Emphysema
Reading File
Finding Sources
Searching PubMed
emphysema pathophysiology treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive material for a thorough answer. Let me compile everything.
Emphysema
Definition
Emphysema is defined as permanent, irreversible enlargement of airspaces distal to the terminal bronchioles, accompanied by destruction of alveolar walls, without significant fibrosis. It is a major component of COPD alongside chronic bronchitis.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 635
Types (Anatomic Classification)
There are four types, classified by which part of the acinus is destroyed:
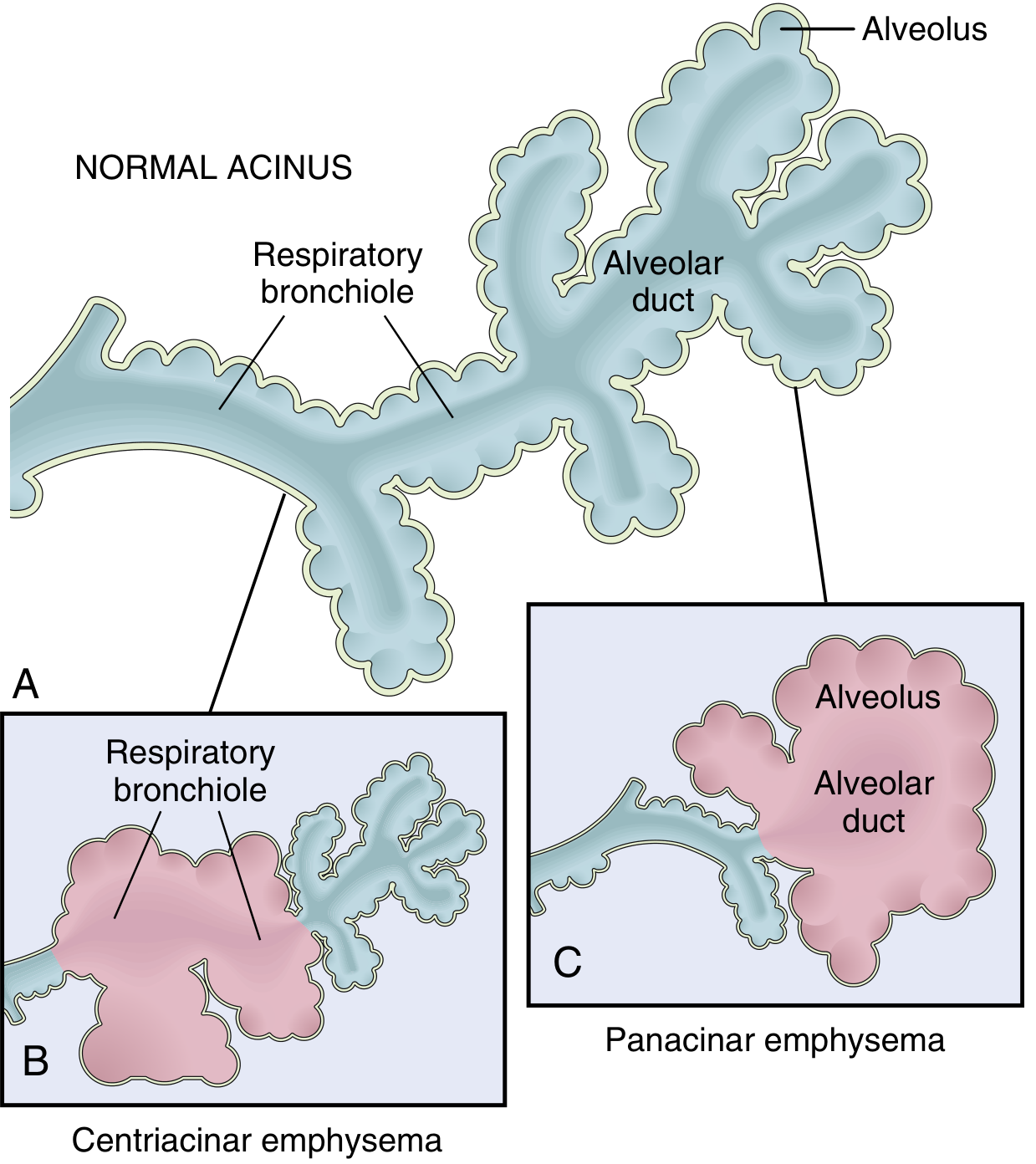
Fig: Major patterns of emphysema showing the normal acinus (A), centriacinar emphysema with dilation of respiratory bronchioles (B), and panacinar emphysema with uniform distension of the alveolus and alveolar duct (C). - Robbins Basic Pathology
| Type | Location of destruction | Association | Distribution |
|---|---|---|---|
| Centriacinar (centrilobular) | Central/proximal acinus (respiratory bronchioles); distal alveoli spared | Smoking - most common (>95% of cases) | Upper lobes, apical segments |
| Panacinar (panlobular) | Entire acinus uniformly enlarged | α1-antitrypsin deficiency; worsened by smoking | Lower lobes, anterior margins |
| Distal acinar (paraseptal) | Distal part of acinus, near pleura/septa | Spontaneous pneumothorax in young adults; bulla formation | Upper half of lungs, subpleural |
| Irregular (paracicatricial) | Irregular, associated with scarring | Usually clinically insignificant | Around scars |
Only centriacinar and panacinar types cause clinically significant airflow obstruction.
