Femoral triangle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I have all the content needed for a thorough answer. Here is the complete overview:
Femoral Triangle
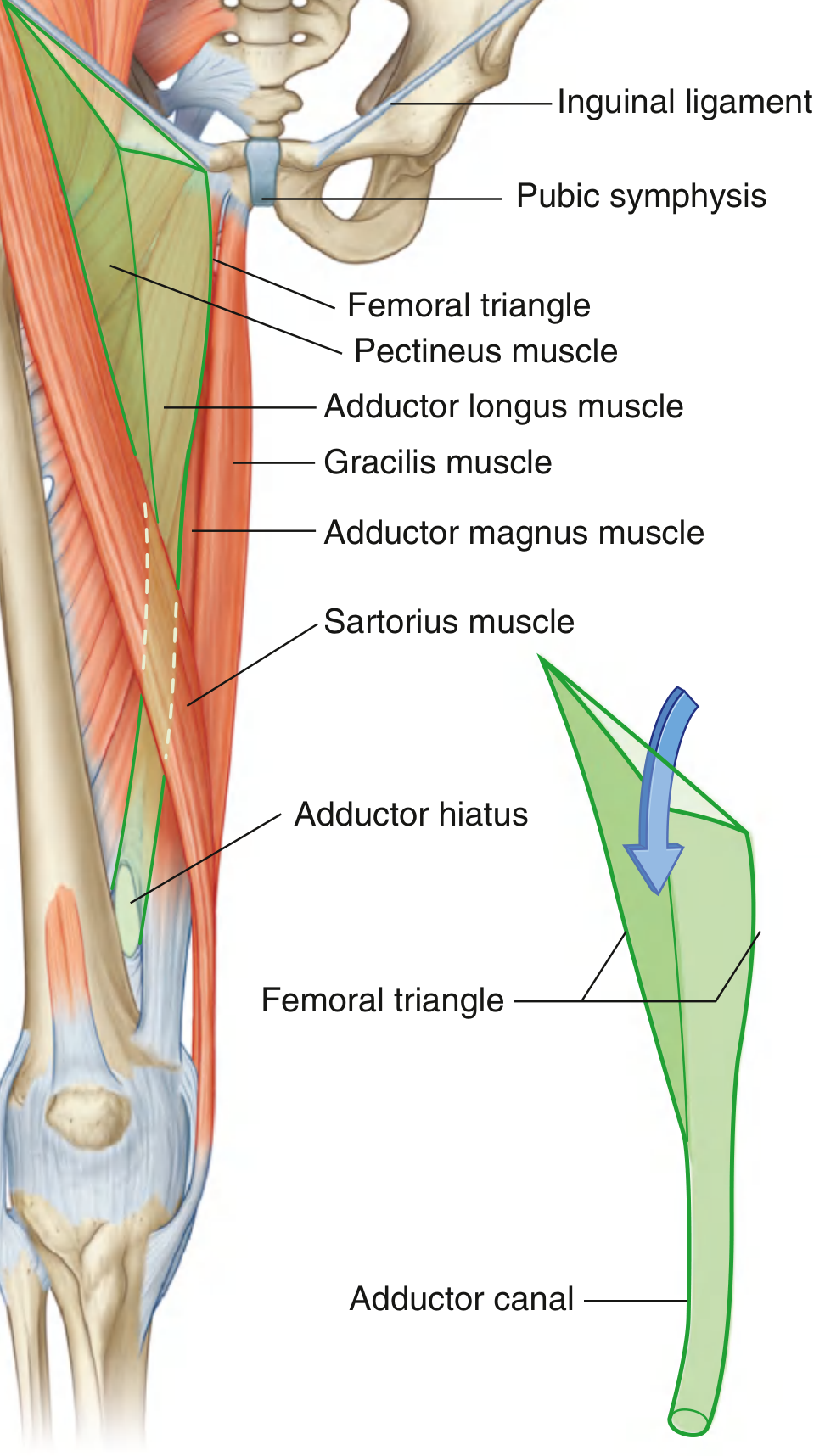
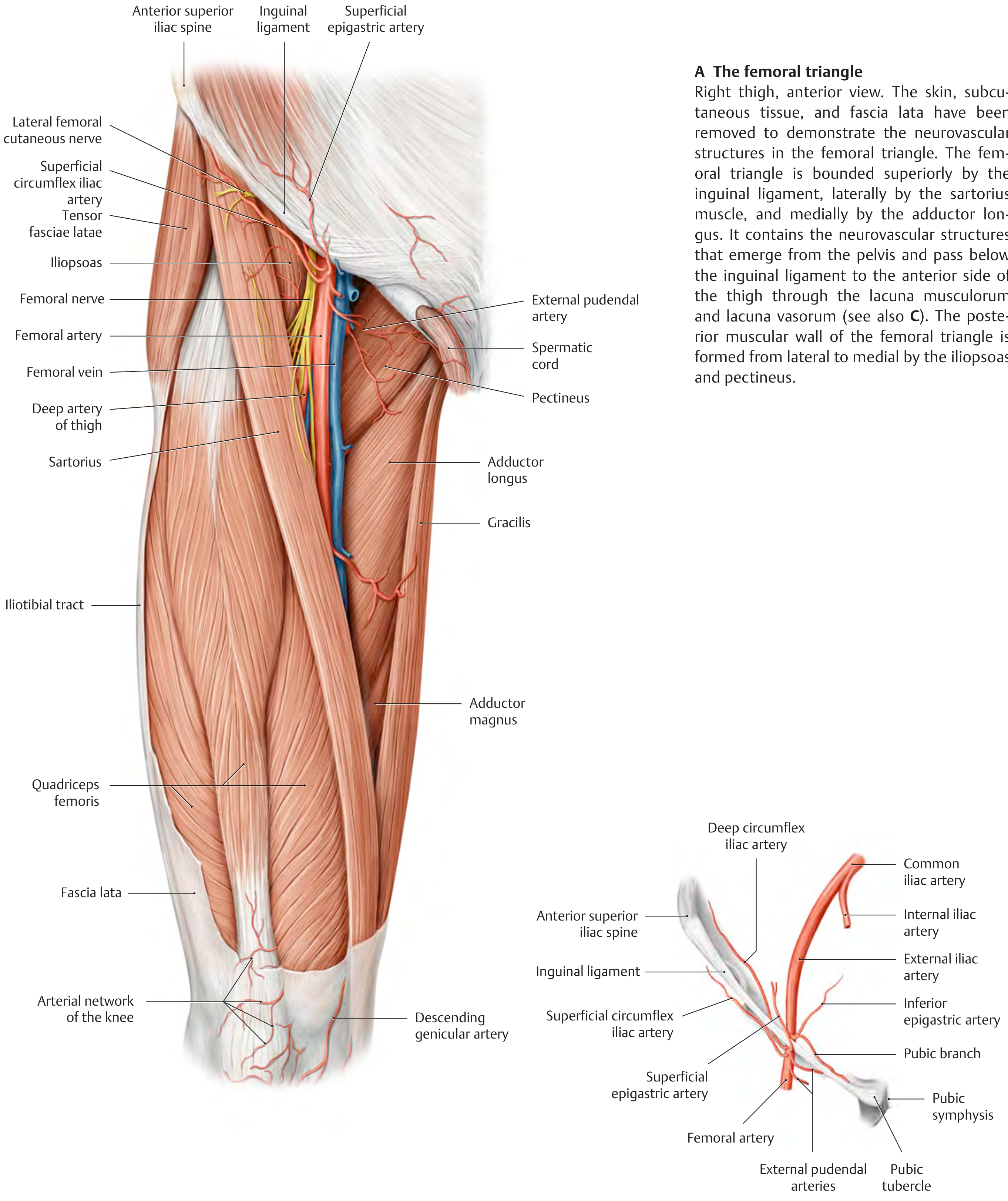
The femoral triangle is a wedge-shaped (pyramidal) depression located in the upper anterior thigh, at the junction between the anterior abdominal wall and the lower limb. It serves as a key passageway for major neurovascular structures entering the leg.
Boundaries
| Border | Structure |
|---|---|
| Base (superior) | Inguinal ligament (from ASIS to pubic tubercle) |
| Lateral border | Medial margin of the sartorius muscle |
| Medial border | Medial margin of the adductor longus muscle |
| Apex (inferior) | Where sartorius and adductor longus converge; opens inferiorly into the adductor canal |
Floor (from lateral to medial): Iliopsoas (lateral), pectineus (medial), and adductor longus (most medial).
Roof: Fascia lata (deep fascia) and skin, pierced by the great saphenous vein at the saphenous opening (fossa ovalis).
- Gray's Anatomy for Students
Contents
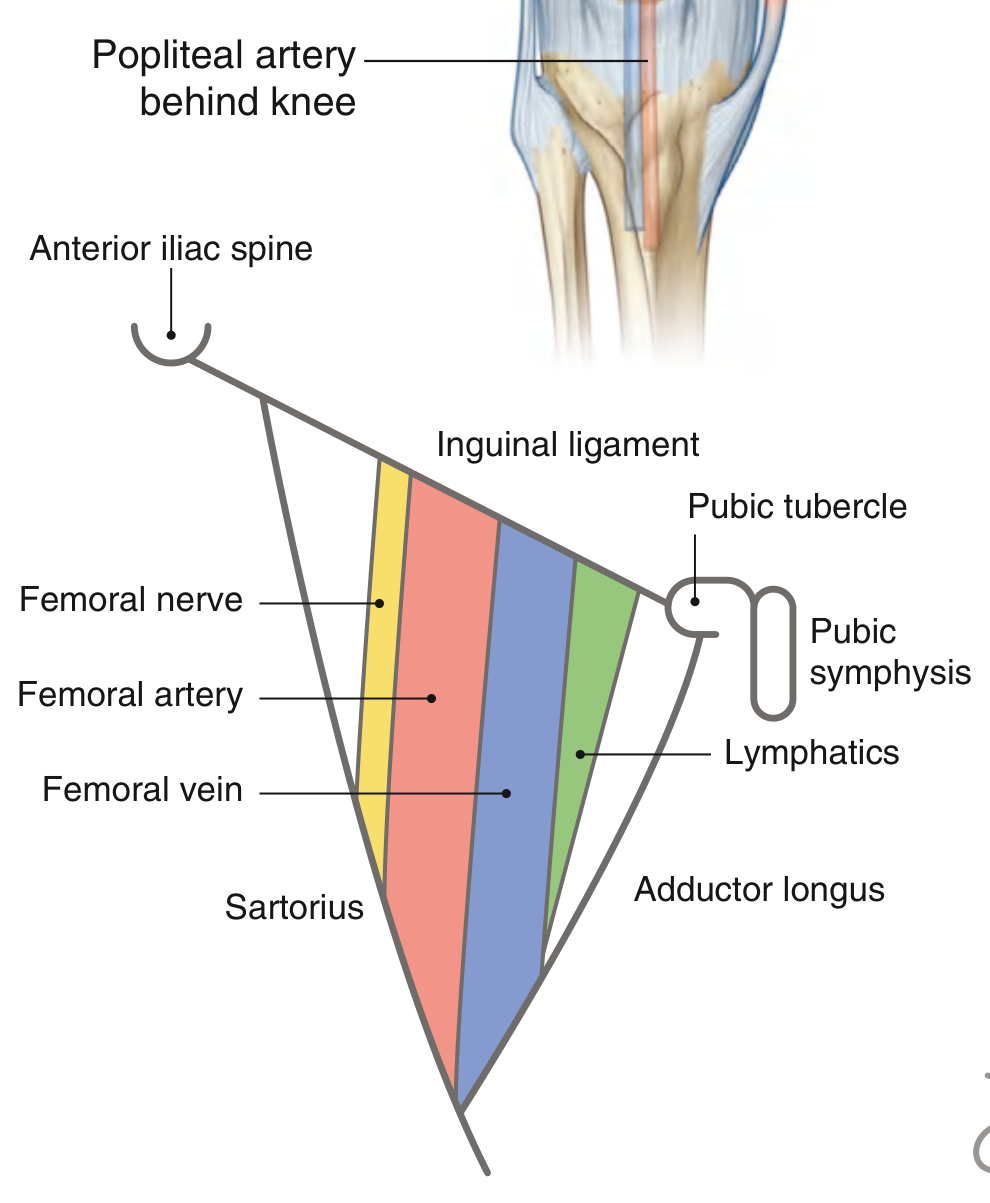
From lateral to medial (mnemonic: NAVY - Nerve, Artery, Vein, Y-fronts/lymphatics):
- Femoral nerve (L2-L4) - lateral; lies outside the femoral sheath
- Femoral artery - continuation of the external iliac artery, enters under the inguinal ligament; palpable midway between ASIS and pubic symphysis
- Femoral vein - medial to the artery
- Femoral canal (lymphatics + deep inguinal lymph nodes, including the node of Cloquet/Rosenmüller) - most medial
Femoral Sheath
The femoral artery, vein, and lymphatics (but not the femoral nerve) are enclosed in a funnel-shaped fascial sleeve called the femoral sheath, continuous superiorly with transversalis fascia and iliac fascia of the abdomen. It has three compartments:
| Compartment | Contents |
|---|---|
| Lateral | Femoral artery |
| Intermediate | Femoral vein |
| Medial (femoral canal) | Lymphatics; potentially a femoral hernia site |
The femoral canal is the most medial compartment. Its superior opening (femoral ring) is bounded by: inguinal ligament anteriorly, femoral vein laterally, lacunar ligament medially, pectineal ligament posteriorly. It is a potential weak point and the site of femoral hernias.
