Notochord spinal malformation
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
notochord spinal malformation congenital
Finding Sources
Searching the Web
notochord spinal malformations split cord diastematomyelia neurenteric cyst clinical overview
Reading File
Searching Images
notochord spinal cord malformation embryology diagram
Loading Image
Loading Image
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile it.
Notochord & Spinal Malformations
1. Normal Notochord Development
The notochord arises around day 16–18 of embryogenesis from the primitive node. Mesenchymal cells migrate cranially, forming the notochordal process — a cellular tube extending from the primitive node to the prechordal plate. It undergoes a sequence of transformations (notochordal plate → definitive notochord) and serves two critical functions:
- Primary inductor of the neural plate: the notochord induces overlying embryonic ectoderm to thicken into the neural plate, the primordium of the entire CNS
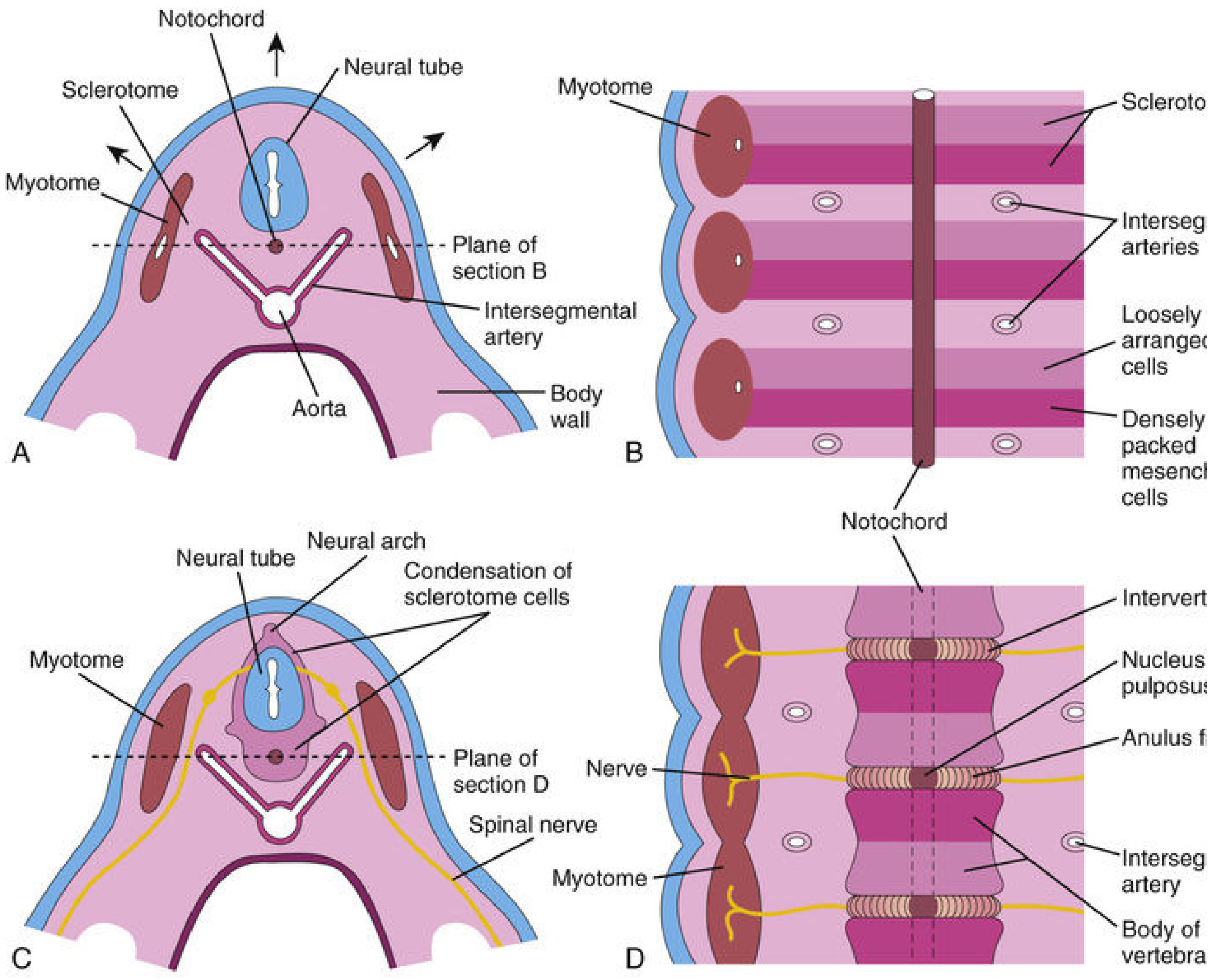
- Axial skeleton patterning: it signals sclerotomal cells (from somites) to condense around it and form the vertebral bodies
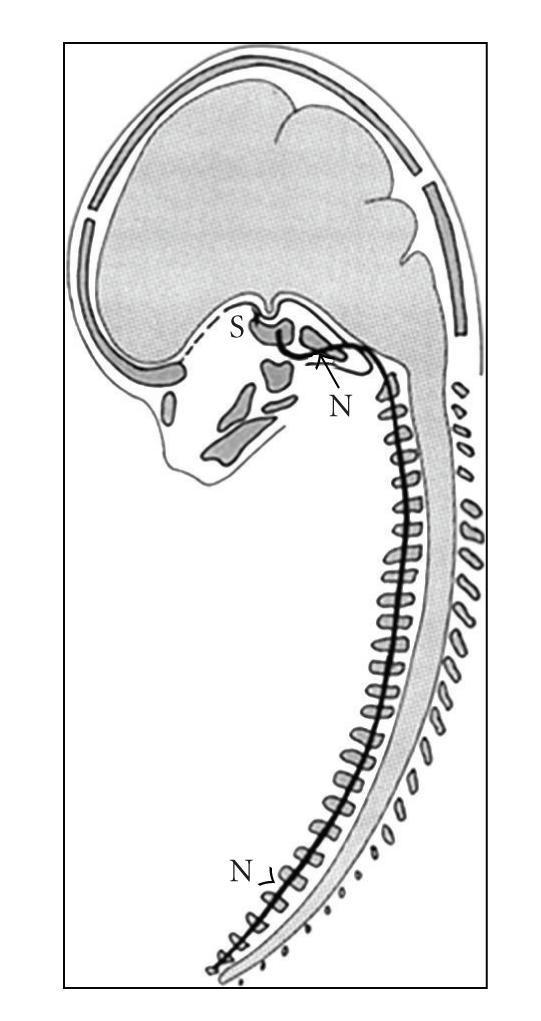
As vertebral bodies form, the notochord degenerates within each body but persists between vertebrae, expanding into the gelatinous nucleus pulposus of each intervertebral disc. — The Developing Human: Clinically Oriented Embryology
2. The Neurenteric Canal — The Key to Notochord-Related Malformations
During development, the proximal notochordal canal transiently communicates with the umbilical vesicle as the neurenteric canal. Under normal conditions, this canal is obliterated once the notochord is complete.
Failure of obliteration or aberrant reformation of this canal is the root cause of the major notochord-related spinal malformations.
3. Classification of Notochord-Related Spinal Malformations
A. Split Cord Malformation (SCM) — Diastematomyelia & Diplomyelia
The most clinically significant group. Pang's unified theory (1992) explains both types via a single embryological error during gastrulation (days 18–21): an accessory neurenteric canal forms due to abnormal adhesion between ectoderm and endoderm, creating an endomesenchymal tract that bisects both the notochord and the overlying neural plate.
| Feature | SCM Type I (Diastematomyelia) | SCM Type II (Diplomyelia) |
|---|---|---|
| Cord split | Two hemicords, separate dural sacs | Two hemicords, single dural tube |
| Septum | Rigid bony or cartilaginous spur | Non-rigid fibrous or fibrovascular septum |
| Tethering | More severe, spur tethers cord | Less mechanical tethering |
| Symptoms | Low back pain, leg weakness, scoliosis, bladder/bowel dysfunction | Similar but often milder |
Demographics: Predominantly female; lower thoracic/lumbar most common; up to 20% present in adulthood.
B. Neurenteric Cyst (Enterogenous Cyst)
Failure of normal separation between endoderm and ectoderm with persistence of notochord–endoderm adhesions leaves an epithelium-lined cyst, usually ventral to the spinal cord. These cysts are lined by endoderm-derived (gut-type) epithelium.
- Locations: Spinal (most common), mediastinal, intracranial, abdominal, pelvic, subcutaneous
- Most symptomatic presentations: pain, progressive neurological deficit, rarely infection
- Often co-exist with SCM — when found together, it supports the unified embryological mechanism (bisected notochord + persistent endodermal tract)
C. Split Notochord Syndrome
A spectrum of conditions where the notochord is physically split, leaving a communication between the gut and dorsal skin. The spectrum includes:
- Dorsal enteric fistula / sinus
- Anterior spina bifida
- Combined anterior + posterior vertebral defects with gut herniation
D. Chordoma
The malignant end of notochordal remnant pathology.
