1. Desferrioxamine - mechanism of action, therapeutic uses 2. Dimercaprol 3. Chelating Agents in clinical practice - list, elaborate briefly 1. Antioxidant Vitamins and Uses 2. Vitamin A - daily requirement, therapeutic uses 1. Explain why Folic Acid is started from First Trimester but Iron is started from Second Trimester of Pregnancy, even if Hb Level is normal 2. Catecholamines and Non-Catecholamines - compare and contrast 3. Drug Use in Children - general principles if diagrams moa adv effect uses precautions needed add it to answer , all detail answer for 2 mbbs pharmacology kdt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Searching the Web
catecholamines vs non-catecholamines sympathomimetics pharmacology differences 2nd MBBS
Here is the full, detailed 2nd MBBS Pharmacology answer covering all your topics:
SECTION A: CHELATING AGENTS & RELATED DRUGS
1. Desferrioxamine (Deferoxamine) - Mechanism of Action & Therapeutic Uses
Chemistry
Desferrioxamine (DFO) is a naturally occurring siderophore derived from Streptomyces pilosus. It is a hexadentate chelator - meaning one molecule has 6 oxygen donor atoms that wrap around one atom of trivalent iron (Fe³+) in an octahedral configuration.
Mechanism of Action
Fe³⁺ (Free iron) + Desferrioxamine
↓
Ferrioxamine complex
(stable, water-soluble, non-toxic)
↓
Excreted via urine (red-brown colored)
and bile/feces
- DFO binds free iron (both Fe³+ from plasma and iron from inside cells and mitochondria)
- It does NOT bind iron already incorporated into hemoglobin, transferrin, ferritin, or cytochromes - this selectivity is pharmacologically important
- The ferrioxamine complex is water-soluble, non-toxic, and renally excreted
- 100 mg DFO binds approximately 8.5 mg of elemental iron
Routes of Administration
- IV infusion (preferred in acute toxicity) - 15 mg/kg/hr; max 6 g/day
- SC infusion (preferred in chronic iron overload) - using infusion pump over 8-12 hours, 5-7 nights/week
- Oral (for gastric binding in acute poisoning) - 8-12 g orally to absorb unabsorbed iron in the gut
Therapeutic Uses
| Indication | Details |
|---|---|
| Acute iron poisoning | IV deferoxamine; urine turns vin-rosé/red-brown (positive vin-rosé test = confirms free iron present) |
| Chronic iron overload (hemosiderosis) | Thalassemia major, sickle cell disease requiring repeated transfusions; SC infusion |
| Hereditary hemochromatosis | When phlebotomy is contraindicated |
| Aluminum toxicity | Dialysis encephalopathy (dialysis dementia) - DFO chelates aluminum; caution: may mobilize Al into brain |
| Radioactive heavy metal poisoning | Promotes removal of radioactive iron and heavy metals |
Adverse Effects
- Ocular: Retinal toxicity, visual field defects, night blindness, cataracts (especially with high doses/young patients)
- Auditory: Sensorineural hearing loss (SNHL) - reversible in early stages
- Systemic: Hypotension with rapid IV infusion, allergic reactions, febrile reactions
- Infections: DFO acts as a siderophore for Rhizopus spp., increasing risk of mucormycosis (especially in dialysis patients)
- Long-term SC use: Local injection site reactions, skeletal dysplasia in children
- Monitoring: Regular ophthalmologic and audiometric testing required during chronic therapy
Newer Oral Iron Chelators
- Deferasirox (tridentate) - oral, once daily; hepatotoxic
- Deferiprone - oral; causes agranulocytosis (requires WBC monitoring)
2. Dimercaprol (BAL - British Anti-Lewisite)
History
Developed during World War II as an antidote to Lewisite (an arsenical war gas). Chemical name: 2,3-dimercaptopropanol.