- Gray's Anatomy for Students, p. 675-676
Detailed Neurovascular Anatomy
Femoral Artery
- Continuation of the external iliac artery below the inguinal ligament
- Gives off the profunda femoris (deep artery of the thigh) in the triangle - the main blood supply to the thigh
- Also gives: superficial epigastric artery, superficial circumflex iliac artery, superficial and deep external pudendal arteries
- At the apex, passes into the adductor canal (Hunter's canal), exiting as the popliteal artery through the adductor hiatus
Femoral Vein
- Medial to the femoral artery
- Receives the great saphenous vein at the saphenous opening (fossa ovalis)
- Receives tributaries corresponding to the branches of the femoral artery
Femoral Nerve (L2, L3, L4)
- Largest branch of the lumbar plexus
- Enters the thigh lateral to the femoral artery, outside the femoral sheath
- Within or just below the triangle, divides into anterior and posterior divisions:
- Anterior: cutaneous branches to the anteromedial thigh (medial and intermediate femoral cutaneous nerves)
- Posterior: motor to quadriceps femoris and rectus femoris; gives off the saphenous nerve (continues into adductor canal)
Adductor Canal (Hunter's Canal)
The apex of the femoral triangle is continuous inferiorly with the adductor canal (subsartorial canal), a fascial tunnel deep to the sartorius. It transmits:
- Femoral artery and vein
- Saphenous nerve
- Nerve to vastus medialis
The canal ends at the adductor hiatus in adductor magnus, where the vessels become the popliteal artery and vein.
Surface Anatomy and Clinical Relevance
Pulse point
The femoral artery pulse is felt just below the midpoint of the inguinal ligament (midinguinal point = midway between ASIS and pubic symphysis). This is a standard site for:
- Pulse palpation
- Femoral artery catheterization (angiography, cardiac catheterization, angioplasty)
- Femoral venous access (for right heart catheterization, pulmonary artery catheterization, dialysis)
Femoral Hernia
- Protrusion of abdominal contents through the femoral ring into the femoral canal
- More common in women (wider pelvis, wider femoral ring)
- Presents as a mass below and lateral to the pubic tubercle (distinguishing it from inguinal hernias, which are above and medial to the pubic tubercle)
- High risk of strangulation due to the rigid boundaries of the femoral ring
Inguinal Lymphadenopathy
The superficial inguinal nodes lie below the inguinal ligament in the subcutaneous tissue. Deep inguinal nodes lie within the femoral canal. These drain lymph from the lower limb, perineum, and lower abdominal wall. Enlargement (lymphadenopathy) may indicate infection, malignancy, or inflammation in these territories.
Lumbar Plexus Blocks / Femoral Nerve Block
The femoral nerve's position lateral to the femoral artery in the triangle makes this a commonly used site for regional anesthesia of the anterior thigh and knee.
Summary Table
| Feature | Detail |
|---|---|
| Shape | Wedge/pyramid, apex inferiorly |
| Base | Inguinal ligament |
| Lateral wall | Sartorius (medial margin) |
| Medial wall | Adductor longus (medial margin) |
| Floor | Iliopsoas (lateral) + pectineus (medial) |
| Roof | Fascia lata + skin |
| Contents (L→M) | Femoral nerve, Femoral artery, Femoral vein, Femoral canal (lymphatics) |
| Apex continues as | Adductor canal (Hunter's canal) |
| Key clinical relevance | Femoral pulse, vascular access, femoral hernia, lymph nodes |
Sources: Gray's Anatomy for Students; THIEME Atlas of General Anatomy and Musculoskeletal System
Histology of cartilage
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the content and images needed for a comprehensive response.
Histology of Cartilage
Cartilage is an avascular specialized connective tissue composed of cells (chondrocytes) embedded in an abundant, firm but pliable extracellular matrix (ECM). Over 95% of cartilage volume is ECM; chondrocytes occupy only 3-5% of the total mass.
General Properties
- No blood vessels, lymphatics, or nerves - nutrients reach chondrocytes entirely by diffusion through the matrix
- The ECM's high glycosaminoglycan (GAG) content binds large amounts of water (60-80% of cartilage net weight), enabling this diffusion and providing resilience under compression
- Surrounded by a perichondrium (except articular cartilage and epiphyseal plates)
The Cells: Chondroblasts and Chondrocytes
Chondroblasts are young, active cells derived from the perichondrium. They synthesize and secrete all ECM components (collagen, proteoglycans, GAGs). As they become surrounded by their own secreted matrix, they are termed chondrocytes and occupy small spaces called lacunae.