Pathogenesis
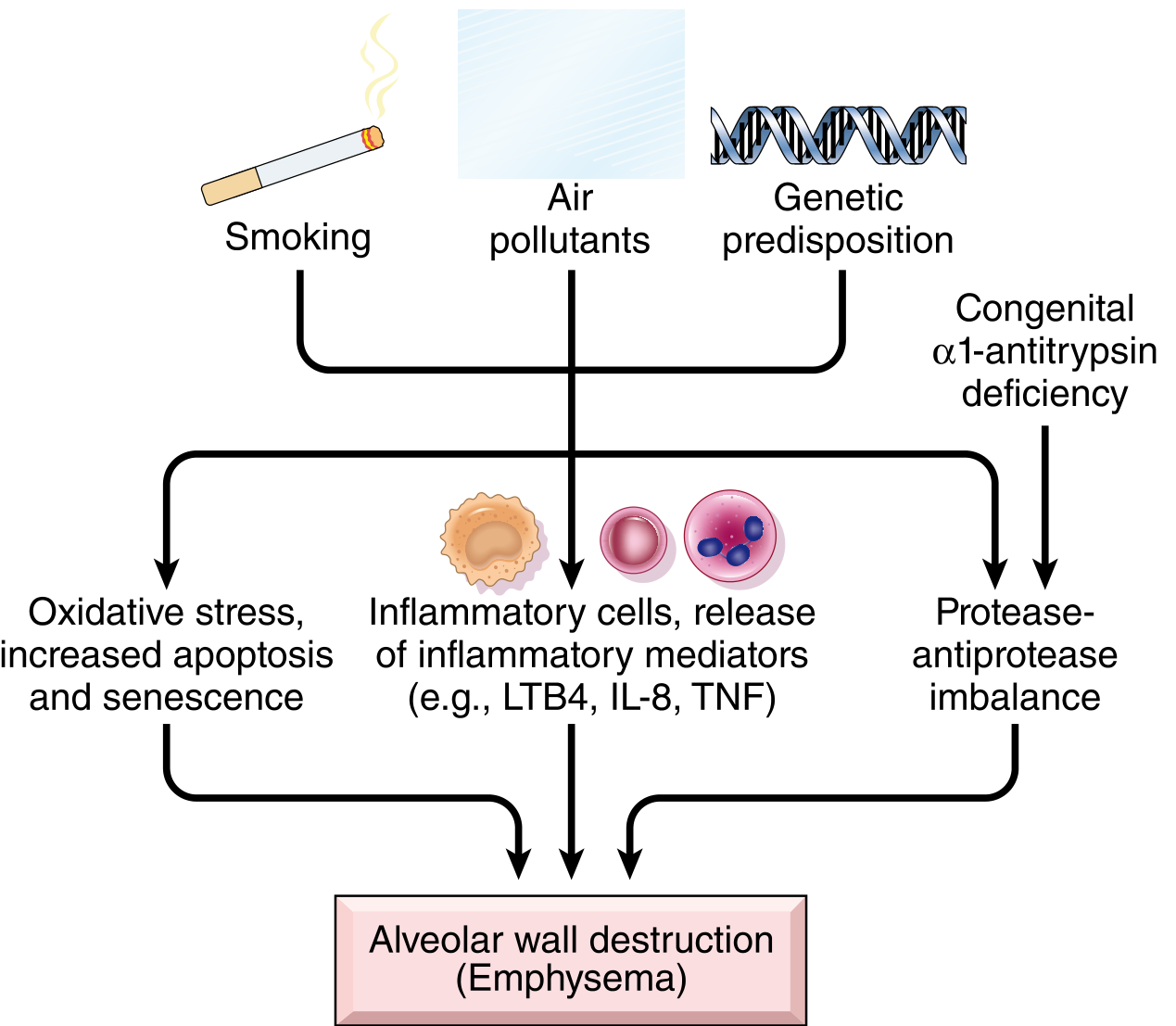
Fig: Pathogenesis of emphysema - Robbins, Cotran & Kumar
Four key mechanisms converge on alveolar wall destruction:
1. Toxic Injury and Inflammation
Inhaled smoke/noxious particles damage respiratory epithelium and trigger chronic inflammation. Mediators released include leukotriene B4 (LTB4), IL-8, and TNF, which recruit neutrophils, macrophages, and lymphocytes. These cells cause parenchymal destruction.
