Hiv in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"HIV" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from authoritative textbooks including Harrison's 2025, Robbins, and Sherris Microbiology. Let me compile the full detailed response.
HIV (Human Immunodeficiency Virus) - Comprehensive Overview
Scanning electron micrograph: HIV (yellow) budding from an infected H9 T cell (blue/green)
(Courtesy of NIAID Rocky Mountain Laboratories)
1. Virology and Structure
HIV is a lentivirus belonging to the family Retroviridae. There are two types:
- HIV-1: Responsible for the vast majority of infections worldwide. Has four groups - M (Main), N, O, and P. Group M is further divided into 11 subtypes (clades A-K), with clade B predominating in Western nations.
- HIV-2: Found primarily in West Africa; similar pathogenesis but slower disease progression and naturally lacks the Vpu gene (has Vpx instead).
Viral Genome and Proteins
HIV-1 is an RNA virus with a 9.8 kb genome encoding:
| Gene | Product | Function |
|---|---|---|
| gag | p24 (capsid), p17 (matrix), p7 (nucleocapsid) | Structural proteins |
| pol | Reverse transcriptase, integrase, protease | Enzymatic replication |
| env | gp120 (surface), gp41 (transmembrane) | Envelope/entry |
| tat | Tat protein | Transcriptional transactivation |
| rev | Rev | Regulates mRNA export |
| nef | Nef | Downregulates CD4/MHC-I; enhances pathogenicity |
| vif, vpr, vpu | Accessory proteins | Host cell modification, viral release |
The extraordinary variability of HIV-1 arises from the low fidelity of reverse transcriptase (error-prone copying), which drives mutations especially in the hypervariable regions of the envelope (gp120 V3 loop). This contrasts with the relative stability of reverse transcriptase's active site. - Harrison's Principles of Internal Medicine 22E, 2025
2. Epidemiology
- Global burden: Approximately 39 million people living with HIV worldwide (UNAIDS 2023 data).
- Transmission routes: Unprotected sexual intercourse (most common globally), intravenous drug use (needle sharing), mother-to-child (vertical transmission - perinatal/breastfeeding), blood transfusion/organ transplantation (rare in developed countries), occupational needlestick exposure.
- Risk quantification (Harrison's):
- Needlestick from HIV+ source: ~0.23% per exposure (untreated)
- Mucous membrane exposure: ~0.09%
- Male-to-male sexual contact: accounts for ~two-thirds of incident cases in men in the USA
- Heterosexual contact: ~90% of new infections in women in the USA
- HIV disproportionately affects minority populations; ~60% of prevalent US cases affect Black women. - Goldman-Cecil Medicine International Edition
- CCR5-Δ32 mutation: ~1% of northern Europeans are homozygous and resistant to HIV infection; ~10-15% are heterozygous.
3. Pathogenesis
3a. Entry Mechanism
HIV entry requires CD4 as the primary receptor plus one of two major co-receptors:
- CCR5 (C-C chemokine receptor type 5): Used by R5 (M-tropic) viruses - predominate in early infection; infect monocytes/macrophages
- CXCR4 (C-X-C chemokine receptor type 4): Used by X4 (T-tropic) viruses - emerge in later disease; associate with rapid CD4 decline
- Dual-tropic R5X4 viruses: Use both co-receptors
The sequence of entry:
- gp120 binds CD4 → conformational change in gp120
- gp120 engages CCR5 or CXCR4 co-receptor (via V3 loop)
- gp41 undergoes conformational change → membrane fusion
- Viral RNA enters cytoplasm
The chemokines RANTES (CCL5), MIP-1α, MIP-1β (natural CCR5 ligands) block R5 entry by steric inhibition. SDF-1 (natural CXCR4 ligand) blocks X4 entry.