Chondrocytes:
- Rounded/ovoid cells with a central nucleus, prominent nucleolus
- Cytoplasm contains abundant rough ER (rER), Golgi apparatus, lipid droplets, and glycogen - reflecting high secretory activity
- Do not divide readily in mature cartilage (limited repair capacity)
- Chondrocytes that have recently divided remain clustered together as isogenous groups (cell nests) - 2-8 cells sharing a single lacuna
The Extracellular Matrix
Molecular Composition of Hyaline Cartilage (Fig. 7.2)
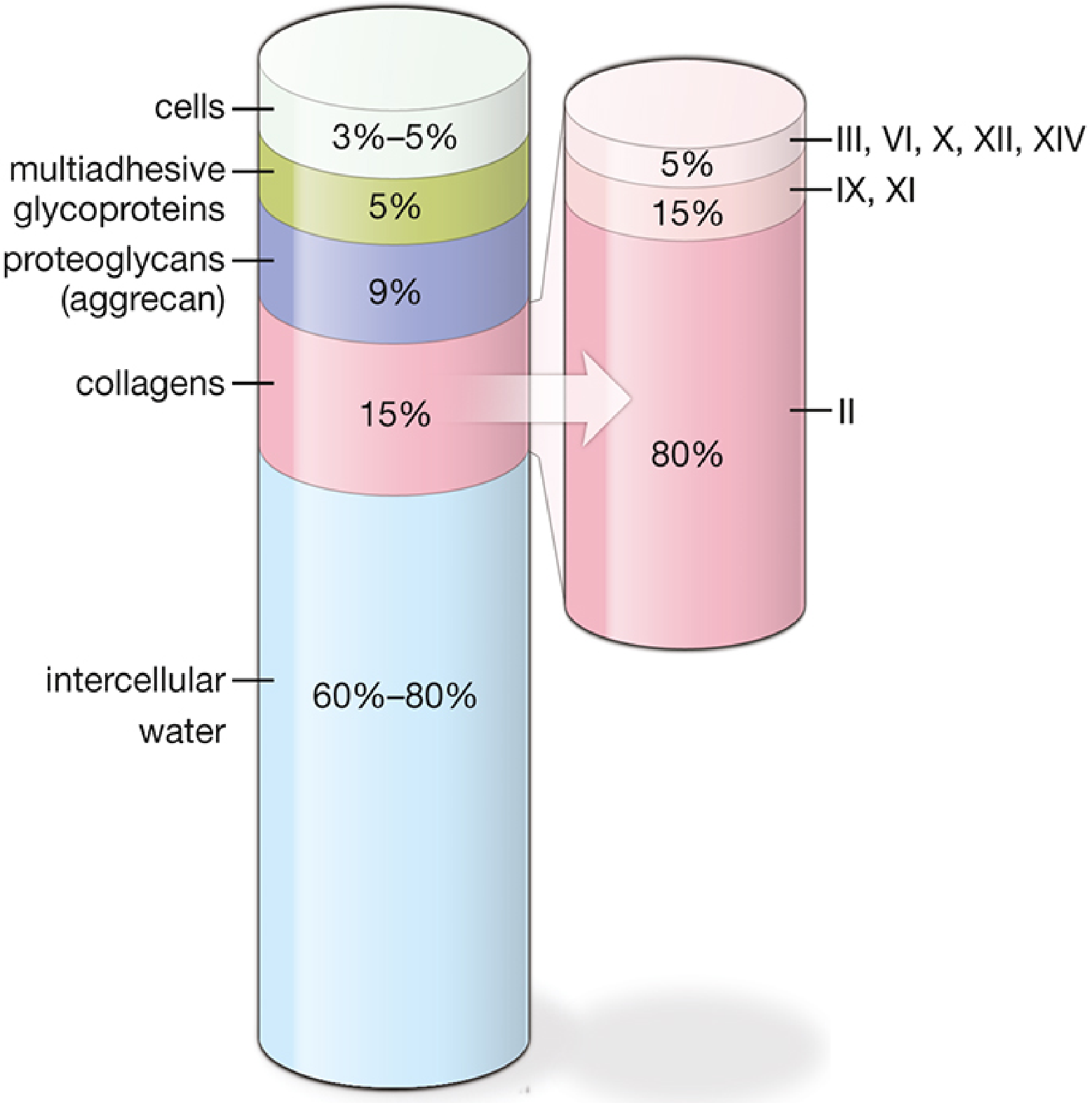
1. Collagen fibers (15% of total weight):
- Type II collagen - predominant (80% of all collagen); forms thin 20-nm fibrils creating a tension-resisting meshwork
- Type IX - links fibrils to proteoglycan molecules
- Type XI - regulates fibril diameter
- Type X - organizes fibrils into a 3D hexagonal lattice (important for mechanical function)
- Type VI - concentrated in the capsular matrix (pericellular zone); anchors chondrocytes to the matrix via integrin receptors
2. Proteoglycans (9% of total weight):
- Aggrecan is the major proteoglycan. Each aggrecan monomer has a core protein with many attached GAG chains (chondroitin sulfate and keratan sulfate)
- Aggrecan monomers bind to hyaluronan via link proteins to form enormous proteoglycan aggregates
- These aggregates are highly hydrated and enable cartilage to bear compressive loads
3. Multiadhesive glycoproteins (5%):
- Fibronectin, decorin, laminin - mediate cell-matrix adhesion
Matrix Zones Around Chondrocytes
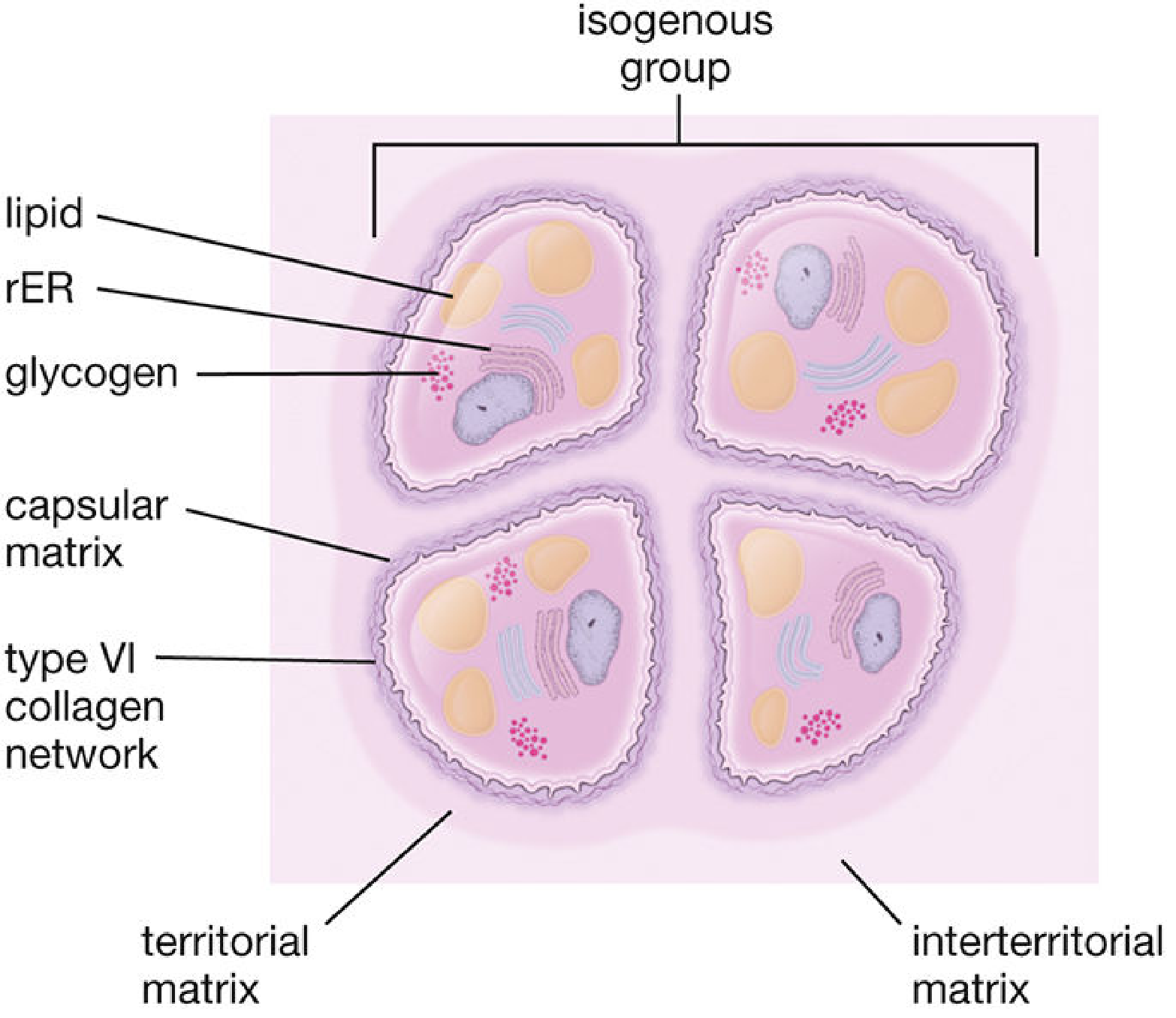
