Senile Macular DegenerationSenile Macular Degeneration
Reading File
Finding Sources
Finding Sources
Searching PubMed
"age-related macular degeneration"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have rich content from multiple authoritative sources. Let me compile the comprehensive answer:
Senile (Age-Related) Macular Degeneration (AMD / ARMD)
Definition & Epidemiology
Age-related macular degeneration (AMD) - also called senile macular degeneration - is a progressive neurodegenerative disease that primarily affects the retinal pigment epithelium (RPE) of the macula, typically presenting in the sixth to ninth decades of life. It is the most common cause of blindness in older individuals in industrialized countries, accounting for approximately 8.5% of the world's blindness. In the United States alone, more than 1.75 million persons are affected, and prevalence increases with each decade after age 55.
- Goldman-Cecil Medicine, p. 662
- Histology: A Text and Atlas (Eroschenko), p. 2402
Anatomy Involved
The pathological changes center on a structural and functional unit comprising:
- Retinal Pigment Epithelium (RPE) - nourishes photoreceptors
- Bruch membrane - basement membrane of the RPE
- Choriocapillaris - innermost layer of choroidal vasculature
Disturbance to any component damages overlying photoreceptors and causes vision loss.
Classification: Two Major Forms
1. Dry (Atrophic / Non-exudative) AMD - ~90% of cases
The most common form. Characterized by:
- Drusen - focal thickenings/abnormal lipoprotein deposits within the RPE basement membrane complex (Bruch membrane); soft drusen >60 μm are most significant
- Geographic atrophy - well-defined pigment loss and RPE atrophy
- Lipofuscin accumulation in stressed RPE cells (oxidation products of polyunsaturated fatty acids and vitamin A dimers)
- Obliteration of capillaries in the underlying choroid
Progression is slow (months to decades). May precede subjective visual change by years to decades.
2. Wet (Exudative / Neovascular) AMD - ~10% of cases
Considered a complication of dry AMD. Characterized by:
- Choroidal neovascularization (CNV) - frail new vessels from choriocapillaris penetrate through a breach in Bruch membrane into the subretinal space
- These thin, fragile vessels leak producing exudates, subretinal hemorrhage, and intraretinal fluid
- Progresses to fibrosis and scarring with rapid, severe central vision loss
- Responsible for the most profound vision loss, especially if untreated
Dry and wet AMD may coexist; dry AMD is not always a precursor to wet AMD - each can develop through distinct pathways.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1221
- Histology: A Text and Atlas, p. 2402
Dry vs. Wet AMD Diagram (Robbins)
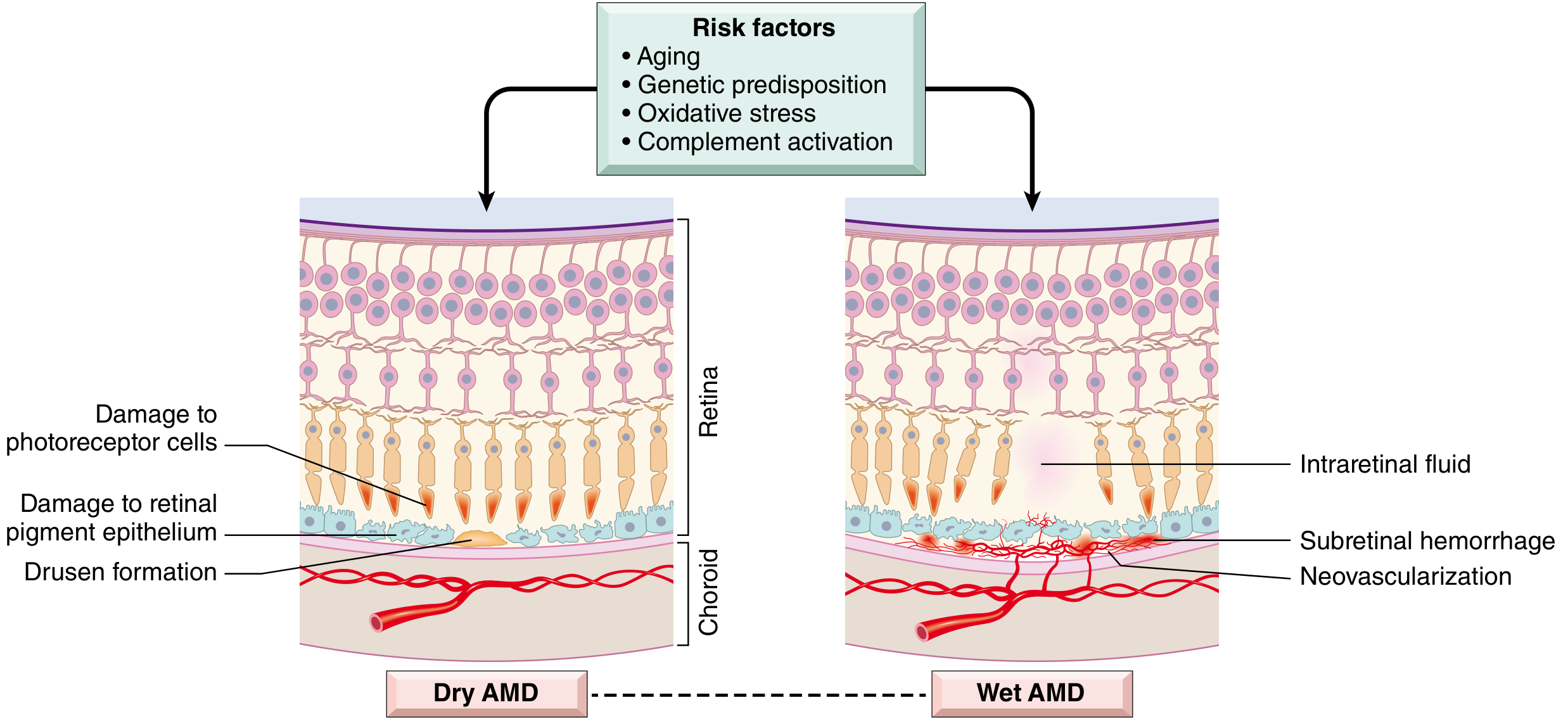
Schematic comparing Dry AMD (drusen, RPE damage, photoreceptor loss) vs Wet AMD (neovascularization, subretinal hemorrhage, intraretinal fluid). Risk factors: aging, genetic predisposition, oxidative stress, complement activation.
Fundus Appearance
Dry AMD - Fine drusen (fundus photograph):
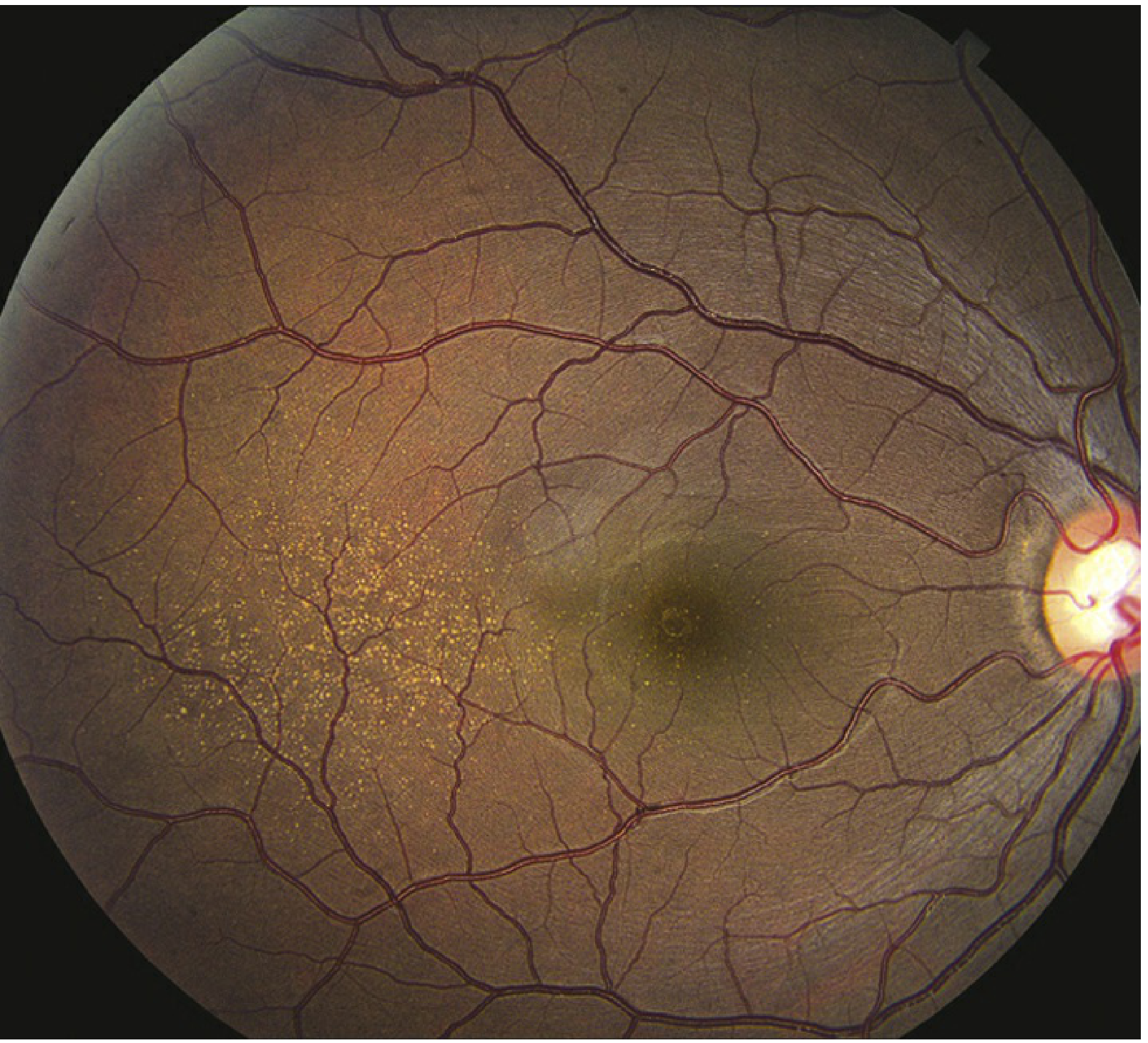
Note the scattered yellow-white drusen deposits in the macular region with surrounding normal retina and visible optic disc.
Histopathology
Wet AMD - Histology of neovascular membrane (Robbins):
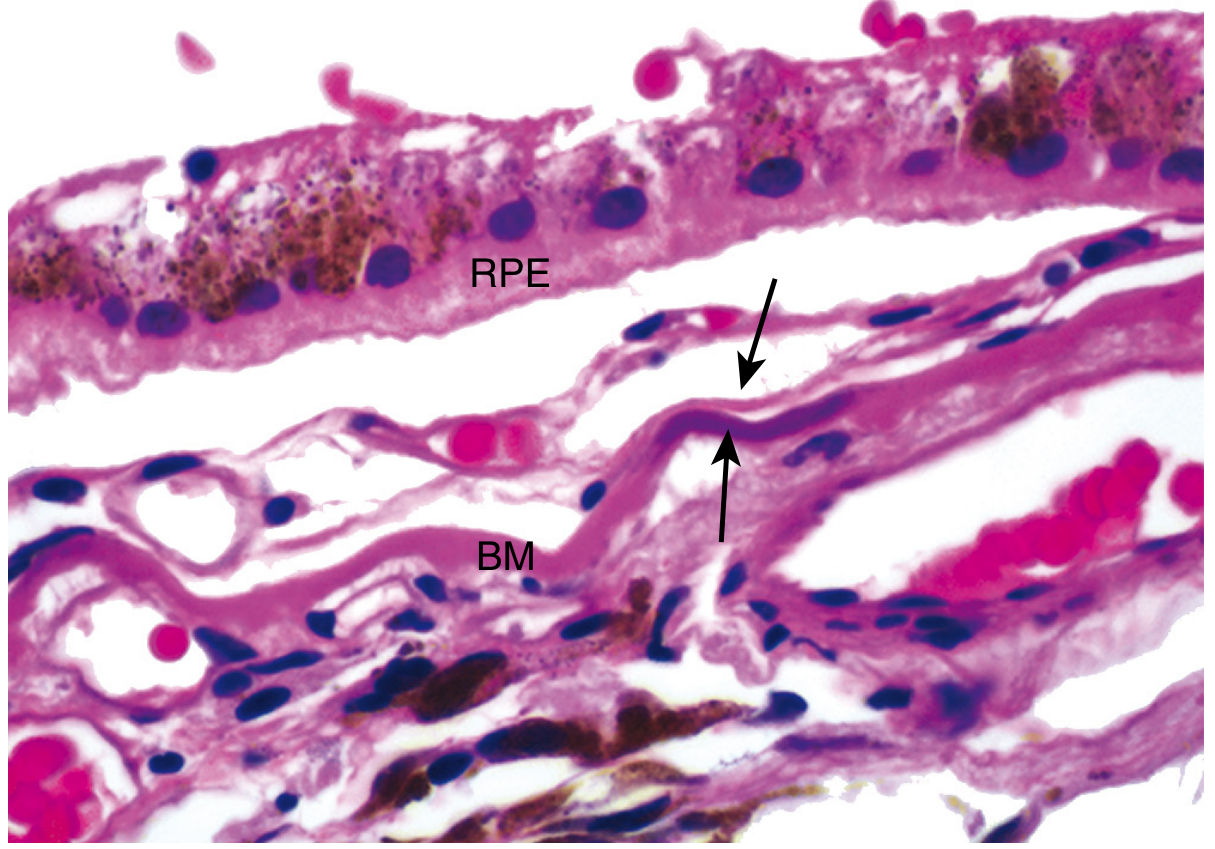
A neovascular membrane is positioned between the retinal pigment epithelium (RPE) and Bruch membrane (BM). Arrows indicate focal calcification (blue discoloration) of BM.
Pathogenesis
Genetic Factors
- CFH (Complement Factor H), Complement Factor I (CFI), and other complement regulatory gene polymorphisms are strongly associated with AMD
- These suggest AMD stems partly from excess complement activation, injuring photoreceptors
- ARMS2 gene polymorphisms also confer increased risk
- Therapy targeting complement may slow geographic atrophy progression
Environmental Factors
- Cigarette smoking - increases risk 2- to 3-fold; the single most modifiable risk factor; dose-dependent
- Ultraviolet (UV) irradiation and oxidative stress
- Poorly controlled hypertension, hyperlipidemia, diabetes
Pathological Sequence (Dry AMD)