An accessory receptor, integrin α4β7, facilitates HIV targeting to gut-associated lymphoid tissue (GALT). - Harrison's Principles of Internal Medicine 22E
3b. Replication Cycle
- Attachment and fusion (gp120/gp41 - CD4/co-receptor interaction)
- Reverse transcription: Viral RNA → dsDNA via reverse transcriptase
- Nuclear import: Pre-integration complex enters nucleus
- Integration: Integrase incorporates proviral DNA into host genome
- Transcription: Host RNA polymerase II transcribes viral genes; Tat amplifies transcription; Rev exports unspliced mRNA
- Translation and processing: Viral protease cleaves polyproteins
- Assembly and budding: New virions bud from cell membrane
3c. CD4+ T Cell Depletion - Mechanisms
The central immunopathological event in HIV disease is progressive depletion of CD4+ T cells. Multiple mechanisms are involved:
Direct mechanisms:
- Loss of plasma membrane integrity during viral budding
- Accumulation of unintegrated viral DNA
- Intracellular gp120-CD4 autofusion events
- Syncytia formation (especially X4 viruses)
Indirect mechanisms:
- Pyroptosis: Abortive HIV infection of resting CD4+ T cells activates the inflammasome (caspase-1), releasing inflammatory cytokines and recruiting more cells - a major mechanism of CD4 depletion
- Activation-induced cell death: Chronic immune activation of uninfected cells causes apoptosis
- Autoimmunity and innocent bystander killing
- Inhibition of lymphopoiesis: Loss of CD4+ precursors in thymus
- Elimination of HIV-infected cells by CD8+ cytotoxic T cells
The viral reservoir persists even with effective ART: integrated provirus in long-lived memory T cells and follicular helper T cells in germinal centers (CD8+ CTLs are excluded from germinal centers, so these infected cells survive). - Robbins & Kumar Basic Pathology; Harrison's 22E
3d. Infection of Non-T Cells
- Macrophages: Infected via CCR5; serve as a reservoir; do not die but carry virus to tissues including the brain
- Dendritic cells (DCs): Carry HIV to lymph nodes, presenting it to CD4+ T cells; Langerhans cells beneath mucosal surfaces are early targets during sexual transmission
- Microglial cells of the brain: Infected via CCR5; underlie HIV-associated neurocognitive disorder (HAND)
- Gut-associated lymphoid tissue (GALT): Massive early depletion of intestinal CD4+ T cells occurs within days to weeks of primary infection - a key early event
3e. Immune Dysfunction
| Category | Abnormality |
|---|---|
| Quantitative | Lymphopenia; preferential loss of activated and memory CD4+ T cells |
| T cell function | Decreased delayed-type hypersensitivity; reduced antigen-induced proliferation; decreased Th1 responses; defective cell-mediated immunity |
| B cell function | Hypergammaglobulinemia; poor de novo antibody responses; loss of memory B cells |
| NK cells | Decreased cytotoxic activity |
| Macrophages | Decreased phagocytosis, IL-12 production, and antigen presentation |
4. Clinical Course
