image
Loading Image
Excellent - I now have comprehensive content from the textbooks. Let me put together a thorough clinical analysis.
Clinical Analysis: 44-Year-Old with Recurrent Pelvic Mass After Ovarian Cystectomy
Summary of the Clinical Scenario
This patient has a bilaterally complex history: right serous cystadenoma (benign epithelial tumor) and left endometriotic cyst (endometrioma), both treated by laparoscopic cystectomy 18 months ago. She now returns with right lower abdominal pain and a pelvic mass on examination. This is a diagnostically important situation because the nature of the recurrent mass - benign recurrence vs. borderline vs. frank malignancy - determines management entirely.
Step 1: Differential Diagnosis of the Current Pelvic Mass
Given her history, the differential has four main possibilities, in order of likelihood:
1. Recurrent Endometrioma (left, or bilateral)
The most common cause of recurrent pelvic mass after conservative surgery for endometriosis.
- Conservative surgery carries high recurrence rates: 2-20% per year, with cumulative rates of 4-25% at 2 years and up to 40% at 5 years (Berek & Novak's Gynecology, p. 684)
- Risk factors that apply here: previous surgery (the strongest predictor), young age at diagnosis, and left-sided involvement (left-sided disease has a higher recurrence risk than right-sided disease)
- She also had an endometrioma on the left specifically, and the literature notes left-sided endometriosis has a higher recurrence probability
