Icu infections in hivpatients
Reading File
Finding Sources
Finding Sources
Searching PubMed
"HIV" AND "ICU" AND "infections"
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"HIV" AND "intensive care unit" AND "mortality"
Reading File
Finding Sources
Finding Sources
Reading File
Searching the Web
HIV ICU infections management opportunistic infections critical care 2024
Now I have comprehensive information. Let me compile a thorough, well-structured answer.
ICU Infections in HIV/AIDS Patients
HIV-infected patients admitted to the ICU present a unique challenge: they are susceptible to both common ICU pathogens AND HIV-specific opportunistic infections (OIs). The CD4+ T-cell count is the single most important factor guiding which pathogens to suspect.
CD4 Count as the Roadmap
| CD4 Count (cells/μL) | Likely Pathogens |
|---|---|
| >500 | Mostly common bacterial pathogens (similar to immunocompetent) |
| 200-500 | TB, recurrent bacterial pneumonia, herpes zoster |
| 100-200 | Pneumocystis jirovecii (PCP), Toxoplasma (CNS) |
| 50-100 | Cryptococcus, CMV disease, disseminated histoplasmosis |
| <50 | Disseminated MAC, CMV retinitis/colitis, disseminated fungal infections |
1. Respiratory Infections (Most Common ICU Admission Cause)
Pneumocystis jirovecii Pneumonia (PCP)
- Most common OI leading to ICU admission in HIV patients
- Occurs almost exclusively at CD4 <200 cells/μL
- Presents with: subacute progressive dyspnea, dry cough, fever, hypoxemia
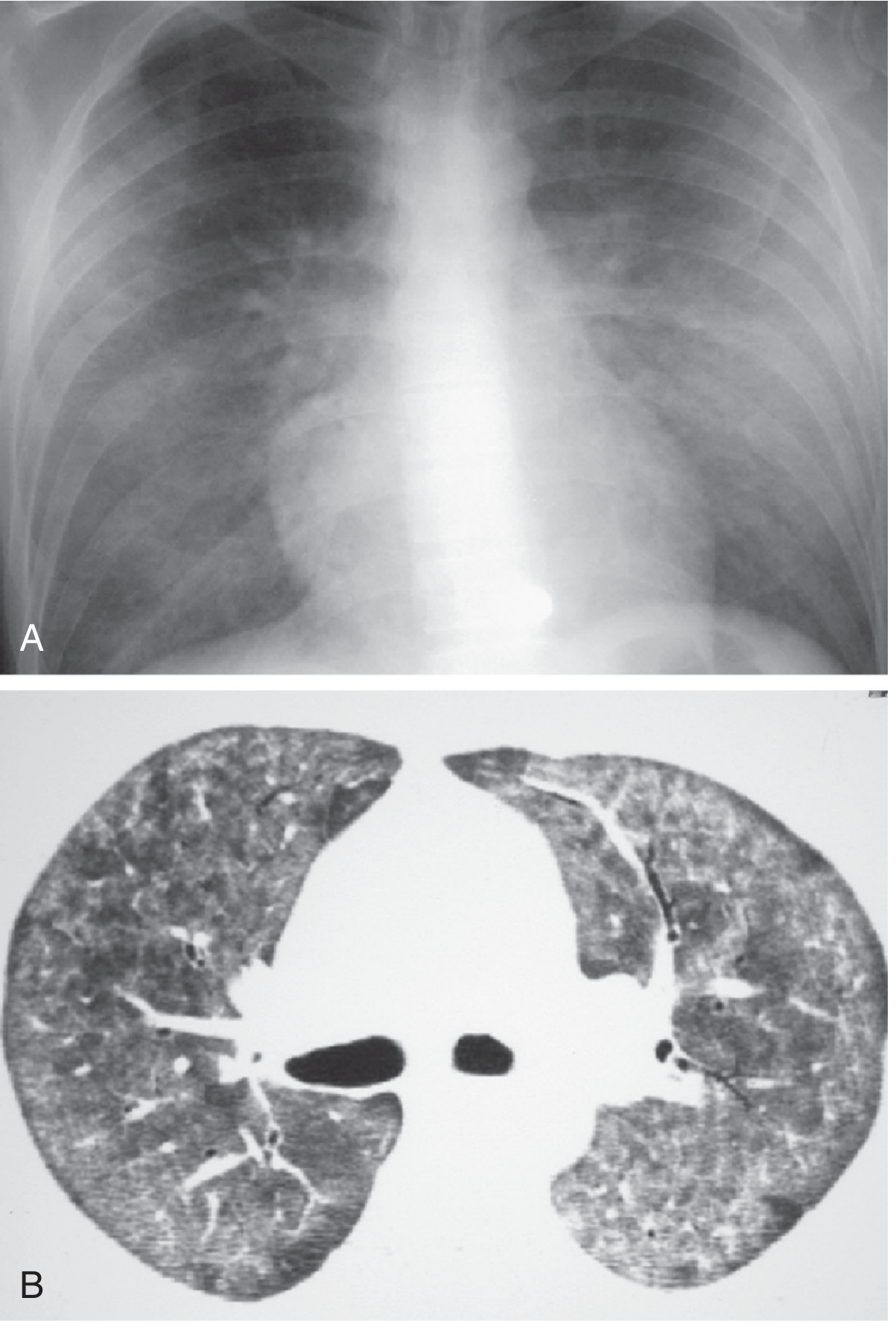
- CXR/CT: bilateral interstitial thickening and ground-glass opacities (bilateral, perihilar, classically "bat-wing" pattern); may also form pneumatoceles (thin-walled cysts) which can rupture causing pneumothorax
- Diagnosis: BAL with silver or Giemsa stain, immunofluorescence, or PCR
- Treatment: TMP-SMX (first-line) x 21 days; for severe PCP (PaO2 <70 mmHg), add adjunctive corticosteroids (prednisone 40 mg BD → taper)
- Recent RCT in Lancet Respiratory Medicine 2025 examined adjunctive corticosteroids specifically in non-AIDS patients with severe PCP - benefit appears steroid class-specific to the AIDS population per established evidence
Murray & Nadel's Textbook of Respiratory Medicine - Typical PCP appearance on CXR (bilateral, interstitial thickening with ground-glass opacities, CD4 <200):
Bacterial Pneumonia
- Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus (including MRSA), Pseudomonas aeruginosa (at low CD4)
- Recurrent bacterial pneumonia (>1 episode/year) is itself an AIDS-defining illness
- Higher risk of bacteremia compared to immunocompetent hosts
Tuberculosis (TB)
- Can occur at any CD4 count but dissemination is more likely at CD4 <200
- May present atypically: lower lobe involvement, hilar adenopathy, miliary pattern