The classic clinical course of untreated HIV infection is illustrated below:
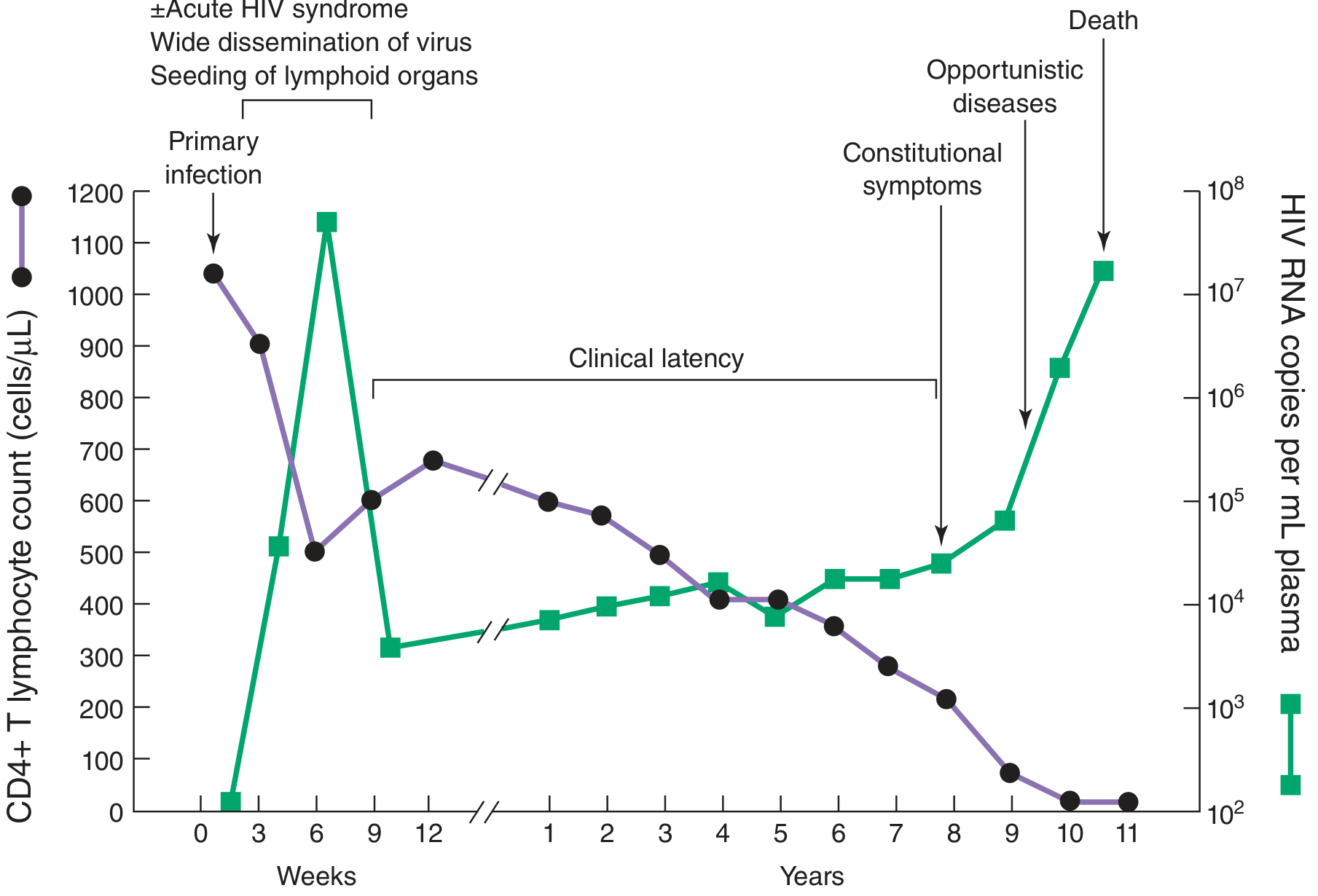
Figure: Typical course of HIV infection - Harrison's Principles of Internal Medicine 22E (2025)
Stage 1 - Acute (Primary) HIV Infection
- Occurs 2-4 weeks after transmission
- ~50-70% of individuals develop a mononucleosis-like acute HIV syndrome:
- Fever, malaise, lymphadenopathy, pharyngitis, rash (erythematous maculopapular), myalgia/arthralgia
- Less commonly: headache, oral ulcers, diarrhea, nausea/vomiting
- Rarely: aseptic meningitis, peripheral neuropathy
- Very high viral load (up to 10^7 copies/mL) - peak viremia → wide dissemination
- CD4+ count drops sharply then partially recovers
- Lasts 1-2 weeks; resolves as immune response develops
- HIV establishes itself in lymphoid organs (seeding phase)
Stage 2 - Chronic Asymptomatic (Clinical Latency)
- Lasts average 8-10 years untreated
- Patient is clinically well but virologically active (viral set point: typically 10^3-10^5 copies/mL)
- CD4+ count declines slowly (~50-100 cells/μL/year)
- May have persistent generalized lymphadenopathy (PGL)
- Viral replication is ongoing in lymphoid tissues
- "Virologic set point": Higher set point = faster progression to AIDS
Stage 3 - Symptomatic / AIDS
- Defined by CDC as:
- CD4+ count <200 cells/μL (in persons >6 years), OR
- Presence of an AIDS-defining opportunistic illness (Stage C conditions)
- Constitutional symptoms precede OIs: fever, night sweats, weight loss, diarrhea
CDC HIV Staging:
| Stage | CD4+ Count |
|---|---|
| Stage 1 | ≥500 cells/μL |
| Stage 2 | 200-499 cells/μL |
| Stage 3 (AIDS) | <200 cells/μL |
5. AIDS-Defining Opportunistic Illnesses
These occur when CD4+ count falls below threshold levels:
| CD4 Threshold | Typical Opportunistic Infections/Complications |
|---|---|
| <500 | Oral candidiasis, recurrent herpes zoster, recurrent bacterial pneumonia |
| <200 | Pneumocystis jirovecii pneumonia (PCP), toxoplasmosis, disseminated histoplasmosis, Kaposi's sarcoma |
| <100 | Cryptococcal meningitis, CMV disease (retinitis, colitis), disseminated MAI |
| <50 | CMV retinitis, disseminated MAC, primary CNS lymphoma, PML |
Full list of CDC Stage 3 (AIDS)-defining illnesses includes:
Bacterial infections (multiple/recurrent), esophageal/tracheal candidiasis, invasive cervical cancer, coccidioidomycosis, cryptococcosis (extrapulmonary), cryptosporidiosis, CMV disease, CMV retinitis, HIV encephalopathy, HSV (chronic ulcers >1 month), histoplasmosis (disseminated), isosporiasis, Kaposi's sarcoma, Burkitt's lymphoma, immunoblastic lymphoma, primary CNS lymphoma, MAC/MAI, tuberculosis, P. jirovecii pneumonia, recurrent pneumonia, progressive multifocal leukoencephalopathy (PML), recurrent Salmonella septicemia, CNS toxoplasmosis, HIV wasting syndrome. - Harrison's 22E
6. Diagnosis
HIV Testing
- 4th generation combination assays (preferred): Detect both p24 antigen AND HIV-1/HIV-2 antibodies; can detect infection as early as 18-45 days after exposure (window period shortened)
