Periosteal reaction
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I have all the information needed to write a comprehensive answer. Let me compile it now.
Periosteal Reaction
A periosteal reaction is the bone-forming response of the periosteum to any stimulus that elevates or irritates it - whether infection, trauma, tumour, or systemic disease. The periosteum contains osteoblast precursors that, when activated, lay down new bone on the cortical surface. Mineralization takes 10 days to 3 weeks after the insult before it becomes visible on plain radiography; CT can detect it earlier, and MRI shows both mineralized and non-mineralized components.
On MRI:
- Mineralized periosteal reaction = signal void on all sequences
- Subperiosteal tissue = isointense T1, hyperintense T2, enhances with gadolinium
Classification by Pattern (and Aggressiveness)
No single pattern is pathognomonic, but the pattern strongly indicates the rate of growth and aggressiveness of the underlying process.
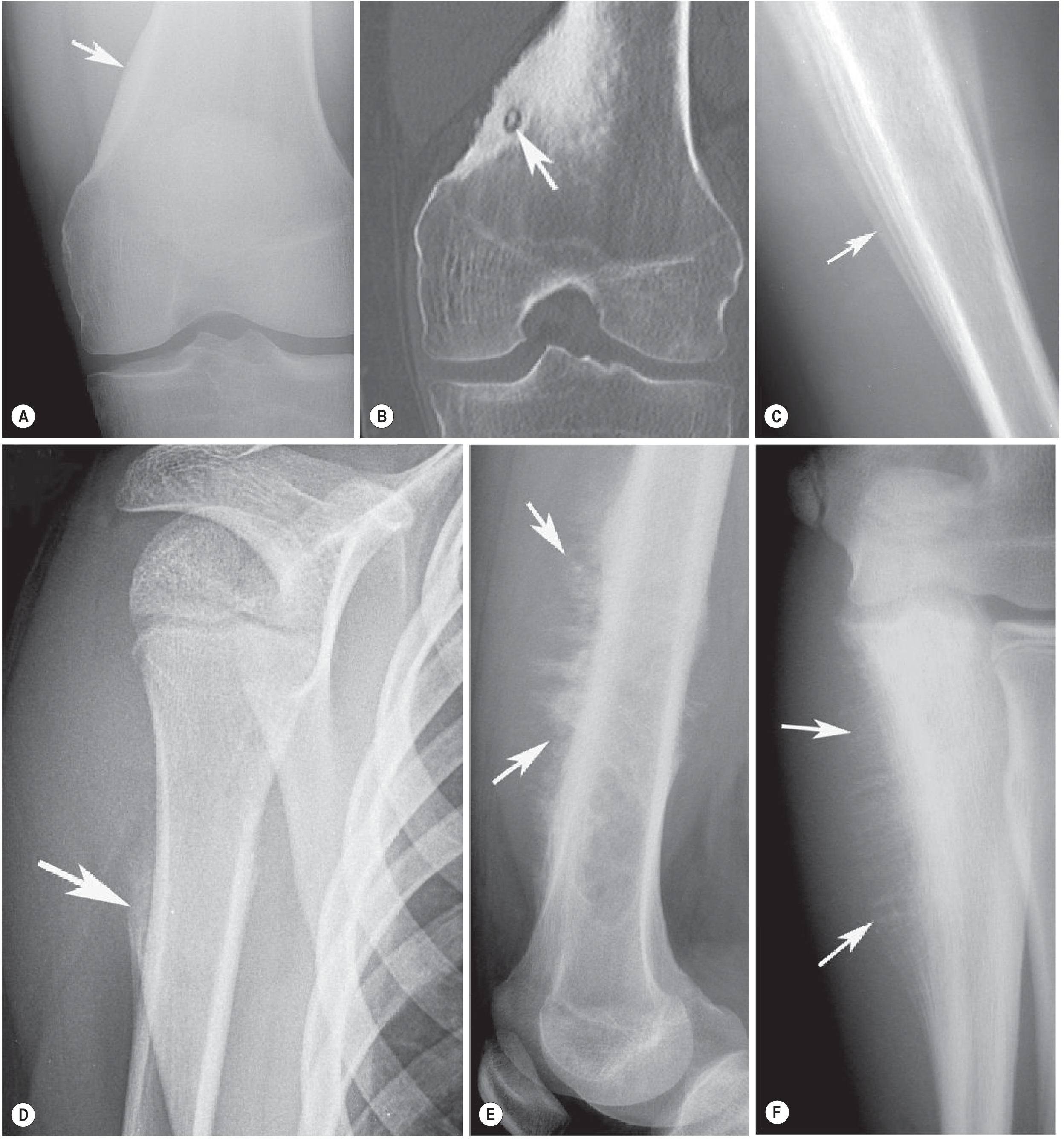
1. Solid (Non-aggressive)
- Appearance: Thick, uniform, well-formed single layer of new bone fused to the cortex
- Mechanism: Slow, successive deposition of compact lamellar bone; periosteal layers fuse over time