- Miliary TB frequently causes ICU-level respiratory failure
- Key concern: drug interactions between rifampicin and antiretrovirals (especially PIs, NNRTIs)
2. CNS Infections
Cryptococcal Meningitis
- Caused by Cryptococcus neoformans - the most common life-threatening fungal infection in HIV patients; AIDS-defining illness in 40-60% of patients when diagnosed with AIDS
- Typically CD4 <100 cells/μL
- Presentation: subacute headache, fever, meningism often absent; altered consciousness if elevated ICP
- Diagnosis: India ink stain, serum/CSF cryptococcal antigen (CrAg), CSF culture
- ICP management is critical: therapeutic LPs or lumbar drain if opening pressure >25 cmH2O
- Treatment: Amphotericin B deoxycholate + flucytosine (induction 2 weeks) → fluconazole consolidation → maintenance
- Pathophysiology: polysaccharide capsule prevents phagocytosis, impairs macrophage antigen presentation, depletes complement, reduces leukocyte migration - Murray & Nadel's, p. 2648
Cerebral Toxoplasmosis
- Toxoplasma gondii reactivation at CD4 <100 cells/μL
- Presents with focal neurologic deficits, fever, seizures, altered consciousness
- CT/MRI: multiple ring-enhancing lesions (basal ganglia, corticomedullary junction), surrounding edema
- Treatment: Pyrimethamine + sulfadiazine + leucovorin (first-line); alternative pyrimethamine + clindamycin
- Maintenance therapy required until CD4 >200 cells/μL for >6 months (Adams and Victor's Neurology)
CMV Encephalitis/Meningitis
- Occurs at CD4 <50 cells/μL
- ICU intensivists should be aware: CMV is an important and often underdiagnosed pathogen in immunocompromised ICU patients (Fernandez et al., Intensive Care Med 2025)
- Treatment: Ganciclovir or foscarnet
Progressive Multifocal Leukoencephalopathy (PML)
- JC virus reactivation, CD4 <200
- Subacute demyelinating process - no effective direct treatment; ART initiation is cornerstone
3. Systemic/Bloodstream Infections
Sepsis from Bacterial Pathogens
- Recurrent Salmonella septicemia is an AIDS-defining illness
- Staphylococcus aureus bacteremia (especially MRSA) - higher in IV drug users
- Gram-negative bacteremia from enteric organisms (at lower CD4)
- Encapsulated organisms: S. pneumoniae, H. influenzae (functional hyposplenism)
Disseminated MAC (Mycobacterium avium Complex)
- Almost exclusively CD4 <50 cells/μL
- Presents with: fever, night sweats, weight loss, hepatosplenomegaly, pancytopenia
- ICU implications: can cause severe anemia, cytopenias requiring transfusion
- Treatment: Clarithromycin + ethambutol (± rifabutin)
- ART now prioritized over prophylaxis per updated 2024 NIH/IDSA guidelines
Disseminated Fungal Infections
- Histoplasma capsulatum - endemic in central/south-central US; disseminates to ICU-level disease at low CD4