- 3rd generation antibody-only ELISA: Window period ~3-6 weeks
- Western blot / Immunofluorescence assay: Confirmatory (now being replaced by supplemental antibody differentiation assays)
- HIV RNA (viral load) PCR: Detects acute infection before seroconversion; quantifies viral burden; guides treatment
- CD4+ T cell count: Absolute count and percentage; determines stage and guides prophylaxis decisions
- HIV genotyping/resistance testing: Done at baseline and at treatment failure
- Rapid tests: Point-of-care antibody tests; results in 20-60 minutes
Monitoring Parameters
- HIV RNA (viral load): Goal is <50 copies/mL on ART (undetectable)
- CD4+ count: Every 3-6 months; determines need for OI prophylaxis
- Drug resistance testing (genotype): Before starting ART and at virologic failure
- HLA-B*5701 testing: Before abacavir use (risk of hypersensitivity reaction)
- CCR5 tropism assay: Before maraviroc use
7. Treatment - Antiretroviral Therapy (ART)
When to Start
ART should be initiated as soon as possible after diagnosis in ALL patients, with rare exceptions:
- Cryptococcal meningitis: Delay ART 4-6 weeks (immune reconstitution inflammatory syndrome risk)
- Active TB: Delay ART 2-8 weeks depending on CD4+ count
- For patients with an OI and CD4 ≥50: Consider 2-4 week delay
- For CD4 <50: Start ART as soon as possible
Drug Classes
| Class | Mechanism | Examples |
|---|---|---|
| NRTIs (Nucleoside/Nucleotide Reverse Transcriptase Inhibitors) | Competitive inhibition + chain termination of reverse transcriptase | Tenofovir (TDF/TAF), Emtricitabine (FTC), Lamivudine (3TC), Abacavir (ABC), Zidovudine (AZT), Stavudine (d4T) |
| NNRTIs (Non-Nucleoside RTIs) | Non-competitive binding to reverse transcriptase | Efavirenz (EFV), Rilpivirine (RPV), Etravirine (ETR), Nevirapine (NVP) |
| PIs (Protease Inhibitors) | Inhibit viral protease (prevents polyprotein cleavage) | Darunavir (DRV), Atazanavir (ATV), Ritonavir (RTV - booster), Lopinavir |
| INSTIs (Integrase Strand Transfer Inhibitors) | Block proviral DNA integration | Dolutegravir (DTG), Bictegravir (BIC), Raltegravir (RAL), Cabotegravir (CAB), Elvitegravir (EVG) |
| CCR5 Antagonists | Block CCR5 co-receptor, prevent viral entry | Maraviroc (MVC) |
| Fusion Inhibitors | Block gp41-mediated membrane fusion | Enfuvirtide (T-20) |
| Capsid Inhibitors | Interfere with multiple lifecycle steps via p24 capsid | Lenacapavir (SC injection every 6 months) |
| CD4 Attachment Inhibitors | Block gp120-CD4 interaction | Ibalizumab |
Preferred Initial Regimens (DHHS Guidelines)
A typical regimen includes:
- Two NRTIs (usually tenofovir-based [TDF or TAF] + FTC/3TC)
- PLUS one of: NNRTI, INSTI, or boosted PI
Most preferred backbone: Tenofovir alafenamide (TAF) + emtricitabine (FTC)
Preferred third agent: Dolutegravir (DTG) or Bictegravir (BIC) - INSTIs with high barrier to resistance
Two-drug regimen: Dolutegravir + 3TC (for HBV-negative patients with baseline viral load <500,000 copies/mL) - Harrison's 22E