Oxidative stress → RPE dysfunction → Lipofuscin accumulation → Drusen formation → Complement activation → Chronic inflammation → Geographic atrophy → Photoreceptor death
Pathological Sequence (Wet AMD)
Drusen/geographic atrophy → Breach in Bruch membrane → VEGF upregulation → Choroidal neovascularization → Vessel leakage + hemorrhage → Scarring → Rapid central vision loss
- Robbins, Cotran & Kumar, p. 1222
Clinical Features
Symptoms
| Feature | Dry AMD | Wet AMD |
|---|---|---|
| Onset | Slow, insidious | Acute to subacute |
| Central vision | Gradually reduced | Acute severe loss |
| Scotoma | Present (late) | Central/paracentral |
| Metamorphopsia | Rare | Common (wavy lines) |
| Photopsias | Absent | May be present |
| Peripheral vision | Preserved | Preserved |
Classic description: A patient can walk down a street without difficulty (peripheral retinal function) but cannot recognize facial features of people they encounter (macular function). - Goldman-Cecil Medicine
Signs on Examination
- Macular drusen (critical sign in both forms)
- Clumps of pigment in outer retina
- RPE atrophy (almost always bilateral)
- Geographic atrophy (confluent choriocapillaris atrophy)
- In wet AMD: subretinal fluid, hemorrhage, exudate, CNV membrane
Visual Field Defect

Simulated photo showing central visual field loss (black scotoma centrally) with preserved peripheral vision - characteristic of macular disease. Patients are instructed to use eccentric fixation.