- Indicates: Slow-growing, chronic, non-aggressive process
- Causes: Stress fractures, medial tibial stress syndrome (shin splints), adductor insertion avulsion syndrome, osteoid osteoma, grade 2 chondrosarcoma
- Note: A solid reaction does not guarantee benignity
2. Lamellated / Multilaminated ("Onion-Skin") (Intermediate aggression)
- Appearance: Multiple parallel layers of periosteal new bone, like concentric rings of an onion
- Mechanism: Periodic or episodic growth causes successive lifting of the periosteum with new bone laid down in each cycle
- Indicates: Intermediate aggressiveness - subperiosteal extension of tumour, infection, or haematoma
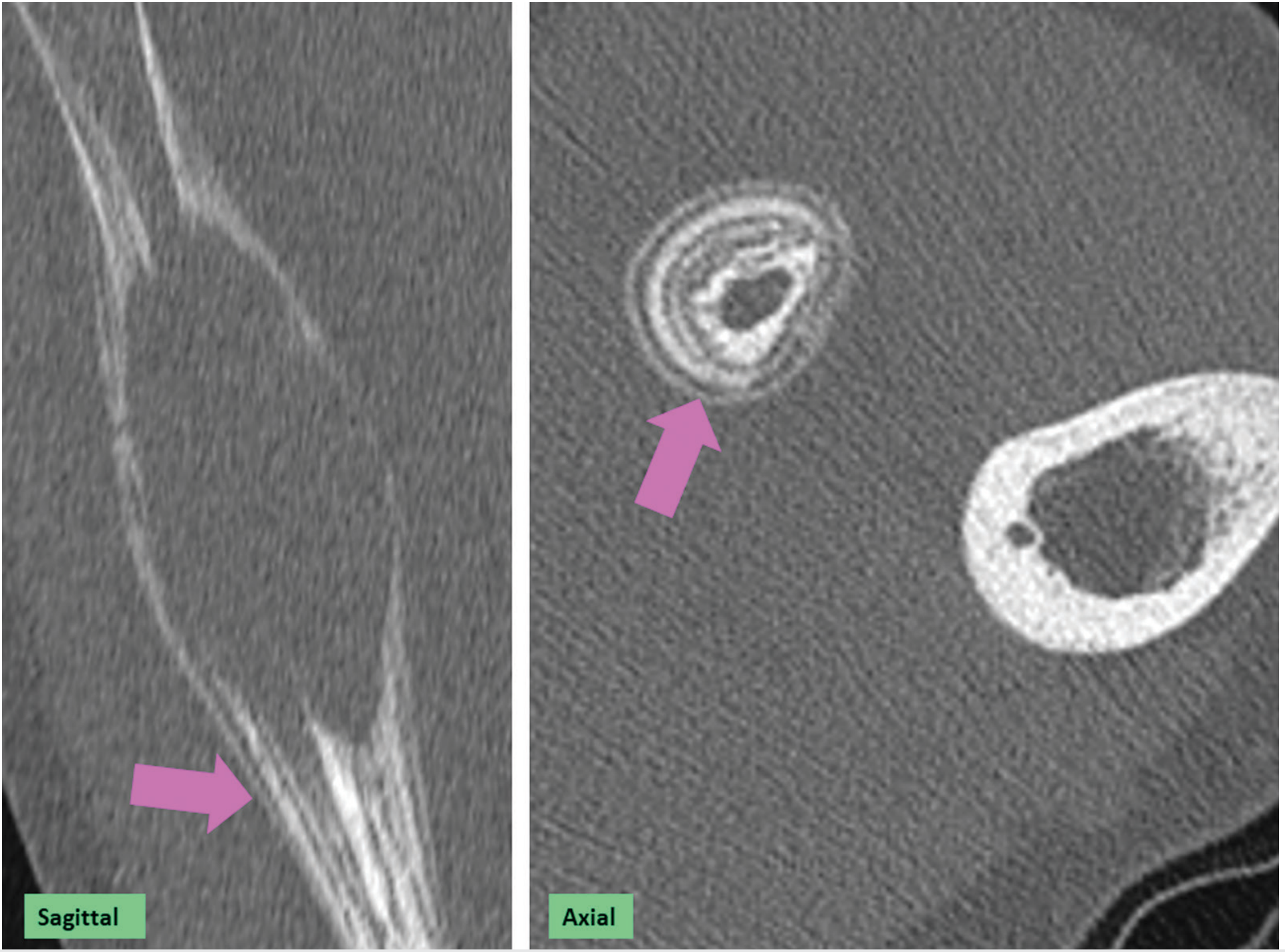
- Classic causes: Ewing sarcoma (most classic), acute osteomyelitis, some benign masses (aneurysmal bone cyst)
3. Codman Triangle (Aggressive)
- Appearance: A triangular shell of reactive periosteal bone at the margin of the lesion, where the periosteum has been lifted and interrupted by the rapidly growing process. It represents the edge of subperiosteal tumour extension in the longitudinal direction.