Key fixed-dose combinations:
- Biktarvy: Bictegravir/TAF/FTC (once daily - preferred first-line)
- Triumeq: Abacavir/Dolutegravir/Lamivudine
- Atripla: Efavirenz/FTC/TDF
- Cabotegravir + Rilpivirine (Cabenuva): Monthly or every-2-month injectable regimen
Long-acting options: Lenacapavir (every 6 months SC injection) for heavily treatment-experienced patients; Cabotegravir LA (every 2 months) for virologically suppressed patients.
Treatment Goals
- Achieve and maintain undetectable viral load (<50 copies/mL)
- Preserve and restore CD4+ count
- Prevent opportunistic infections
- Reduce HIV transmission risk ("U=U": Undetectable = Untransmittable)
- Minimize drug toxicity
Drug Resistance
- Resistance arises from mutations in viral genes encoding drug targets
- High-level replication in the absence of ART generates quasi-species with resistant mutations
- Resistance testing (genotype) guides regimen selection at baseline and at virologic failure
- Drugs with high genetic barrier to resistance (e.g., dolutegravir, bictegravir) are preferred because multiple mutations are needed to overcome them
8. Opportunistic Infection Prophylaxis
| CD4 Count | Prophylaxis |
|---|---|
| <200 cells/μL | TMP-SMX (trimethoprim-sulfamethoxazole) for PCP prophylaxis |
| <100 cells/μL | TMP-SMX also covers toxoplasmosis; if allergic: dapsone + pyrimethamine |
| <50 cells/μL | Azithromycin for MAC prophylaxis (now often deferred if ART started promptly) |
9. Prevention
Pre-Exposure Prophylaxis (PrEP)
- Oral PrEP: Tenofovir/emtricitabine (Truvada) once daily - reduces transmission risk by >99% with adherence
- Injectable PrEP: Cabotegravir LA (every 2 months) - shown to be even more effective than oral TDF/FTC
- Recommended for high-risk individuals (MSM, serodiscordant couples, IDU)
Post-Exposure Prophylaxis (PEP)
- Must be initiated within 72 hours of exposure
- nPEP regimen: Tenofovir-emtricitabine 300/200 mg daily + Raltegravir 400 mg q12h OR Dolutegravir 50 mg once daily for 28 days
- Follow-up HIV testing at 6 weeks
- Risk of transmission: ~0.23% per needlestick (untreated); PEP dramatically reduces this. - Washington Manual of Medical Therapeutics
Other Prevention Strategies
- Consistent condom use
- Harm reduction for PWID (needle exchange programs, opioid agonist therapy)
- Treatment as prevention (TasP): ART in HIV+ individuals reduces transmission to near zero when viral load is undetectable
- Male circumcision: Reduces female-to-male transmission by ~60%
- Prevention of mother-to-child transmission (PMTCT): ART during pregnancy, safe delivery practices, formula feeding (where safe and feasible)
- Universal precautions in healthcare settings
10. HIV-Associated Complications
Neurological (HAND - HIV-Associated Neurocognitive Disorder)
- HIV enters CNS early via infected monocytes/macrophages (Trojan horse model)
- Microglial cell infection disrupts neuronal function