Chemistry & Mechanism of Action
Heavy metal (As, Hg, Pb) + SH groups of tissue enzymes
↓
Enzyme inhibition → cell death
Dimercaprol (two free -SH groups)
↓
Competes with enzyme -SH groups
↓
Metal-BAL complex (water-soluble ring chelate)
↓
Excreted in urine
Key principle: Heavy metals have high affinity for sulfhydryl (-SH) groups of enzymes (particularly those involved in cellular respiration, e.g., pyruvate dehydrogenase). Dimercaprol contains two adjacent -SH groups which form a stable 5-membered ring chelate with the metal, effectively "rescuing" the enzyme.
The metal-dimercaprol complex is more stable than the metal-enzyme complex - this is the basis of its antidotal action.
Pharmacokinetics
- Given as 10% solution in arachis oil (peanut oil) with benzyl benzoate via deep IM injection (never IV - too toxic)
- Oily preparation because BAL is water-insoluble
- Peak blood levels: 30-60 minutes
- Metabolized in liver; excreted in bile and urine
- Short half-life (~4 hours) necessitates frequent dosing
Therapeutic Uses
| Metal Poisoning | Notes |
|---|---|
| Arsenic | Drug of choice for acute arsenic poisoning |
| Mercury | Inorganic mercury poisoning (NOT for organic methylmercury - may worsen CNS distribution) |
| Lead | Used in combination with CaNa₂-EDTA, especially in encephalopathy |
| Gold | Gold-induced nephropathy or dermatitis |
| Antimony, Bismuth, Copper | Less commonly used |
| Lewisite poisoning | Original indication |
Dosing Schedule (Standard)
- Severe poisoning: 3-4 mg/kg IM every 4 hours for 2 days, then twice daily for 10 days (or until recovery)
- Mild poisoning: 2.5 mg/kg IM every 6 hours for 2 days, then every 12 hours for 7 days
Adverse Effects
- Pain at injection site (IM)
- Hypertension and tachycardia (dose-dependent)
- Nausea, vomiting, salivation, headache, lacrimation, rhinorrhea (within 15-20 min)
- Fever in children (common)
- Nephrotoxic at high doses - alkalinize urine to protect kidneys
- Hemolysis in G6PD-deficient patients (CONTRAINDICATED)
- Hepatotoxic - contraindicated in hepatic failure
Contraindications
- G6PD deficiency (hemolysis risk)
- Hepatic damage (liver metabolizes complex)
- Iron, cadmium, or selenium poisoning (BAL-metal complex is MORE toxic than metal alone)
- Renal impairment (reduces excretion of toxic complex)
3. Chelating Agents in Clinical Practice - Complete List & Brief Elaboration
Chelating agents (from Greek chele = claw) are molecules that bind metal ions to form stable, water-soluble ring complexes, which are then excreted renally or via bile.
Complete List
| Chelating Agent | Metal(s) Targeted | Route | Key Feature |
|---|---|---|---|
| Dimercaprol (BAL) | As, Hg, Pb, Au, Sb | IM | Two -SH groups; original heavy metal antidote |
| CaNa₂-EDTA | Pb (primary), also Cu, Hg, Co, Ni | IV/IM | Only for lead currently; can redistribute lead to brain |
| Penicillamine | Cu (Wilson's), Pb, Hg, Au | Oral | D-form used; also used in rheumatoid arthritis |
| Desferrioxamine (DFO) | Fe³⁺, Al³⁺ | IV/SC/IM | Selective for trivalent metals |
| Deferasirox | Fe³⁺ | Oral | Once daily; renal and hepatic toxicity |
| Deferiprone | Fe³⁺ | Oral | Agranulocytosis risk |
| Succimer (DMSA) | Pb (preferred), Hg, As | Oral | Superior to EDTA - does NOT redistribute lead to brain; safe in G6PD deficiency |
| DMPS (Unithiol) | Hg, Pb, As | Oral/IV | Same dithiol mechanism as BAL; more hydrophilic |
| Trientine | Cu (Wilson's disease) | Oral | Alternative to penicillamine when intolerant |
| Prussian blue | Cs-137, Tl | Oral | Binds radioactive cesium/thallium in gut |
Clinical Application Guidelines
Lead poisoning:
- Asymptomatic, blood lead 25-45 μg/dL: succimer (oral DMSA)
- Symptomatic or blood lead >45 μg/dL: CaNa₂-EDTA + dimercaprol (BAL) together
- Lead encephalopathy: BAL first (4 mg/kg), then 4 hrs later add CaNa₂-EDTA
Mercury poisoning:
- Inorganic: BAL or DMSA
- Organic (methylmercury): DMSA (BAL may worsen brain distribution)
Arsenic poisoning:
- BAL (IM) or DMSA (oral)
Wilson's disease (copper):
- Penicillamine (first line) or trientine
Iron toxicity:
- Desferrioxamine (IV)
Aluminum (dialysis):
- Desferrioxamine (IV/IM)
SECTION B: VITAMINS
1. Antioxidant Vitamins and Their Uses
What Are Antioxidants?
Free radicals (reactive oxygen species - ROS) are molecules with unpaired electrons that damage cell membranes, proteins, and DNA. Antioxidant vitamins neutralize these by donating electrons without themselves becoming damaging radicals.
The Three Major Antioxidant Vitamins
A. Vitamin C (Ascorbic Acid)
Mechanism of Antioxidant Action:
- Water-soluble antioxidant, works in aqueous compartments
- Donates electrons to neutralize superoxide (O₂•⁻), hydroxyl radical (•OH), and peroxyl radicals
- Regenerates oxidized Vitamin E back to its active form (ascorbate-vitamin E cycle)
- Inhibits LDL oxidation (prevents foam cell formation in atherosclerosis)
Other Functions:
- Cofactor for prolyl and lysyl hydroxylase (collagen synthesis)
- Enhances iron absorption from gut (reduces Fe³⁺ to Fe²⁺)
- Immune function: supports neutrophil and NK cell activity
Therapeutic Uses:
- Scurvy treatment and prevention (100-200 mg/day)
- Wound healing promotion (post-surgery, burns)
- Common cold - reduces duration, not incidence
- Iron deficiency anemia - given with iron to enhance absorption
- Methemoglobinemia (along with methylene blue)
Daily Requirement: 60-90 mg/day (adult); 500-2000 mg/day in therapeutic doses
Deficiency: Scurvy - perifollicular hemorrhages, bleeding gums, corkscrew hairs, poor wound healing
B. Vitamin E (Tocopherol)
Mechanism of Antioxidant Action:
- Fat-soluble antioxidant - resides in cell membranes and lipid bilayers
- Donates a hydrogen atom to lipid peroxyl radicals (LOO•), breaking the chain reaction of lipid peroxidation
- The tocopheroxyl radical formed is less reactive; regenerated by Vitamin C
LOO• (lipid peroxyl radical) + Vitamin E-OH
↓
LOOH + Vitamin E-O• (tocopheroxyl radical - stable)
↓
Regenerated by Vitamin C → Vitamin E-OH again
Therapeutic Uses:
- Premature infant - prevents hemolytic anemia in neonates
- Antioxidant in atherosclerosis prevention (controversial in trials - WACS, WAVE)
- Abetalipoproteinemia (fat malabsorption - requires high dose supplementation)
- Ataxia with vitamin E deficiency (AVED) - genetic disorder
- Skin photoaging (topical)
- Intermittent claudication (marginal benefit)
Daily Requirement: 15 mg/day (adults); 1000 mg/day is the UL (least toxic fat-soluble vitamin)
Deficiency: Hemolytic anemia in premature infants; spinocerebellar ataxia, peripheral neuropathy in adults
C. Beta-Carotene (Provitamin A)
Mechanism: Quenches singlet oxygen (¹O₂), a highly reactive form of oxygen not neutralized well by other antioxidants
Note: In smokers, high-dose beta-carotene supplementation increased lung cancer incidence (CARET trial) - an important clinical caveat
Summary Table: Antioxidant Vitamins
| Feature | Vitamin C | Vitamin E | Beta-Carotene |
|---|---|---|---|
| Solubility | Water-soluble | Fat-soluble | Fat-soluble |
| Location | Cytoplasm, plasma | Cell membranes | Fat droplets |
| ROS targeted | O₂•⁻, •OH, H₂O₂ | Lipid peroxyl radicals | Singlet oxygen |
| Key clinical use | Scurvy, wound healing | Neonatal hemolysis, AVED | Photosensitivity disorders |
| Toxicity | Renal stones at >2g/day | Low toxicity | Safe; high dose in smokers - cancer risk |
2. Vitamin A - Daily Requirement and Therapeutic Uses
Chemistry
Vitamin A is a group of fat-soluble retinoids:
- Retinol (preformed vitamin A - from animal sources)
- Retinal (retinaldehyde - visual cycle)
- Retinoic acid (gene regulation, differentiation)
- Beta-carotene (provitamin A from plant sources; 12 μg β-carotene = 1 μg retinol = 1 RAE)
Daily Requirement
| Group | Requirement |
|---|---|
| Adult males | 900 RAE/day (900 μg retinol/day = ~3000 IU) |
| Adult females | 700 RAE/day (700 μg retinol/day = ~2333 IU) |
| Pregnant women | 770 RAE/day |
| Lactating women | 1300 RAE/day |
| Infants (0-6 months) | 400 RAE/day |
| Upper tolerable limit (UL) | 3000 μg/day (10,000 IU) |
Conversion: 1 RAE = 1 μg retinol = 12 μg β-carotene = 24 μg other carotenoids = 3.33 IU
Functions (Quick Recap)
Retinol → Retinal → Rhodopsin (rod pigment) → VISION
Retinal ← → Retinoic acid → Nuclear RAR/RXR receptors → GENE EXPRESSION
→ Cell differentiation, growth
→ Immune function (T-cell, NK cell maturation)
→ Glycoprotein synthesis (mucus production)
Deficiency - Clinical Features
| Stage | Feature |
|---|---|
| Early | Night blindness (nyctalopia) - earliest & reversible sign |
| Progressive | Xerophthalmia - conjunctival xerosis, Bitot's spots (white keratinized patches on sclera) |
| Late | Corneal ulceration, keratomalacia (corneal softening) |
| Severe | Corneal scarring → permanent blindness (blinded ~250,000 children/year worldwide) |
| Systemic | Growth retardation, follicular hyperkeratosis ("toad skin"), increased infection susceptibility |
Therapeutic Uses
| Use | Drug/Form | Details |
|---|---|---|
| Vitamin A deficiency | Retinol / retinyl esters | Night blindness, xerophthalmia treatment |
| Measles | High-dose Vitamin A | WHO recommends two doses (100,000 IU < 1 yr; 200,000 IU > 1 yr) - reduces mortality |
| Acne vulgaris (mild) | Tretinoin (all-trans retinoic acid) | Topical; reduces keratin plugging |
| Severe cystic acne | Isotretinoin (13-cis retinoic acid) | Oral; teratogenic - iPLEDGE program required |
| Acute Promyelocytic Leukemia (APL) | ATRA (all-trans retinoic acid, oral) | Induces differentiation of leukemic promyelocytes; combined with arsenic trioxide |
| Psoriasis | Acitretin (synthetic retinoid) | Oral; teratogenic |
| Prevention of NTDs | Indirectly (through folic acid programs) |
Toxicity (Hypervitaminosis A)
Acute: Headache, vomiting, papilledema, increased intracranial pressure (single large dose >200,000 IU)
Chronic: Alopecia, dry skin, hepatotoxicity, hypercalcemia, premature epiphyseal closure in children, teratogenicity (most dangerous) - contraindicated in pregnancy (causes CNS malformations, craniofacial defects, cardiac defects)
SECTION C: SPECIAL PHARMACOLOGY TOPICS
1. Why Folic Acid is Started from 1st Trimester but Iron from 2nd Trimester
This is a high-yield exam question with a clear physiological rationale:
Folic Acid - Must Start from 1st Trimester (Ideally Periconceptional)
Reason: Neural Tube Formation occurs in the 1st Trimester (Days 18-28 of gestation)
Fertilization → Implantation → Neural plate forms (Day 18)
→ Neural groove
→ Neural tube closure (Days 22-28)
→ This is in the FIRST TRIMESTER (often before woman knows she is pregnant!)
- Folic acid is required for DNA synthesis (purine and thymidylate synthesis)
- Rapidly dividing neural tube cells require folate for normal cell division
- Deficiency leads to: Spina bifida, anencephaly, encephalocele (neural tube defects)
- Neural tube CLOSES by Day 28 - before most women realize they are pregnant
- Therefore, folate supplementation must begin at least 1 month before conception and through the first trimester (ideally taken by all women of childbearing age)
- Dose: 400 μg (0.4 mg)/day (normal risk); 5 mg/day (high risk - previous NTD child, epilepsy patients on AEDs, etc.)
Additional benefits of folic acid in pregnancy:
- Prevents megaloblastic anemia of pregnancy
- Reduces risk of congenital heart defects, orofacial clefts, limb defects
- Lowers homocysteine (reduces thrombotic risk)
Why it is started even when Hb is normal: Because the purpose is NOT anemia prevention at this stage but fetal neural tube protection - a structural development process.
Iron - Started from 2nd Trimester (Even if Hb is Normal)
Reason: Maternal and fetal iron demand rises sharply in the 2nd trimester
1st Trimester: Iron demand LOW (no menstruation, fetal growth minimal, iron stores are used up slowly)
2nd Trimester: ↑↑ Fetal growth ↑↑ Plasma volume expansion ↑↑ Red cell mass increases
→ Total iron need = 1000 mg extra over pregnancy
→ 300 mg to fetus/placenta
→ 500 mg for maternal RBC mass expansion
→ 200 mg basal loss
3rd Trimester: Maximum iron demand (fetal liver stores iron for post-natal period)
Why NOT in 1st trimester (even if Hb is normal):
- Morning sickness - iron worsens nausea and vomiting (common in 1st trimester)
- Iron demand is low in 1st trimester - maternal stores are sufficient
- Risk of excess iron - free iron is pro-oxidant and potentially teratogenic in early organogenesis
- Compliance - adverse GI effects deter compliance; delaying start improves adherence
Why started in 2nd trimester even with normal Hb:
- Prophylactic iron prevents iron deficiency anemia that develops in 2nd/3rd trimester
- Fetal iron requirement peaks in 2nd-3rd trimester; maternal stores may be insufficient
- Dose: 100-200 mg elemental iron/day (prophylactic; IFA tablets in government programs = 100 mg elemental iron + 0.5 mg folic acid)
Summary Table
| Feature | Folic Acid | Iron |
|---|---|---|
| Start time | Periconceptional → 1st trimester | 2nd trimester |
| Why early | Neural tube closure Day 22-28 | Low demand in 1st trimester; GI tolerance |
| Purpose when Hb normal | Prevent NTDs (structural) | Prevent future anemia (prophylaxis) |
| Dose in pregnancy | 400 μg/day (0.4 mg normal; 5 mg high risk) | 100-200 mg elemental iron/day |
| Danger if omitted | Spina bifida, anencephaly | Iron deficiency anemia, LBW, preterm |
2. Catecholamines vs Non-Catecholamines - Compare and Contrast
Definition
Catecholamines: Sympathomimetic amines with a catechol nucleus (benzene ring with two adjacent hydroxyl groups at positions 3 and 4) and an ethylamine side chain.
Non-catecholamines: Sympathomimetic amines that lack the catechol nucleus (absent or modified ring hydroxyl groups).
Structure Comparison
Catechol nucleus:
OH
|
3-C
| \
| benzene ring
| /
4-C
|
OH
+ ethylamine side chain (-CH₂-CH₂-NH₂)
Catecholamines = catechol nucleus + ethylamine
Non-catecholamines = Modified ring (absent/different OH groups) + ethylamine
Examples
| Catecholamines | Non-Catecholamines |
|---|---|
| Adrenaline (Epinephrine) | Amphetamine |
| Noradrenaline (Norepinephrine) | Ephedrine |
| Dopamine | Phenylephrine |
| Dobutamine | Salbutamol (Albuterol) |
| Isoprenaline (Isoproterenol) | Terbutaline |
| Methoxamine | |
| Phenylpropanolamine |
Detailed Comparison Table
| Property | Catecholamines | Non-Catecholamines |
|---|---|---|
| Structure | Catechol nucleus (3,4-diOH benzene) + ethylamine | Modified benzene (no/different OH) + ethylamine |
| Oral bioavailability | POOR (destroyed by intestinal MAO and COMT, and liver first-pass) | GOOD (resistant to gut/liver MAO and COMT) |
| Route of administration | IV, SC, inhalation | IV, oral, SC, inhalation |
| Mechanism of action | Primarily DIRECT (act directly on adrenergic receptors) | Direct, Indirect, or Mixed depending on drug |
| CNS penetration | POOR (polar due to two -OH groups; does not cross BBB) | GOOD (less polar; crosses BBB easily - basis for CNS stimulant effects) |
| Metabolism | Rapidly metabolized by MAO and COMT | Resistant to MAO and COMT; longer duration |
| Duration of action | SHORT (minutes) | LONGER (hours) |
| Tachyphylaxis | Less common | More common (indirect-acting agents deplete NE stores) |
| Potency | High | Moderate-high (varies) |
| Receptor selectivity | Varies (Epi: α+β; Nor: mainly α; Iso: mainly β) | Varies widely (phenylephrine: α₁; salbutamol: β₂) |
Mechanism of Action - Key Differences
Catecholamines: Act directly on α and β adrenergic receptors
Non-catecholamines:
- Direct-acting: Phenylephrine (α₁), salbutamol (β₂) - act directly on receptors
- Indirect-acting: Amphetamine, tyramine - enter nerve terminal → displace NE from storage vesicles → NE released → acts on receptors
- Mixed-acting: Ephedrine - both direct receptor agonism AND NE release
Indirect mechanism (Amphetamine/Ephedrine):
Drug → enters adrenergic nerve terminal
→ displaces NE from vesicles
→ NE floods synapse
→ NE acts on post-synaptic receptors
→ Adrenergic effect
Pharmacological Effects Comparison
| Effect | Catecholamines (e.g., Adrenaline) | Non-Catecholamines (e.g., Ephedrine) |
|---|---|---|
| Heart rate | ↑↑ (β₁) | ↑ (less intense) |
| Blood pressure | Biphasic (Epi) / ↑ (Nor) | ↑ (prolonged) |
| Bronchodilation | ↑↑ (β₂, adrenaline) | ↑ (ephedrine oral) |
| CNS effects | Minimal (poor BBB penetration) | Prominent (anxiety, insomnia, alertness) |
| Duration | Short (minutes) | Long (hours) |
| Oral use | Not effective | Effective |
| Tachyphylaxis | Not typical | Yes (indirect-acting: NE depletion) |
Clinical Uses
Catecholamines:
- Adrenaline (Epinephrine): Anaphylaxis, cardiac arrest, local anesthetic adjuvant
- Noradrenaline: Septic shock (vasopressor)
- Dopamine: Cardiogenic shock (inotrope + renal dose vasodilation)
- Dobutamine: Acute decompensated heart failure (β₁ inotrope)
- Isoprenaline: Complete heart block (temporary), severe bradycardia
Non-Catecholamines:
- Salbutamol/Terbutaline: Bronchial asthma (β₂ agonist)
- Phenylephrine: Nasal decongestant, hypotension during spinal anesthesia
- Ephedrine: Hypotension during spinal anesthesia, nasal congestion
- Amphetamine: ADHD, narcolepsy
- Pseudoephedrine: Nasal decongestant (oral)
3. Drug Use in Children - General Principles
Why Children are NOT "Small Adults"
Children have distinct pharmacokinetic and pharmacodynamic differences from adults that make their response to drugs fundamentally different. The maxim from pediatric pharmacology: "Children are not just small adults."
Age-Based Classification
| Group | Age |
|---|---|
| Premature neonate | <37 weeks gestation |
| Neonate | 0-28 days |
| Infant | 1 month - 1 year |
| Child | 1-12 years |
| Adolescent | 12-18 years |
A. Pharmacokinetic Differences in Children
1. ABSORPTION
| Factor | Child | Clinical Significance |
|---|---|---|
| Gastric acid | Reduced in neonates (achlorhydria) → pH 6-8 | Acid-labile drugs (penicillin G) better absorbed; acid-dependent drugs (itraconazole) poorly absorbed |
| Gastric emptying | Slow in neonates | Delayed oral drug absorption |
| GI motility | Reduced in neonates | Erratic absorption of oral drugs |
| IM absorption | Reduced (less muscle mass, poor perfusion) | Unreliable IM route in neonates |
| Skin (transdermal) | Increased in neonates (thin, high surface area:body weight) | Toxic absorption - hexachlorophene, topical steroids, EMLA cream caution |
2. DISTRIBUTION
| Factor | Neonate/Infant | Adult | Clinical Effect |
|---|---|---|---|
| Total body water | 75-80% of body weight | 60% | Higher Vd for water-soluble drugs (e.g., aminoglycosides) → higher mg/kg dose needed |
| Body fat | Less (especially preterm) | More | Lower Vd for fat-soluble drugs |
| Plasma protein binding | Reduced (less albumin, different albumin structure, competitive displacement by bilirubin) | Normal | More free (active) drug → higher effect/toxicity; e.g., sulfonamides displace bilirubin → kernicterus risk |
| Blood-brain barrier | Immature in neonates | Intact | Greater CNS drug penetration → morphine, phenobarbitone more CNS active |
| Body compartments | Different proportions | Standard | Dose calculations based on mg/kg (weight) or mg/m² (body surface area) |
3. METABOLISM
| Factor | Neonate/Child | Clinical Significance |
|---|---|---|
| CYP450 enzymes | Reduced in neonates; mature by 3-6 months; HIGHER than adults at 1-10 years | Chloramphenicol: reduced metabolism → Gray baby syndrome in neonates |
| Phase II glucuronidation | Very low at birth | Chloramphenicol accumulates (glucuronidation is primary pathway) |
| Phase II sulfation | Relatively intact | Compensates for glucuronidation deficiency in neonates (e.g., acetaminophen) |
| MAO activity | Reduced in neonates | |
| Plasma esterases | Reduced in neonates | Succinylcholine, cocaine metabolism reduced |
| Older children (1-10 yrs) | Higher CYP activity per kg than adults | May require higher mg/kg doses |
Gray Baby Syndrome (Chloramphenicol):
- Neonates lack UGT (UDP-glucuronosyltransferase) → chloramphenicol accumulates
- Features: abdominal distension, vomiting, gray cyanosis, cardiovascular collapse, death
- Dose in neonates: 25 mg/kg/day (vs 50-100 mg/kg/day in adults)
4. EXCRETION (RENAL)
| Parameter | Neonates | Adult values achieved |
|---|---|---|
| GFR | 2-4 mL/min (very low) | By ~6-12 months |
| Tubular secretion | Very low | By ~7-12 months |
| Tubular reabsorption | Also low | Matures gradually |
Clinical consequence: Drugs eliminated by kidneys (digoxin, aminoglycosides, penicillins) have prolonged half-life in neonates → dose reduction and increased dosing intervals required
B. Pharmacodynamic Differences
| System | Child vs Adult |
|---|---|
| CNS | More sensitive to opioids, sedatives, anticonvulsants (immature BBB) |
| Respiratory | Neonates at risk of apnea with opioids, barbiturates |
| Cardiovascular | Neonatal heart is rate-dependent (less contractile reserve) |
| Bone/growth | Tetracyclines - bind calcium in growing bone/teeth → staining and growth inhibition (contraindicated <8 years) |
| Fluoroquinolones | Damage growing cartilage (avoid in children; limited exceptions) |
C. Dose Calculation Methods
Standard method: mg/kg body weight - most commonly used
Body Surface Area (BSA) method: More accurate for drugs with narrow therapeutic index
- BSA (m²) = √(Height(cm) × Weight(kg) / 3600)
- Child's dose = (Child's BSA / 1.73 m²) × Adult dose
Clark's Rule (historical): Child's dose = (Weight in lbs / 150) × Adult dose
Young's Rule (historical): Child's dose = (Age in years / Age + 12) × Adult dose
Note: Fried's rule for infants: Dose = (Age in months / 150) × Adult dose
D. Specific Drug Problems in Children (High-Yield)
| Drug | Problem | