Pudendal Neuralgia
Reading File
Finding Sources
Finding Sources
Searching PubMed
pudendal neuralgia diagnosis treatment
Reading File
Finding Sources
Reading Article
PMID: 39607531
Reading Article
PMID: 38942945
Reading File
Reading File
Reading Article
PMID: 38797289
Reading File
Searching Images
pudendal nerve anatomy Alcock canal entrapment
I now have comprehensive information. Let me compile a thorough response on pudendal neuralgia.
Pudendal Neuralgia
Pudendal neuralgia (PN) is a chronic neuropathic pain syndrome affecting the distribution of the pudendal nerve (S2–S4), most commonly caused by nerve entrapment or injury. It is frequently underdiagnosed and can be profoundly debilitating.
Anatomy
The pudendal nerve arises from the sacral plexus (S2, S3, S4). Its course makes it vulnerable to entrapment at several points:
- Exits the pelvis through the greater sciatic foramen (below piriformis)
- Wraps around the ischial spine and posterior sacrospinous ligament
- Re-enters the pelvis through the lesser sciatic foramen
- Travels through the pudendal canal (Alcock's canal) — a fascial tunnel on the medial aspect of the obturator internus muscle — where it divides into its three terminal branches:
- Inferior rectal nerve (anal canal, external sphincter, perianal skin)
- Perineal nerve (scrotum/labia, perineal muscles, urogenital diaphragm)
- Dorsal nerve of the clitoris/penis
The most common entrapment sites are between the sacrospinous and sacrotuberous ligaments and within Alcock's canal.
MR Neurography of Pudendal Neuropathy
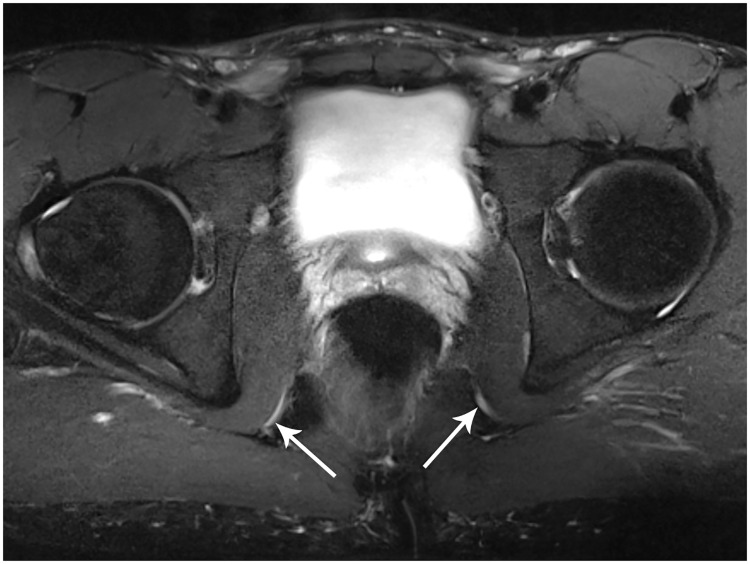
Axial 3T MR neurography (T2 fat-suppressed): bilateral pudendal nerve hyperintensity and enlargement within the pudendal (Alcock's) canals — hallmark of pudendal neuropathy/entrapment.
Etiology & Risk Factors
| Category | Examples |
|---|---|
| Mechanical/compressive | Prolonged cycling, horseback riding, prolonged sitting |
| Surgical/iatrogenic | Sacrospinous ligament fixation, lateral mesh procedures, episiotomy, Bartholin gland excision |
| Obstetric | Vaginal delivery (stretching, prolonged 2nd stage) |
| Traumatic | Pelvic fracture, motor vehicle accident |
| Functional | Chronic constipation, pelvic floor hypertonia, perineal descent syndrome |
| Vascular | Pelvic varicosities compressing the nerve |
Pudendal neuropathy from perineal descent syndrome is caused by stretching and entrapment of the nerve, evidenced by elongation, prolonged pudendal nerve motor terminal latency (PNTML), and decreased anal sensation. — Berek & Novak's Gynecology
Clinical Features
Pain characteristics:
- Burning, sharp, aching, or electric shock-like pain
- Paresthesia/numbness in perineum, vulva/scrotum, clitoris/penis, perianal region, distal urethra
- Typically unilateral (though bilateral occurs)
- Allodynia — pain from non-painful stimuli (e.g., clothing contact)
Key symptom patterns:
- Pain worsened by sitting (classically, sitting on a toilet is less painful than a hard chair — the central perineum is unloaded)
- Pain relieved by standing or lying down
- Pain does not wake the patient from sleep (a distinguishing feature)
- Exacerbated by hip flexion, exercise, straining
- Associated urinary symptoms: urgency, frequency, dysuria
- Sexual dysfunction: dyspareunia, ejaculatory pain, erectile dysfunction
Diagnosis: Nantes Criteria
The Nantes criteria are the internationally recognized diagnostic framework for pudendal nerve entrapment (PNE):
| Criterion | Description |
|---|---|
| 1 | Pain in the S2–S4 dermatomal area (clitoris/penis, distal urethra, labia/scrotum, perineum, anus) |
| 2 | Pain increased while sitting |
| 3 | Patient is not awakened by pain at night |
| 4 | No objective sensory loss on clinical examination (sensory deficit suggests sacral root lesion, not entrapment) |
| 5 | Resolution of pain with pudendal nerve block (diagnostic and therapeutic) |
"It is not possible with examination or imaging to completely differentiate pudendal entrapment from neuralgia related to nerve injury." — Berek & Novak's Gynecology, p. 596
Examination Findings
- Maximum tenderness near the ischial spine and Alcock's canal on vaginal/rectal palpation
- Confirmatory diagnostic nerve block: 3–5 mL of 0.25% bupivacaine at ischial spine; ≥50% relief is diagnostic
Electrodiagnostics
- Pudendal nerve motor terminal latency (PNTML): prolonged in entrapment/stretch injury
- Limited sensitivity; normal PNTML does not exclude PN
Imaging
- MR neurography (3T): emerging gold standard — detects T2 hyperintensity and nerve enlargement in Alcock's canal; also useful for pre-surgical planning
- DTI tractography: allows 3D mapping of nerve course; a 2024 systematic review (PMID 38797289) found DTI of the lumbosacral plexus is feasible and may offer prognostic and preoperative value, though normative values for pudendal nerve microstructure are not yet established
- CT/MRI: exclude structural causes (tumors, cysts, sacral lesions)
Management
Management is multimodal and stepped. No single treatment has proven superiority.
Conservative (First-Line)
| Intervention | Details |
|---|---|
| Behavioral/activity modification | Avoid prolonged sitting, use perineal cutout cushions, stop cycling |
| Pelvic floor physiotherapy | Address hypertonia, trigger points, myofascial dysfunction |
| Pharmacotherapy | TCAs (amitriptyline), SNRIs (duloxetine), gabapentinoids (gabapentin, pregabalin), topical lidocaine/amitriptyline |
| Cognitive-behavioral therapy | Pain psychology; especially for central sensitization component |
Interventional (Second-Line)
Pudendal nerve blocks:
- CT- or ultrasound-guided injection at ischial spine or within Alcock's canal
- Local anesthetic ± corticosteroid
- Both diagnostic and therapeutic
- Campbell-Walsh Wein notes: "pudendal nerve blocks applied by trained clinicians may be helpful therapy and can also aid in diagnosis" in pelvic pain conditions
Pulsed radiofrequency (PRF):
- Applied to pudendal nerve; neuromodulatory rather than ablative
- A 2025 meta-analysis (PMID 39607531) found PRF, injections, and surgery all improved pain to a similar extent (mean VAS reduction ~2.73 cm), with no statistically significant difference between modalities
Electrical stimulation / neuromodulation:
- Sacral neuromodulation (S3 stimulation), posterior tibial nerve stimulation, and direct pudendal nerve stimulation
- A 2024 systematic review (PMID 38365090) supports electrical stimulation as a viable option
Surgical (Third-Line)
Indicated for true entrapment (not pure nerve injury). Three main approaches:
| Technique | Route | Success Rate (meta-analysis) |
|---|---|---|
| Laparoscopic transperitoneal | Minimally invasive, direct visualization | ~91% (95% CI 0.64–0.98) |
| Perineal | Via perineal incision | ~69% (95% CI 0.52–0.82) |
| Transgluteal | Via gluteal incision | ~50% (95% CI 0.37–0.63) |
A 2024 meta-analysis (810 patients, 19 studies) found overall surgical pain relief in 67% of patients, with the laparoscopic approach appearing most promising (PMID 38942945). Complication rate for laparoscopic approach was 16%.
Key caveat: Surgery benefits entrapment — not pure nerve injury. Since these cannot be fully distinguished clinically, appropriate patient selection is critical.
Differential Diagnosis
- Vulvodynia / vestibulodynia (no nerve block response)
- Coccydynia
- Interstitial cystitis/bladder pain syndrome
- Levator ani syndrome / pelvic floor myofascial pain
- Piriformis syndrome
- Sacral nerve root compression (radiculopathy — would show sensory deficits, distinguishing it from PN)
- Prostatitis / chronic pelvic pain syndrome (men)
- Pelvic congestion syndrome
Summary of Recent Evidence (2024–2025)
| Study | Finding |
|---|---|
| Andiman et al., 2025 (PMID 39607531) | All treatments (surgery, injection, PRF) reduce pain (~2.73 cm VAS); no treatment clearly superior; evidence quality is mostly Grade C |
| Mylle et al., 2024 (PMID 38942945) | Surgical decompression success ~67% overall; laparoscopic approach best (~91%) |
| Duraffourg et al., 2024 (PMID 38797289) | DTI/MR tractography feasible for pudendal nerve imaging; promising for preoperative planning |
| Giulioni et al., 2024 (PMID 38714513) | Pudendal neurolysis improves urogenital/rectal symptoms beyond pain |
Sources:
- Berek & Novak's Gynecology, pp. 595–596 (Nerve Entrapment; Nantes Criteria)
- Berek & Novak's Gynecology, p. 172 (Pudendal nerve anatomy)
- Campbell-Walsh-Wein Urology (IC/BPS and pudendal nerve blocks)
- PubMed systematic reviews: PMIDs 39607531, 38942945, 38797289, 38365090
Tp be done in a case of primary infertility with tubal block
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
tubal factor infertility treatment
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
tubal factor infertility hysterosalpingography HSG tubal occlusion
I have comprehensive information. Now I'll compose the full clinical answer on the workup and management of primary infertility with tubal block.
Primary Infertility with Tubal Block — Investigations & Management
This is a structured clinical approach covering history, investigations, and treatment options.
Step 1 — Establish the Diagnosis of Primary Infertility
Definition: Failure to conceive after 12 months of regular unprotected intercourse (or 6 months if age ≥35).
A full infertility workup must precede tubal-focused management to identify co-existing factors (male factor, ovarian reserve, uterine pathology), since tubal disease coexists with other factors in a significant proportion of couples.
Step 2 — Initial Workup (All Couples)
Female Partner
| Investigation | Purpose |
|---|---|
| Menstrual history, BMI, pelvic exam | Ovulatory status, signs of PCOS/endometriosis |
| Serum FSH, LH, AMH, antral follicle count (AFC) | Ovarian reserve assessment |
| Mid-luteal progesterone (day 21) | Confirm ovulation |
| TSH, prolactin | Rule out endocrine causes |
| Rubella immunity, STI screen | Pre-conception |
| Chlamydia antibody test (CAT) | Non-invasive screen for tubal damage — can differentiate low vs. high risk for tubal occlusion before invasive testing (ESHRE GPP) |
Male Partner