2. Recurrent / Residual Serous Tumor - Benign or Borderline
Serous cystadenomas may recur after cystectomy if excision was incomplete. More importantly:
- 5-10% of serous tumors have borderline malignant potential, and 20-25% are malignant - Berek & Novak's Gynecology, p. 454
- A borderline tumor cannot be distinguished from benign on gross examination alone - frozen section is required
- Borderline serous tumors may recur after many years; 5-year survival is not synonymous with cure for borderline tumors - Robbins & Cotran, p. 943
- At 44 years of age, the risk of epithelial tumors increases, making this possibility more significant than it would have been in a younger woman
3. De Novo Ovarian Neoplasm (New Primary Tumor)
Either side may develop a new primary mass independent of the previous pathology:
- New endometrioma on the right (her previously operated side)
- New epithelial ovarian neoplasm
- Endometriosis can transform into endometrioid carcinoma or clear cell carcinoma - this is a well-recognized though uncommon malignant transformation of endometriosis
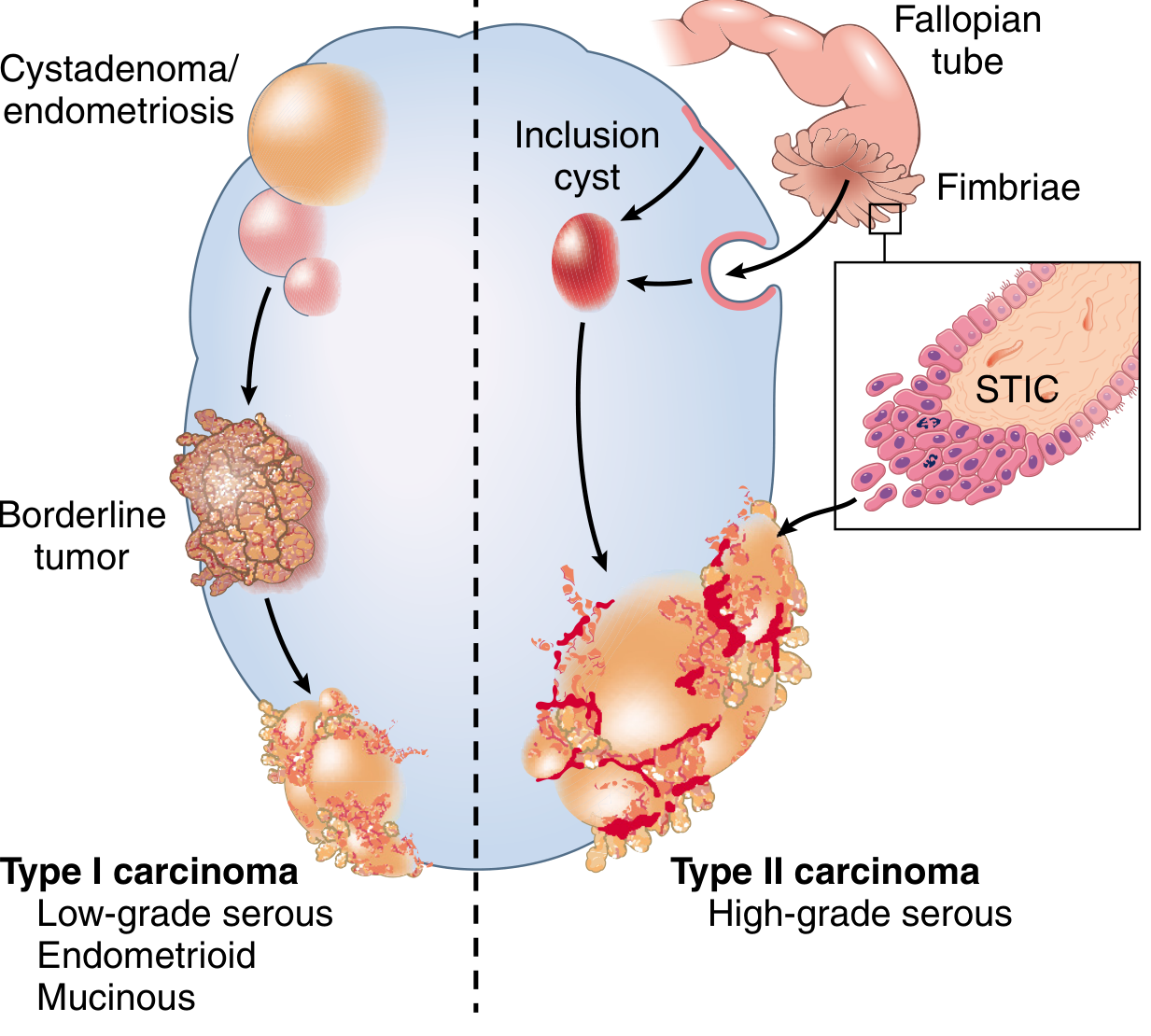
4. Malignant Transformation / Ovarian Cancer
- Must be ruled out at this age with a new pelvic mass
- The WHO classification places serous cystadenoma in the same lineage as serous cystadenocarcinoma (Type I pathway: cystadenoma → borderline tumor → low-grade serous carcinoma)
Step 2: Histological Spectrum of Serous Tumors (Key Point for This Patient)
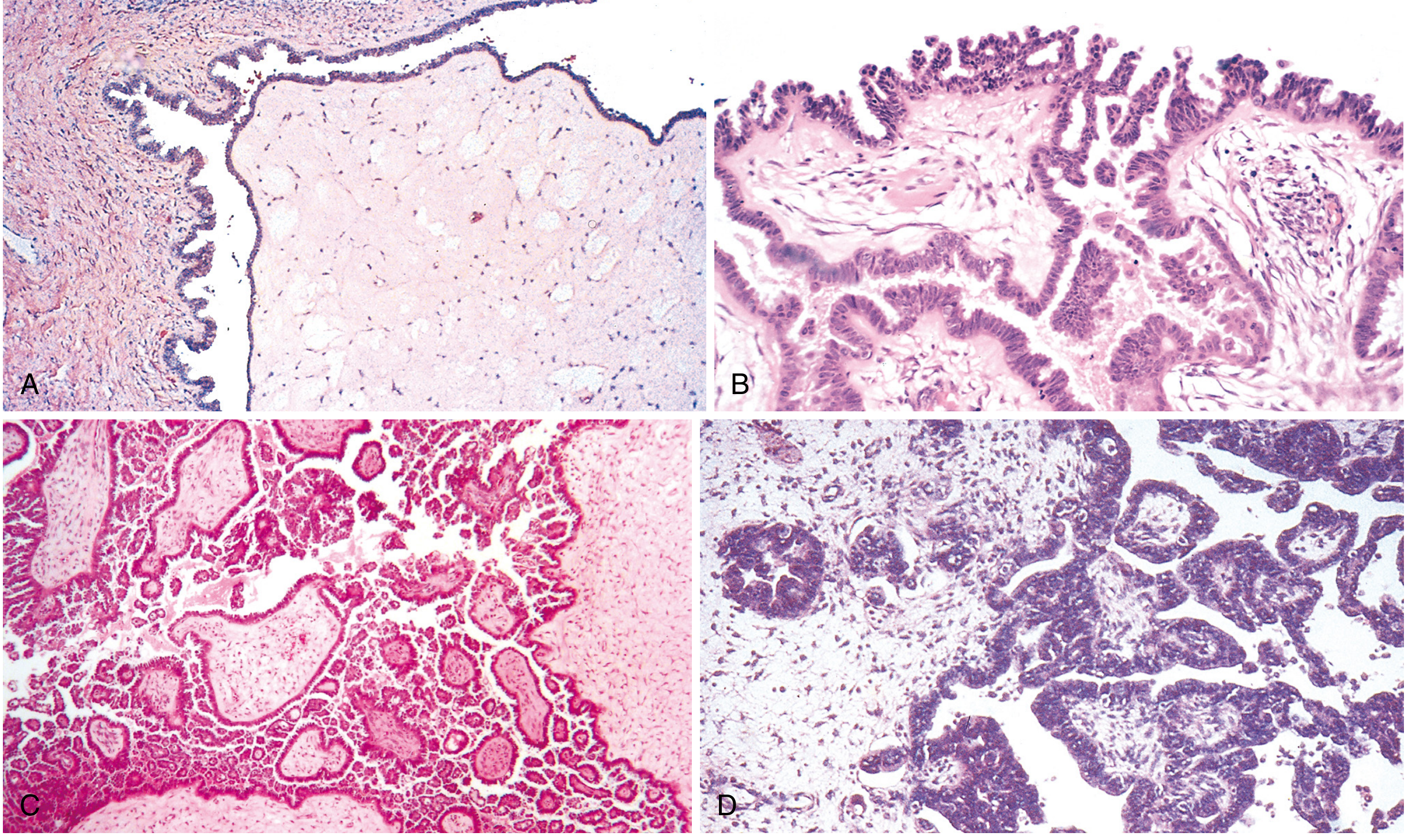
The spectrum from A to D above shows why frozen section and histologic confirmation are mandatory for any recurrent mass in this patient.
Step 3: Workup (Recommended Approach)
History & Examination
- Character of pain: cyclical (suggests endometrioma) vs. constant (malignancy concern)
- Menstrual changes, dysmenorrhea, dyspareunia
- Weight loss, anorexia (red flag symptoms)
- Family history of BRCA1/2, breast/ovarian cancer, Lynch syndrome
Investigations
| Investigation | Purpose |
|---|---|
| Transvaginal + transabdominal ultrasound | First-line; assess cyst characteristics |
| CA-125 | Elevated in endometriosis AND ovarian cancer; high sensitivity but low specificity; useful for trend monitoring |
| CEA, CA 19-9 | Rule out mucinous primary or metastatic GI tumor to ovary |
| HE4 (Human Epididymis Protein 4) | More specific than CA-125 for malignancy; ROMA score calculation |
| MRI pelvis | Best for characterizing pelvic masses; differentiates endometrioma (T1 high, T2 shading) from other lesions |
| CT abdomen-pelvis | If malignancy suspected - assess for peritoneal disease, lymphadenopathy, omental deposits |
| BRCA1/2 testing | Given she now has a second pelvic mass at 44 |
Ultrasound Features Concerning for Malignancy (from Berek & Novak's):
- Multiloculations
- Cyst size > 10 cm
- Solid components or papillary projections
- Thick septations
- Irregular walls/nodularity
- Ascites
- Bilateral masses
- Abnormal color Doppler flow (low-resistance pattern)
A simple cyst up to 10 cm is likely benign and can be managed expectantly if asymptomatic - Berek & Novak's, p. 465.