| Zone | Location | Composition | Staining |
|---|---|---|---|
| Capsular (pericellular) | Immediately around each chondrocyte | Type VI collagen network, highest concentration of sulfated proteoglycans, fibronectin, laminin | Most intensely basophilic |
| Territorial | Surrounds the isogenous group | Type II + IX collagen, lower proteoglycan concentration | Moderately basophilic |
| Interterritorial | Between groups | Largest area; lowest proteoglycan concentration, largest collagen fibrils | Least basophilic |
Types of Cartilage
1. Hyaline Cartilage
The most common type.
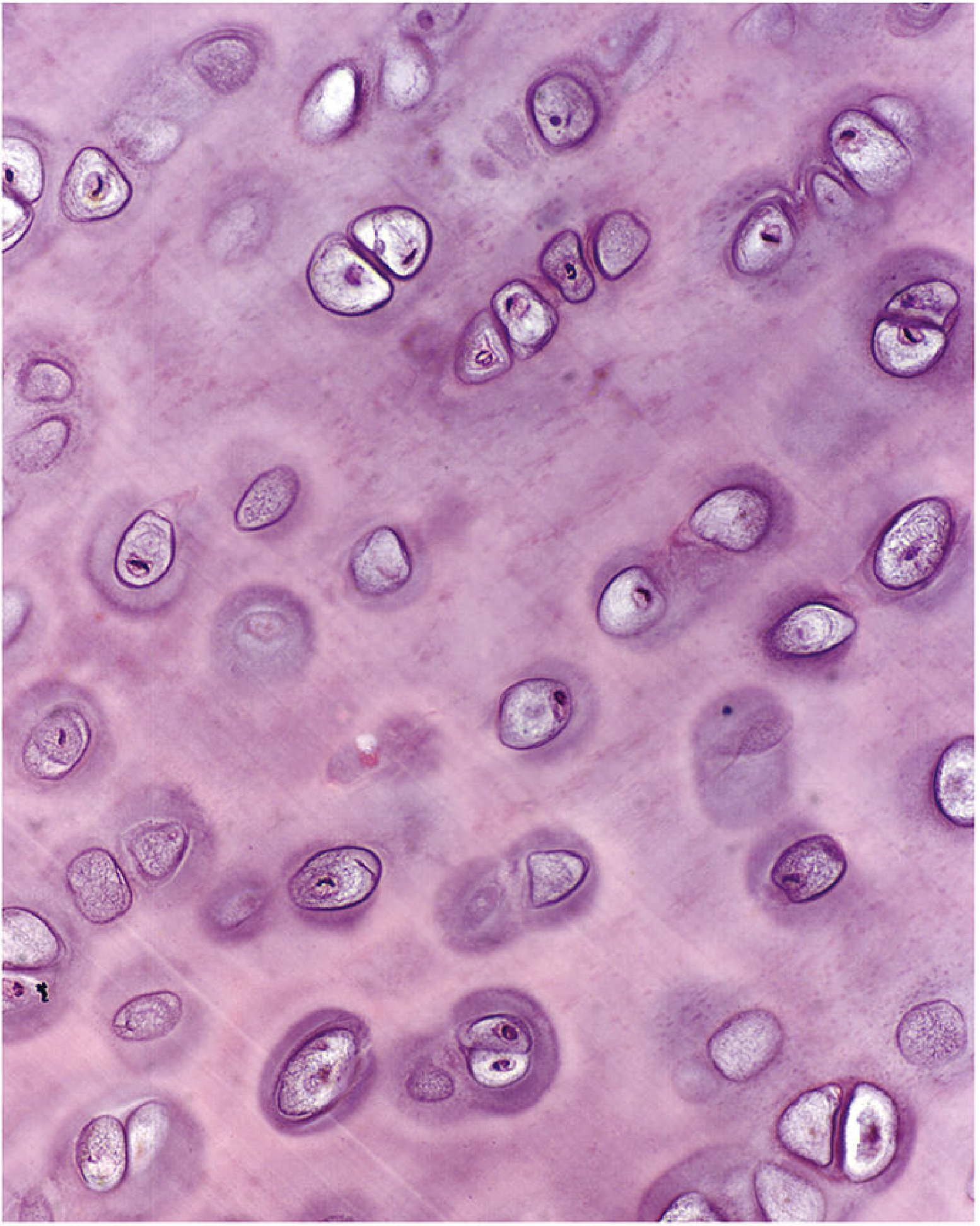
Histological appearance:
- Matrix appears glassy/homogeneous ("hyaline" = glassy) on H&E - type II collagen fibrils are invisible because they have the same refractive index as the surrounding ground substance
- Chondrocytes in lacunae, often in isogenous groups
- Surrounded by perichondrium (except articular cartilage and epiphyseal plates)
- Matrix stains basophilic with H&E (due to sulfated GAGs) and metachromatic with toluidine blue
Locations:
- Articular surfaces of synovial joints
- Costal cartilages (ribs)
- Larynx (thyroid, cricoid, arytenoid cartilages)
- Tracheal rings and bronchial plates
- Nasal cartilages
- Fetal skeleton (precursor to most bones via endochondral ossification)
- Epiphyseal growth plates
Key feature: Can calcify with aging or during endochondral ossification.
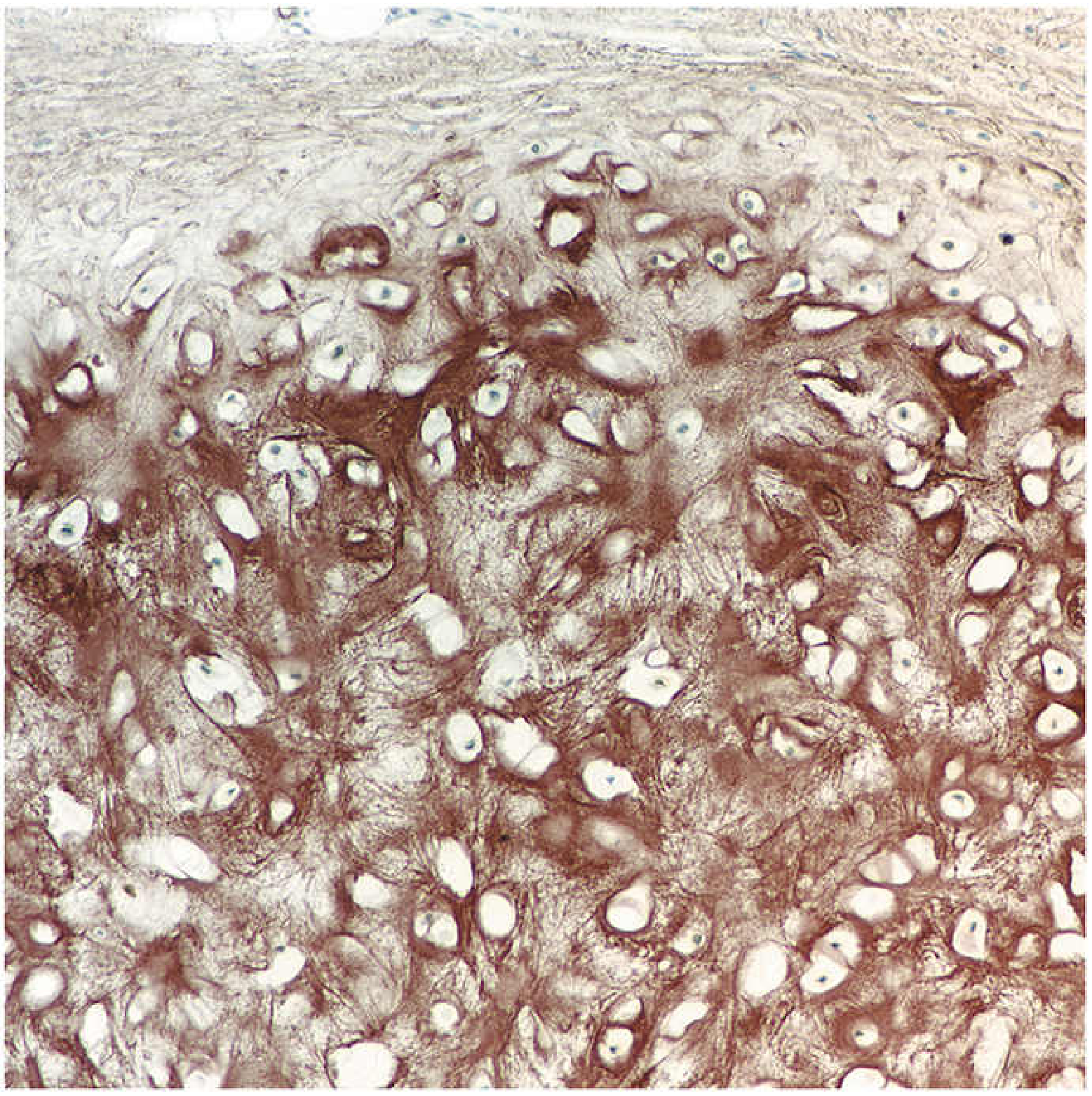
Special Structure: Articular Cartilage