- Mechanism: Tumour grows so fast it breaks through the periosteum, leaving a triangular residual shell at the proximal/distal limit
- Indicates: Rapidly evolving, aggressive process
- Classic causes: Osteosarcoma (most classic), Ewing sarcoma; not specific to any one tumour
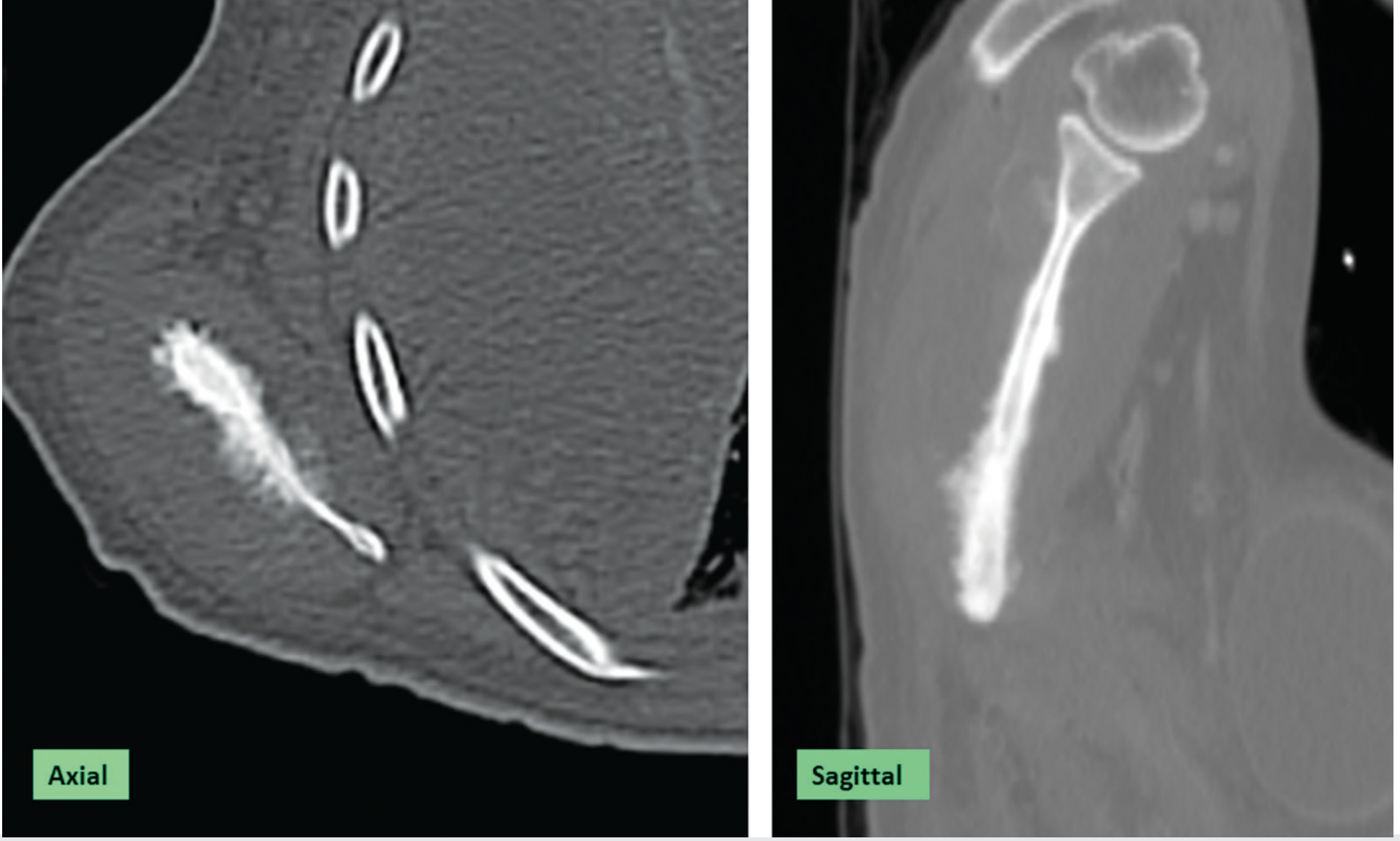
4. Spiculated - Sunburst / Hair-on-End (Most aggressive)
- Appearance:
- Sunburst: coarse, diverging spicules radiating outward from the cortex
- Hair-on-end: fine, parallel vertical spicules perpendicular to the cortex
- Mechanism: The periosteum is elevated and disrupted by the pathologic process; osteogenesis occurs in the subperiosteal space perpendicular to the cortex, creating radial spicules
- Indicates: Most aggressive, rapidly evolving process
- Classic causes: High-grade osteosarcoma (sunburst), Ewing sarcoma, occasionally sickle cell disease / thalassemia (hair-on-end in diploe of skull)
Summary Table
| Pattern | Aggression | Key Diseases |
|---|---|---|
| Solid | Non-aggressive | Stress fracture, osteoid osteoma, shin splints |
| Lamellated / Onion-skin | Intermediate | Ewing sarcoma, osteomyelitis, ABC |
| Codman triangle | Aggressive | Osteosarcoma, Ewing sarcoma |
| Sunburst | Most aggressive | High-grade osteosarcoma |
| Hair-on-end | Aggressive | Sarcoma; also marrow hyperplasia (thalassemia, sickle cell - skull) |
Other Contexts
- Osteomyelitis: periosteal reaction (often lamellated) accompanies osteolysis; MRI is optimal for demonstrating both periosteal reaction and bone marrow changes, and helps differentiate from infarction
- Sickle cell disease: osteolysis + periosteal reaction are early findings of bone infection
- Thyroid acropachy: solid periosteal reaction of the hands/feet in autoimmune thyroid disease (clubbing + digital swelling)
- Fracture healing: exuberant periosteal callus can mimic periosteal reaction
- Aseptic loosening (orthopaedic implants): outer cortical periosteal reaction along a stem tilted in the medullary canal suggests aseptic loosening
Key principle: No periosteal reaction pattern is pathognomonic, but the pattern is a major indicator of lesion aggressiveness when evaluating bone tumours on plain radiography.
Sources: Grainger & Allison's Diagnostic Radiology, Ch. 40 (Periosteal Reaction, pp. 1004-1008); Imaging Anatomy Vol. 3 - Bones, Joints, Vessels & Nerves, Ch. 1 (Periosteum, pp. 30-31)
This is a shared conversation. Sign in to Orris to start your own chat.