2. Protease-Antiprotease Imbalance
Inflammatory cells release proteases (especially neutrophil elastase) that break down connective tissue (elastin, collagen). Normally, α1-antitrypsin (AAT) neutralizes these proteases. When AAT is deficient (genetically - PiZZ allele on chromosome 14) or overwhelmed, the balance tips toward destruction. About 1% of emphysema patients have AAT deficiency.
3. Oxidative Stress
Tobacco smoke and inflammatory cells generate reactive oxygen species (ROS), which cause tissue damage and endothelial dysfunction. The NRF2 transcription factor (encoded by NFE2L2) is a key antioxidant sensor - mice without NRF2 are far more susceptible to smoke-induced lung disease.
4. Infection
Bacterial/viral infections do not initiate emphysema but can acutely exacerbate existing disease.
- Robbins, Cotran & Kumar, p. 636
Morphology
Grossly: Lungs are pale, voluminous, and hyperinflated. Bullae may be visible on cut section. In centriacinar emphysema, enlarged airspaces cluster centrally within lobules. In panacinar emphysema, the entire lobule is uniformly enlarged and the lung takes on a "foam-like" appearance.
Histologically: Alveolar wall loss with enlarged, irregular airspaces. Reduced surface area for gas exchange. The alveolar septa are thinned and may show inflammatory cells. Vascular bed is reduced.
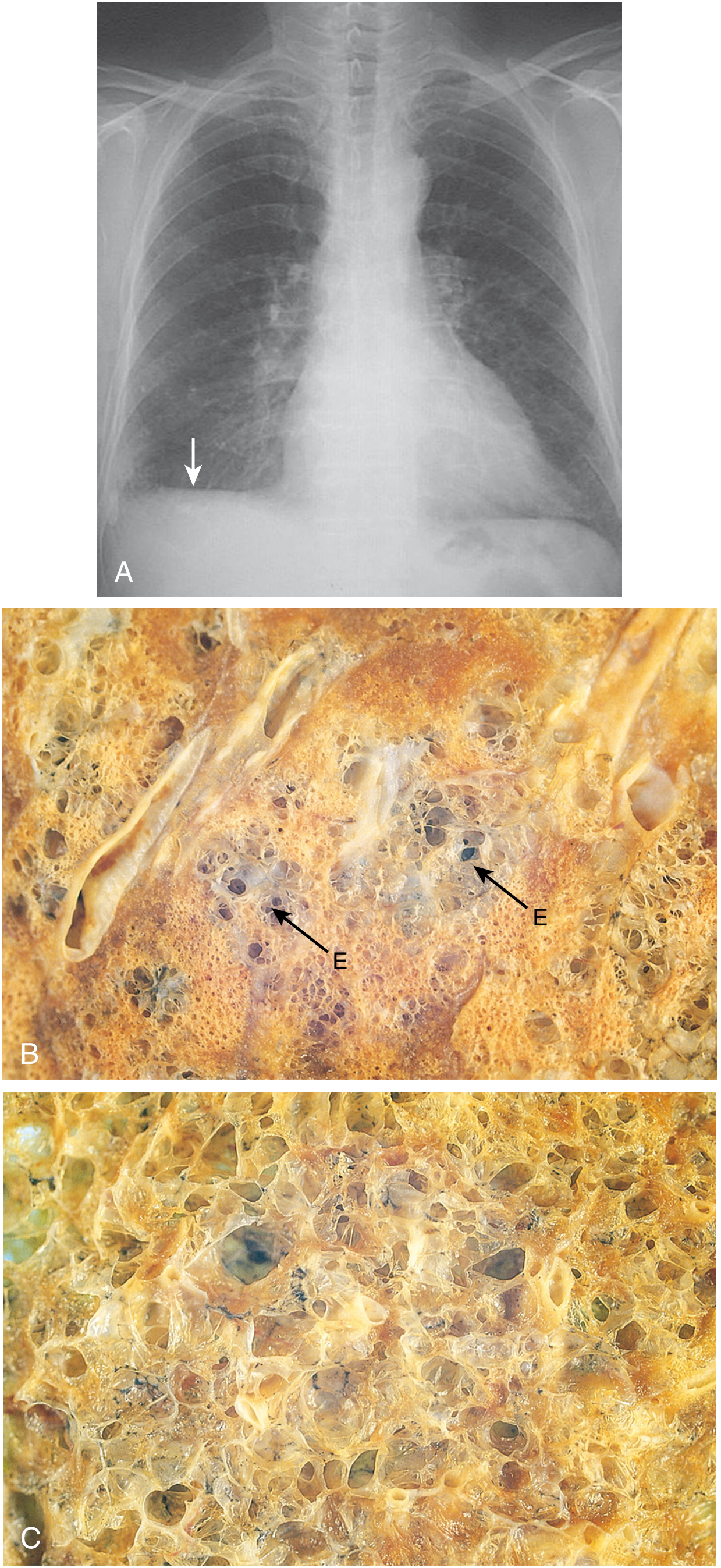
Fig: (A) Chest X-ray of advanced emphysema with flattened diaphragm. (B) Centriacinar emphysema - "E" marks enlarged centrally-placed spaces. (C) Panacinar emphysema - uniform enlargement throughout the lobule. - Robbins, Cotran & Kumar
Clinical Features
Symptoms typically appear after 40+ pack-years of smoking. COPD with emphysema as the dominant component presents as:
Classic "Pink Puffer" (emphysema-dominant):
- Progressive exertional dyspnea, often severe
- Barrel chest (increased AP diameter)
- Prolonged expiration through pursed lips
- Sitting forward in a hunched position
- Minimal cough/sputum
- Severe lung overdistension
- Blood gases relatively normal at rest (maintained by hyperventilation)
- Low diffusing capacity (DLCO)
- Weight loss (common, can be severe - cardiac cachexia-like)
Contrast with "Blue Bloater" (chronic bronchitis-dominant):
- Productive cough, copious sputum
- Cyanosis, CO2 retention
- Cor pulmonale more common
Most patients fall somewhere along this spectrum.
Spirometry: FEV1/FVC ratio < 0.7 (obstructive pattern). Air trapping causes increased total lung capacity (TLC) and residual volume (RV).
Complications:
- Pulmonary hypertension and cor pulmonale
- Respiratory failure
- Spontaneous pneumothorax (especially paraseptal type)
- Secondary polycythemia