- Spectrum: Asymptomatic neurocognitive impairment → HIV-associated mild neurocognitive disorder → HIV-associated dementia
Malignancies
- Kaposi's sarcoma (AIDS-defining): Caused by HHV-8; cutaneous/visceral vascular tumors
- Primary CNS lymphoma: EBV-driven; occurs at CD4 <50
- Non-Hodgkin lymphoma (Burkitt's, immunoblastic)
- Invasive cervical cancer: HPV-related; annual Pap smear recommended for all HIV+ women
- Increased risk of anal, lung, hepatic, and other cancers
Immune Reconstitution Inflammatory Syndrome (IRIS)
- Occurs 2-8 weeks after ART initiation
- Paradoxical worsening of a pre-existing opportunistic infection as immunity recovers
- Risk factors: Low baseline CD4+ count, high antigen burden, rapid CD4+ increase
- Management: Continue ART; NSAIDs or corticosteroids for severe cases
Metabolic and Cardiovascular
- Dyslipidemia (especially with PIs)
- Insulin resistance / lipodystrophy
- Increased risk of cardiovascular disease (partly due to chronic immune activation)
- Some "non-AIDS-defining" serious adverse events (heart attack, stroke) are linked to ongoing HIV replication - reason why treatment interruptions are harmful
11. Genetic Host Factors Influencing Disease Progression
- HLA-B57 and HLA-B27 alleles: Protective - associated with slower progression, lower viral set point, stronger CD8+ T cell responses. Enriched among "elite controllers" (spontaneously control HIV without ART)
- HLA-B35 allele: Detrimental - faster progression to AIDS, higher viral load
- HLA-A1/B8/DR3 (AH 8.1 haplotype): Common in Europeans; associated with rapid CD4 decline and faster progression
- CCR5-Δ32 homozygotes: Near-complete resistance to HIV-1 infection
- CCR5-Δ32 heterozygotes: Slower disease progression
- "Berlin patient" and subsequent cases: Allogeneic stem cell transplant from CCR5-Δ32 homozygous donors led to functional cure in a small number of HIV+ cancer patients - the only documented cases approaching eradication - Harrison's 22E
12. Special Populations
Pregnancy
- ART should be given to ALL pregnant women regardless of CD4+ count
- Same principles apply; regimen chosen for safety in pregnancy
- Undetectable viral load at delivery reduces vertical transmission to <1%
Children
- Unique pharmacologic, virologic, and immunologic considerations
- Earlier and more aggressive ART initiation recommended
Recent Evidence (2024-2025)
Recent systematic review (Zace et al., 2024, PMID 39288983) addressed management of low-level HIV viremia on ART, highlighting that low-level viremia (detectable but <1000 copies/mL) is associated with virologic failure risk and warrants close monitoring and possible regimen optimization.
Sources:
- Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill Medical)
- Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
- Sherris & Ryan's Medical Microbiology, 8th Edition
- Goldman-Cecil Medicine International Edition
- The Washington Manual of Medical Therapeutics
- Medical Microbiology 9e (Murray)
This is a shared conversation. Sign in to Orris to start your own chat.