Articular cartilage is a subtype of hyaline cartilage with no perichondrium on either surface and is 2-5 mm thick. It is organized into 4 zones:
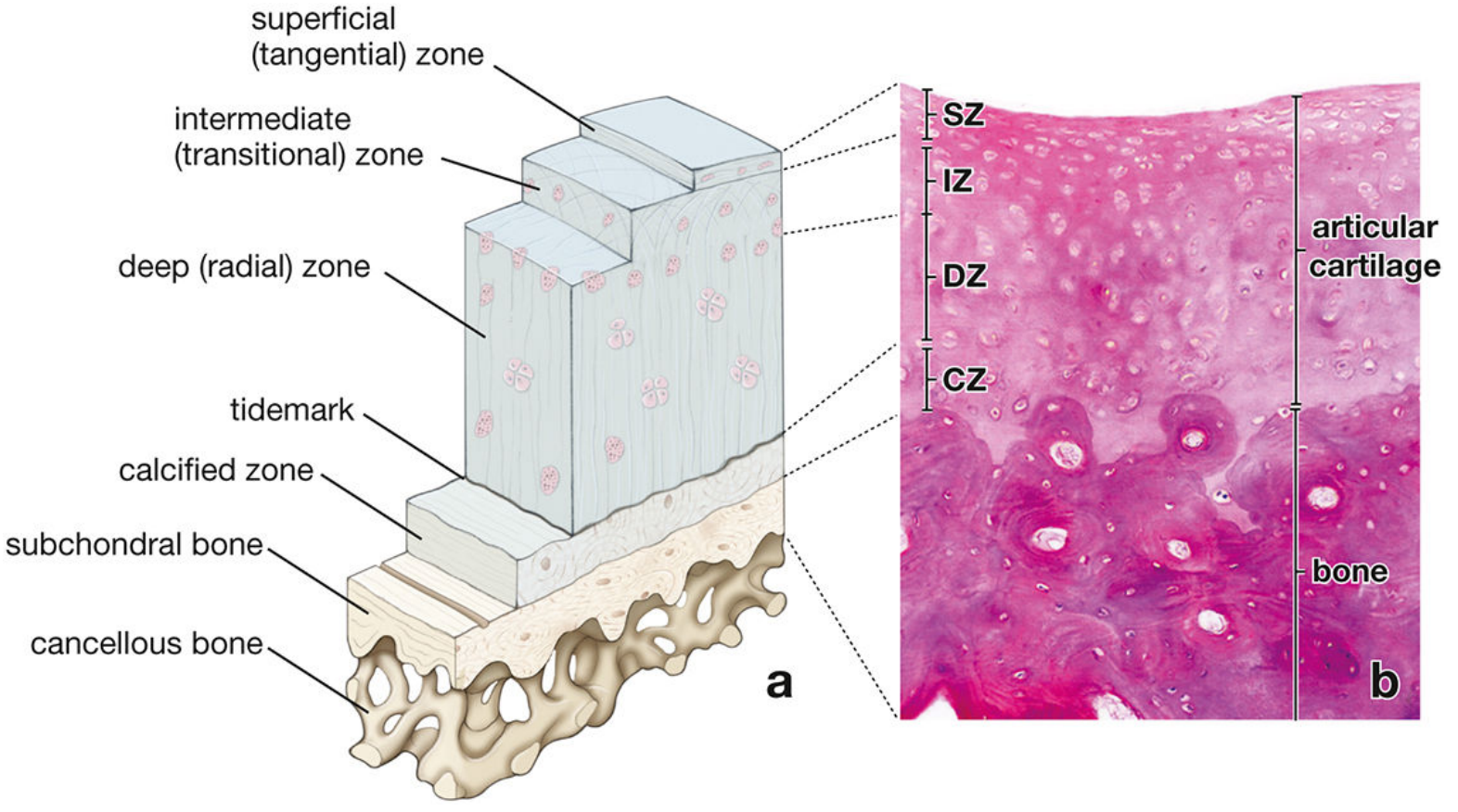
| Zone | Features |
|---|---|
| Superficial (tangential) zone | Flattened chondrocytes; collagen fibrils run parallel to the surface; pressure-resistant |
| Intermediate (transitional) zone | Round chondrocytes scattered in abundant matrix; collagen fibrils obliquely oriented |
| Deep (radial) zone | Chondrocytes in short columns perpendicular to the surface; highest proteoglycan content |
| Calcified zone | Small chondrocytes in calcified matrix; separated from deep zone by the tidemark (basophilic line); interfaces with subchondral bone |
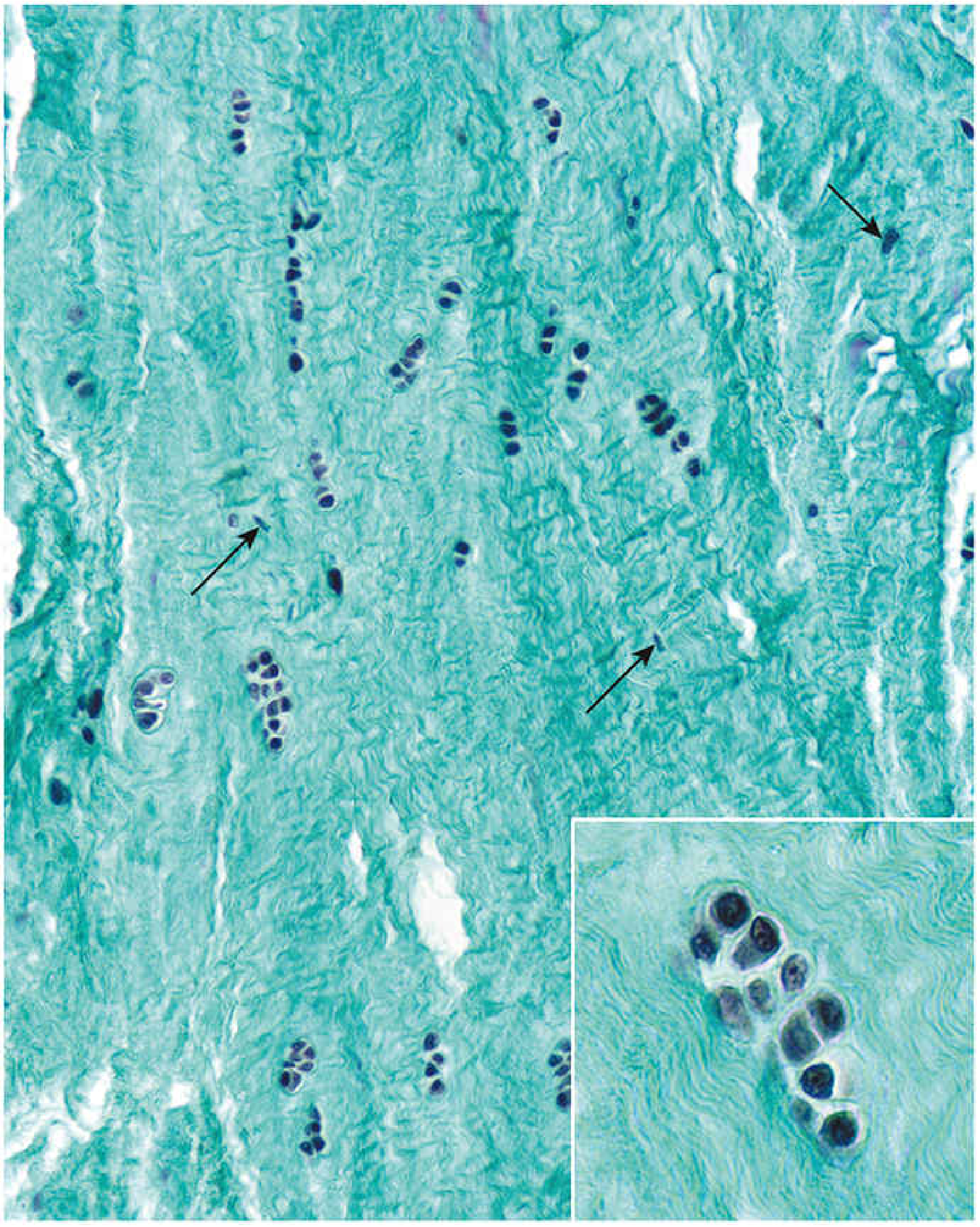
2. Elastic Cartilage
Histological appearance:
- Identical to hyaline cartilage in basic organization (chondrocytes in lacunae, isogenous groups, perichondrium present)
- Matrix additionally contains dense networks of branching and anastomosing elastic fibers and lamellae
- Elastic fibers are not visible on H&E - require special stains: orcein or resorcin-fuchsin stain them brown/dark
Locations:
- Pinna (auricle) of the external ear
- External acoustic meatus
- Eustachian (auditory) tube
- Epiglottis
- Vocal folds (corniculate and cuneiform cartilages)
Key features:
- Gives elasticity and flexibility in addition to the resilience of hyaline cartilage
- Does NOT calcify with aging (unlike hyaline cartilage)
- Has perichondrium
3. Fibrocartilage
Histological appearance:
- A combination of dense regular connective tissue + hyaline cartilage
- Chondrocytes are scattered singly, in rows, or in small isogenous groups amid thick bundles of type I collagen fibers
- Much less ground substance than hyaline cartilage
- No perichondrium
- Two cell populations visible: chondrocytes (round nuclei, small halo of amorphous matrix in lacunae) and fibroblasts (flattened/elongated nuclei within the fibrous areas)
Locations:
- Intervertebral discs (annulus fibrosus)
- Pubic symphysis
- Menisci of the knee
- Articular discs (e.g., temporomandibular, sternoclavicular joints)
- Tendon and ligament insertions (entheses)
Key features:
- Type I and type II collagen (unlike pure hyaline which is type II only)
- Resists both compression and tension - suited to sites of high mechanical stress
- Proportions of type I:type II vary by site and change with age (more type II in older individuals due to ongoing chondrocyte activity)
- No perichondrium; transitions directly into adjacent connective tissue
Summary Comparison Table
| Feature | Hyaline | Elastic | Fibrocartilage |
|---|---|---|---|
| Main collagen | Type II | Type II | Type I + II |
| Dominant proteoglycan | Aggrecan | Aggrecan | Versican > Aggrecan |
| Special matrix component | - | Elastic fibers/lamellae | Dense type I collagen bundles |
| Perichondrium | Yes (except articular/epiphyseal) | Yes | No |
| Calcification | Yes (aging, ossification) | No | Variable |
| Special stain | Alcian blue, toluidine blue (GAGs) | Orcein, resorcin-fuchsin | None specific; Masson trichrome for collagen |