Step 4: Management Algorithm
New pelvic mass post-cystectomy
↓
Clinical + Imaging (TVS + MRI) + Tumor markers
↓
┌─────────────────────────────┐
│ │
Likely benign features Suspicious/malignant features
(simple cyst, CA-125 low) (solid components, ascites,
elevated markers, large size)
↓ ↓
Expectant management Prompt surgical evaluation
(if asymptomatic, <10cm) by gynecologic oncologist
↓
Symptomatic / growing
↓
Laparoscopic cystectomy
(fertility-sparing preferred)
with INTRAOPERATIVE FROZEN SECTION
↓
┌──────────────────────────────────────┐
│ │
Benign Borderline/Malignant
↓ ↓
Cystectomy adequate; Staging laparotomy / full
postop OCP/GnRH agonist surgical staging (TAH+BSO
to prevent endometriosis + omentectomy + lymphadenectomy)
recurrence
Key surgical principle: The current recommendation is laparoscopic management of suspected benign adnexal masses, even those >10 cm. Intraoperative rupture rates are similar to open surgery, and laparoscopy offers decreased operative time, hospital stay, and morbidity - Berek & Novak's, p. 466.
Step 5: Specific Concerns in This Patient
Regarding the Right Side (Previous Serous Cystadenoma)
- Any new mass on the right must rule out borderline or malignant transformation - a frozen section at the time of any re-operation is non-negotiable
- Serous borderline tumors can recur years after initial surgery; 5-year survival ≠ cure
- Low-grade serous carcinomas (Type I pathway) carry KRAS/BRAF mutations and progress slowly
Regarding the Left Side (Previous Endometrioma)
- High risk of recurrence: overall endometriosis recurrence up to 40% at 5 years
- Prevention of recurrence: After conservative surgery, OCP use significantly reduces endometrioma recurrence. One study showed recurrence in only 10% of OCP users vs. 40% of non-users (OR 0.16; 95% CI 0.04-0.65) - Berek & Novak's, p. 685
- Medical treatment of recurrence is an option before repeat surgery in symptomatic endometriosis (GnRH agonists, dienogest, OCP)
- Endometriosis can undergo malignant transformation to endometrioid or clear cell carcinoma - this should be kept in mind at 44 years
Age Consideration (44 years)
- She is approaching perimenopause; if she has completed her family, a discussion about definitive surgery (bilateral salpingo-oophorectomy) is appropriate, especially if a second laparoscopic cystectomy is being planned
- Repeat conservative surgery for endometriosis is associated with diminishing returns and increasing adhesion risk
Prevention of Recurrence (Post-Operative)
For endometriosis specifically - Berek & Novak's Gynecology (p. 685):
- Women should seek conception promptly if desired, OR
- Use oral contraceptive pills (cyclic or continuous) until pregnancy is desired
- Postoperative long-term OCP (24 months) significantly reduces recurrence vs. no treatment
- GnRH agonists with add-back therapy for patients who cannot tolerate OCP
Bottom Line
This 44-year-old woman with a new pelvic mass after bilateral ovarian cystectomy (serous cystadenoma right + endometrioma left) requires:
- Transvaginal ultrasound + MRI pelvis as the primary imaging
- CA-125, HE4, ROMA score for malignancy risk stratification
- Surgical intervention is indicated given she is symptomatic (pain) with a palpable mass
- Laparoscopic re-exploration with frozen section - this is the standard approach
- The most important concern at this age is ruling out a serous borderline tumor or low-grade serous carcinoma from the right ovary, and endometrioma recurrence or malignant transformation from the left
- If repeat cystectomy is chosen, discuss definitive surgery as an alternative given her age and bilateral disease history
- Postoperative suppressive therapy (OCP or GnRH agonist) regardless of outcome to prevent further endometriosis recurrence
Sources: Berek & Novak's Gynecology, pp. 454-466, 684-685; Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 941-943
This is a shared conversation. Sign in to Orris to start your own chat.