Diagnosis & Workup
- Amsler grid testing - detects metamorphopsia (distortion), indicates CNV development; home monitoring also via PHP (ForseeHome device)
- Dilated fundus examination - drusen, RPE changes, atrophy
- Fluorescein angiography (FA) - identifies CNV in wet AMD
- Optical Coherence Tomography (OCT) - gold standard for detecting subretinal/intraretinal fluid; defines extent of CNV
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Peripheral drusen | Drusen outside macular area only |
| Myopic degeneration | Peripapillary changes, no drusen |
| CSCR | Age <50, serous elevation, no drusen/hemorrhage |
| Stargardt disease | Age <50, familial, lipofuscin accumulation |
| Chloroquine toxicity | Bull's-eye maculopathy, drug history |
| Multifocal choroiditis | Vitreous cells, no drusen |
Treatment
Dry AMD
- No curative treatment exists
- AREDS/AREDS2 formula (Age-Related Eye Disease Study) supplementation for moderate-to-advanced dry AMD:
- Vitamin C, Vitamin E, Zinc, Copper
- Lutein + Zeaxanthin (replaced beta-carotene in AREDS2)
- Note: Beta-carotene avoided in smokers (increased lung cancer risk)
- High dietary omega-3 fatty acids (cold-water fish, nuts)
- Cessation of smoking is the most important modifiable intervention
- Control of blood pressure, blood sugar, blood lipids
- Complement-targeting therapies are in development for geographic atrophy
- iPSC-derived RPE cell replacement therapy - experimental; surgical insertion of RPE-seeded biofilm into subretinal space (early trials in Japan)
- Low-vision aids, special glasses, video magnification aids
Wet AMD - Anti-VEGF Therapy (Mainstay)
Intravitreal injections targeting VEGF reduce the risk of visual loss and can achieve gains in vision when administered promptly:
| Drug | Mechanism |
|---|---|
| Ranibizumab (Lucentis) | Anti-VEGF antibody fragment |
| Bevacizumab (Avastin) | Full anti-VEGF antibody (off-label) |
| Aflibercept (Eylea) | VEGF trap (soluble decoy receptor) |
| Faricimab (Vabysmo) | Dual inhibitor of Ang-2 and VEGF-A |
Other Treatments for Wet AMD
- Photodynamic therapy (PDT) - verteporfin activated by laser; for subfoveal CNV
- Laser photocoagulation - for extrafoveal CNV (destroys pathologic vessels); risks scotoma
- Macular translocation surgery - retina detached, translocated, reattached away from CNV tissue; for advanced cases
Monitoring & Follow-Up
-
Dry AMD: Follow every 6-12 months; daily Amsler grid self-monitoring; return immediately if new distortion or visual change develops (may indicate conversion to wet AMD)
-
Wet AMD: Monitoring interval tailored to treatment response; OCT-guided injection schedules (treat-and-extend, PRN)
-
Wills Eye Manual, p. 832-837
-
Goldman-Cecil Medicine, p. 672-674
Key Points Summary
| Feature | Details |
|---|---|
| Cause | Multifactorial - aging, genetic (CFH), environmental |
| Prevalence | >1.75 million in USA; #1 cause of blindness in elderly (developed world) |
| Onset | 6th-9th decade |
| Vision loss type | Central only; peripheral preserved |
| Dry AMD | 90%, drusen + geographic atrophy, slow progression |
| Wet AMD | 10%, CNV, rapid severe vision loss |
| Key pathology | RPE degeneration, Bruch membrane changes |
| First-line Rx (wet) | Intravitreal anti-VEGF injections |
| Dry AMD Rx | AREDS2 supplements, lifestyle modification |
| Monitoring | Amsler grid, OCT, fluorescein angiography |
Sources: Goldman-Cecil Medicine (2025), Robbins Cotran & Kumar Pathologic Basis of Disease, Histology: A Text and Atlas (Eroschenko), Wills Eye Manual, Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.