α1-Antitrypsin (AAT) Deficiency
- Encoded at the Pi (proteinase inhibitor) locus, chromosome 14
- PiZZ homozygotes have markedly reduced serum AAT (~15% of normal)
- Leads to panacinar emphysema, predominantly in lower lobes
- Smoking dramatically accelerates disease
- Also associated with neonatal hepatitis and cirrhosis (misfolded AAT accumulates in hepatocytes)
- AAT augmentation therapy is available for confirmed deficient patients
Imaging
- Chest X-ray: Hyperinflation, flattened diaphragms, increased retrosternal space, reduced vascular markings ("pruning"), bullae
- HRCT chest: Most sensitive; shows low-attenuation areas without visible walls. Can quantify distribution and severity. Centrilobular emphysema appears as small rounded lucencies without walls around the central artery of secondary lobules.
Management Overview
Treatment is largely the same as for COPD broadly:
| Category | Approach |
|---|---|
| Smoking cessation | Most important disease-modifying intervention |
| Bronchodilators | SABAs, SAMAs; long-acting: LABAs + LAMAs |
| Inhaled corticosteroids | Added for frequent exacerbators (combined with LABA) |
| Pulmonary rehabilitation | Improves exercise tolerance and quality of life |
| Oxygen therapy | If PaO2 < 55 mmHg or SpO2 ≤ 88%; shown to improve survival |
| Lung volume reduction | Surgical (LVRS) or bronchoscopic (endobronchial valves, coils) for selected severe cases |
| AAT augmentation | Weekly IV infusion for documented PiZZ deficiency |
| Lung transplantation | End-stage disease |
Recent evidence on lung volume reduction: A 2025 systematic review and network meta-analysis (Bo et al., COPD 2025, PMID 41037331) compared bronchoscopic lung volume reduction therapies (endobronchial valves, coils, vapor ablation) in emphysema patients, supporting the efficacy of endobronchial valve placement in appropriately selected patients with heterogeneous emphysema and intact interlobar fissures. A 2025 review (Ter Haar et al., Eur Respir Rev, PMID 40174955) also documented extrapulmonary benefits of lung volume reduction (improved cardiac function, reduced pulmonary hypertension).
Key Summary Points
- Emphysema = alveolar wall destruction + permanent airspace enlargement (no fibrosis)
- Centriacinar (smoking) is far more common than panacinar (AAT deficiency)
- Mechanism: protease-antiprotease imbalance + oxidative stress + inflammation
- "Pink puffer" phenotype: dyspnea-dominant, hyperventilating, maintaining O2 at rest
- Irreversible but progression slowed by smoking cessation; bronchoscopic/surgical lung volume reduction is an option in severe disease
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.