- Candida - candidemia in the setting of indwelling catheters, broad-spectrum antibiotics, HIV
- Aspergillus - invasive pulmonary aspergillosis, primarily when CD4 very low or with neutropenia
4. Unique ICU Considerations in HIV Patients
Immune Reconstitution Inflammatory Syndrome (IRIS)
- Occurs when ART is started in the setting of untreated OI
- Paradoxical worsening as immune function returns
- Particularly dangerous with cryptococcal meningitis (rapidly elevated ICP) and TB
- Manage with corticosteroids in severe cases; do not stop ART unless life-threatening
When to Start ART in the ICU
- For most OIs: start ART within 2 weeks of OI treatment
- Exception: Cryptococcal meningitis - delay ART 4-6 weeks to reduce IRIS-related mortality
- Exception: TB meningitis - delay 4-8 weeks
Distinguishing OI from Non-OI Infections
In the ICU, HIV patients can still get standard ICU infections (VAP, CLABSI, C. diff). Always consider:
- What is the CD4 count? (rules in/out OI spectrum)
- Is the patient on ART? What is the viral load?
- Has OI prophylaxis (TMP-SMX, azithromycin, fluconazole) been given?
Drug Interactions
- Rifampicin dramatically reduces PI and NNRTI levels - use rifabutin instead if possible
- Fluconazole inhibits CYP3A4 - watch for toxicity with many antiretrovirals
- TMP-SMX can cause hyperkalemia, elevated creatinine (inhibits tubular secretion) - not true AKI
5. Prophylaxis Summary (NIH/IDSA/HIVMA 2024 Guidelines)
| CD4 Threshold | Primary Prophylaxis |
|---|---|
| <200 cells/μL | TMP-SMX for PCP (and toxoplasmosis if IgG+) |
| <150 cells/μL | Fluconazole for cryptococcosis (in endemic settings) |
| <250 cells/μL (in endemic area) | Fluconazole for coccidioidomycosis |
| <50 cells/μL (not on ART) | Azithromycin for MAC |
| Any CD4, TB exposure | Isoniazid preventive therapy |
Prophylaxis can be safely discontinued once CD4 recovers on ART above relevant thresholds with sustained virologic suppression, per the updated NIH OI Guidelines (2024/2026).
Summary: Approach to an HIV Patient with Infection in the ICU
- Determine CD4 count - this stratifies the entire differential
- Check ART status and viral load - undetectable viral load on ART makes most OIs less likely
- Obtain broad workup early: blood cultures, CrAg (serum), BAL, LP if CNS features, CMV PCR, TB workup
- Empirically cover PCP if hypoxic + CD4 <200 (TMP-SMX + steroids if severe)
- Empirically cover bacterial sepsis with broad-spectrum antibiotics while awaiting cultures
- Beware of IRIS if starting ART during active OI
- Involve infectious disease early for ART timing, drug interactions, and OI-specific management
This is a shared conversation. Sign in to Orris to start your own chat.