| Investigation | Purpose |
|---|---|
| Semen analysis (×2) | Male factor (accounts for ~40% of infertility) |
| If abnormal: FSH, testosterone, karyotype | Azoospermia workup |
Step 3 — Tubal Assessment
3a. Non-invasive / First-line
Chlamydia Antibody Testing (CAT)
- High titres predict tubal damage; can triage patients before imaging
- Negative CAT in a low-risk patient makes significant tubal disease less likely
3b. Tubal Patency Testing (Imaging)
Both are first-line options — choice depends on clinician/patient preference (ESHRE strong recommendation):
| Test | Details | Notes |
|---|---|---|
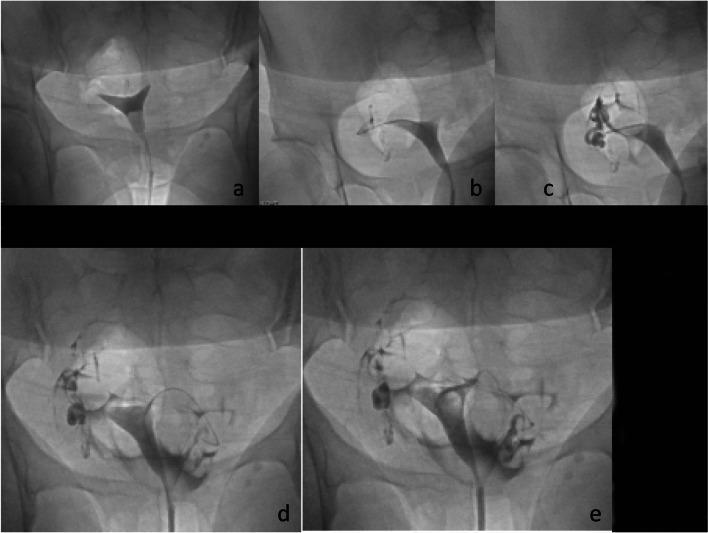
| Hysterosalpingography (HSG) | Fluoroscopic X-ray after uterine contrast injection; evaluates tubal patency + uterine cavity | Can be therapeutic (dye flush) for minor blocks |
| HyCoSy / HyFoSy | Ultrasound-based tubal patency test using saline ± foam contrast | No radiation; comparable diagnostic capacity to HSG |
| Saline Infusion Sonography (SIS) | Evaluates uterine cavity (submucous fibroids, polyps, synechiae) | Adjunct |
HSG findings in tubal block:
3c. Definitive Assessment
Diagnostic Laparoscopy + Chromopertubation
- Gold standard for tubal patency and pelvic pathology
- Methylene blue or indigo carmine dye injected through cervix; spill observed laparoscopically from fimbriae
- Simultaneously diagnoses endometriosis, pelvic adhesions, peritubal disease
- Indicated when: HSG/HyCoSy shows block, history suggests pelvic inflammatory disease (PID), endometriosis, prior pelvic surgery, or high CAT titres
Falloposcopy / Salpingoscopy
- Fiberoptic visualization of tubal ostia and intratubal mucosa (via hysteroscopy)
- Identifies intraluminal pathology (debris, mucosal agglutination)
- Limited by technical complexity and perforation risk; not routine
Step 4 — Treatment Based on Site and Severity of Block
A. Proximal Tubal Occlusion (PTO)
First consider: Is it true occlusion or spasm? (Cornual spasm on HSG is a common false positive — recheck with selective salpingography.)
Tubal Cannulation / Catheterization
- Performed via HSG-guided selective salpingography (fluoroscopic) or hysteroscopy + laparoscopy
- Passes a soft catheter into the tubal ostium; a guidewire is advanced to overcome obstruction
- Restores patency in up to 85% of cases
- Reocclusion rate ~30%; re-cannulation or IVF then considered
- Ongoing pregnancy rates: 12–44%
- Tubal perforation in 1.9–11% (usually minor)
Best candidates for cannulation:
- Spasm, stromal edema, amorphous debris, mucosal agglutination, viscous secretions
Poor candidates (proceed to IVF):
- Luminal fibrosis, TB, congenital atresia, failed prior reanastomosis, fibroids
Microsurgical Tubocornual Anastomosis (rarely done)
- Via laparotomy: excision of blocked isthmus, reimplantation into new cornual opening
- Reported pregnancy rates up to 68% in small series
- Reserved for specific cases; IVF preferred in most
B. Distal Tubal Occlusion
Accounts for 85% of all tubal infertility; usually post-inflammatory (PID, endometriosis, prior surgery).