| Examples | Articular surface, trachea, costal | Ear, epiglottis, Eustachian tube | IVD, menisci, pubic symphysis |
Perichondrium
A bilayer fibrous envelope surrounding hyaline and elastic cartilage:
- Outer (fibrous) layer: dense irregular connective tissue with type I collagen fibers and fibroblasts; provides tensile strength
- Inner (chondrogenic) layer: contains chondroprogenitor cells (chondroblasts) that produce new cartilage during appositional growth
Cartilage Growth
Two mechanisms:
- Appositional growth - new cartilage added at the surface by differentiation of chondroblasts from the inner perichondrium; transcription factor SOX-9 drives this differentiation
- Interstitial growth - chondrocytes divide within their lacunae and produce new matrix around themselves, expanding cartilage from within; prominent during fetal development
Repair
Cartilage has very limited repair capacity due to:
- Avascularity (no vascular inflammatory response)
- Immobility and low mitotic activity of mature chondrocytes
- Matrix as a barrier to cell migration
Minor injuries that do not penetrate the perichondrium may be repaired partially. Full-thickness injuries that reach subchondral bone recruit bone marrow mesenchymal stem cells, but these produce fibrocartilage (type I collagen) rather than the original hyaline cartilage - a mechanically inferior repair tissue.
Source: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina); Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.