"Remnants of notochordal tissue may persist and form a chordoma, a rare neoplasm. Approximately one third of these slow-growing malignant tumors occurs at the base of the cranium and extends to the nasopharynx. Chordomas infiltrate bone and are difficult to remove. Chordomas also develop in the lumbosacral region." — The Developing Human: Clinically Oriented Embryology
Key features:
- Slow-growing but locally invasive
- Two predominant sites: cranial base/clivus (~35%) and sacrococcygeal (~50%)
- Cervical and thoracic vertebrae account for the remainder
- Surgical resection (when achievable with wide margins) provides long-term disease-free survival; proton beam radiotherapy used for residual/unresectable disease
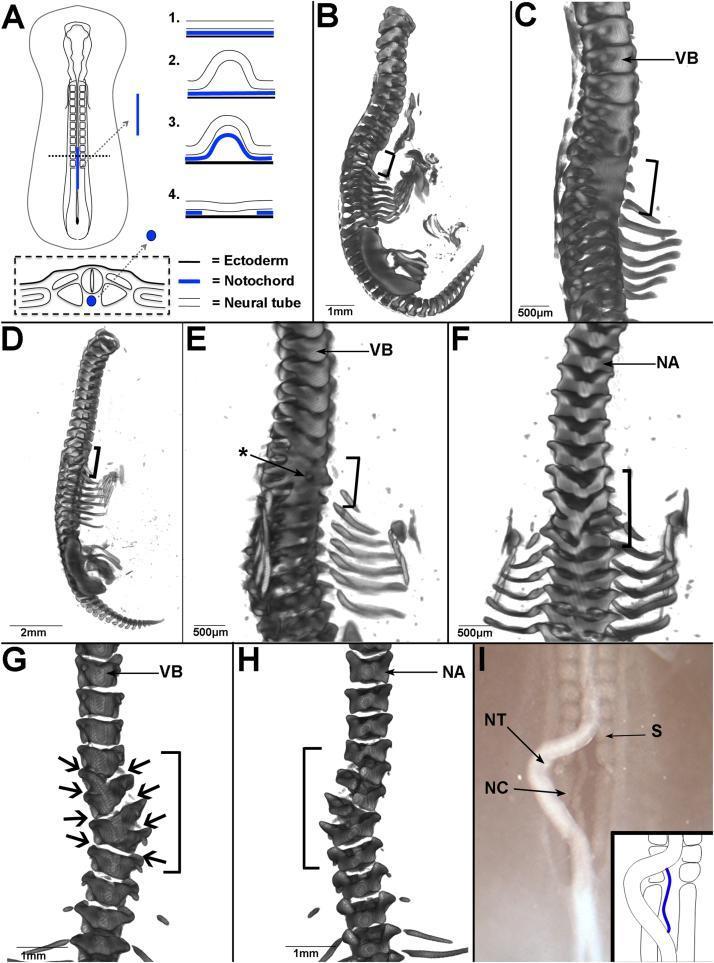
E. Vertebral Segmentation Defects (Notochord Signaling Failure)
When notochord ablation experiments are performed in animal models, the characteristic result is loss of vertebral body segmentation — adjacent bodies fuse into a continuous cartilaginous strip, with disrupted neural arch patterning. This mirrors human congenital segmentation defects:
- Hemivertebrae — partial failure of one sclerotome half
- Block vertebrae (Klippel-Feil syndrome at C-spine) — failure of segmentation
- Butterfly vertebrae — sagittal cleft from persistent notochordal tissue within the vertebral body
- Congenital scoliosis — asymmetric vertebral formation secondary to notochord-sclerotome signaling errors
4. Summary Table
| Malformation | Embryological Event | Key Feature | Clinical Presentation |
|---|---|---|---|
| SCM Type I (Diastematomyelia) | Accessory neurenteric canal → bony spur bisects cord | Bony/cartilaginous septum, two dural sacs | Scoliosis, leg weakness, tethered cord |
| SCM Type II (Diplomyelia) | Same, fibrous septum only | Fibrous septum, single dural sac | Milder, often incidental |
| Neurenteric cyst | Persistent notochord–endoderm adhesion | Ventral intradural cyst, gut-type epithelium | Pain, cord compression |
| Split notochord syndrome | Complete notochord splitting with gut communication | Dorsal enteric fistula ± anterior spina bifida | Midline back mass, meningitis risk |
| Chordoma | Residual notochordal tissue → neoplasm | Locally destructive tumor, clivus/sacrum | Chronic pain, CN palsies (cranial), sacral neurological deficit |
| Vertebral segmentation defects | Abnormal notochord–sclerotome signaling | Hemivertebrae, block vertebrae, butterfly vertebrae | Congenital scoliosis/kyphosis |
Sources:
- The Developing Human: Clinically Oriented Embryology — Notochordal Process & Notochord; Development of Vertebral Column; Chordoma
- Langman's Medical Embryology — Formation of the Notochord
- Pang D, Dias MS, Ahab-Barmada M. Split cord malformation: unified theory of embryogenesis. Neurosurgery 1992;31:451–480
- MedLink Neurology — Split Cord Malformation (unified theory and classification)
This is a shared conversation. Sign in to Orris to start your own chat.