Patient selection is critical:
| Favours Surgery | Favours IVF |
|---|---|
| Age <35 | Age ≥35 |
| Mild distal disease | Severe pelvic adhesions |
| Normal tubal mucosa | Diminished ovarian reserve |
| Absent/minimal adhesions | Combined proximal + distal disease |
| — | Male factor or other infertility factors |
Surgical options (laparoscopic/microsurgical):
| Procedure | Indication | Pregnancy Rate |
|---|---|---|
| Adhesiolysis | Peritubal/fimbrial adhesions | 32–42.2% |
| Fimbrioplasty | Fimbrial phimosis / partial distal block | 54.6–60% |
| Salpingostomy (neo-salpingostomy) | Complete distal occlusion; new opening created | 30–34.6% |
| Tubo-tubal anastomosis | Non-sterilization related | ~55.9% |
Ectopic pregnancy risk after distal tubal surgery: ~7.9% — Berek & Novak's Gynecology, p. 2061
C. Hydrosalpinx (Distal Occlusion with Fluid Collection)
Hydrosalpinx fluid is embryotoxic and impedes implantation.
- Meta-analysis (14 studies, 1,004 patients): IVF pregnancy rates significantly lower in the presence of hydrosalpinges
- Salpingectomy prior to IVF significantly improves both pregnancy and live birth rates compared to IVF with tubes in situ
- Laparoscopic tubal occlusion (proximal ligation/clipping) is a reasonable alternative to salpingectomy when salpingectomy is technically difficult
- Transvaginal needle aspiration and salpingostomy have less outcome data — not preferred
Key principle: If proceeding to IVF with hydrosalpinx, treat the hydrosalpinx first. — Berek & Novak's Gynecology, p. 2062
D. IVF (In Vitro Fertilization)
The primary treatment option in most cases of tubal block, especially when:
- Severe/bilateral disease
- Failed surgical correction or reocclusion
- Age ≥35 or diminished ovarian reserve
- Additional male factor or anovulation
- Tuberculous salpingitis (surgery ineffective)
"As success rates for ART continue to improve, the indications for surgical approaches in the treatment of tubal infertility have become increasingly limited." — Berek & Novak's Gynecology, p. 2060
Surgical Approach Summary
All tubal surgery is preferably performed laparoscopically (equivalent outcomes to laparotomy, faster recovery). Microsurgery principles (magnification, fine sutures, minimal trauma, irrigation) are applied.
Management Algorithm
Primary Infertility with Suspected Tubal Block
│
├── Full couple workup (semen analysis, ovarian reserve, uterine cavity)
│
├── Tubal patency assessment
│ ├── HSG / HyCoSy / HyFoSy (first-line)
│ └── Laparoscopy + chromopertubation if HSG abnormal or high clinical suspicion
│
├── PROXIMAL BLOCK
│ ├── Tubal cannulation (HSG-guided or hysteroscopic)
│ │ └── Success → TI / IUI; Failure/reocclusion → IVF
│ └── True fibrosis/TB → IVF directly
│
├── DISTAL BLOCK / ADHESIONS
│ ├── Age <35, mild disease, good ovarian reserve → Laparoscopic surgery
│ │ (adhesiolysis / fimbrioplasty / salpingostomy)
│ └── Age ≥35, severe disease, poor ovarian reserve → IVF
│
└── HYDROSALPINX
├── Salpingectomy (preferred) or tubal occlusion
└── Then proceed to IVF
Special Situations
| Situation | Action |
|---|---|
| Tuberculous salpingitis | IVF directly; anti-TB treatment first; surgery not beneficial |
| Cornual spasm on HSG | Repeat with selective salpingography; antispasmodics before HSG |
| Unilateral block, other tube normal | Trial of expectant management / IUI; consider surgery if young |
| Sterilization reversal request | Microsurgical reanastomosis if age <35, isthmic-isthmic, tube length >4 cm; IVF if older/poor reserve |
| Previous ectopic pregnancy | IVF preferred; surgical repair associated with higher ectopic risk |
Sources:
- Berek & Novak's Gynecology, pp. 2060–2062 (Treatment of Tubal Factor Infertility — Proximal Tubal Occlusion, Distal Tubal Occlusion, Hydrosalpinx, Sterilization Reversal)
- Berek & Novak's Gynecology, p. 2060 (Falloposcopy, Selective Salpingography)
- ESHRE Guidelines on Unexplained Infertility (HSG vs. HyCoSy; CAT screening)
This is a shared conversation. Sign in to Orris to start your own chat.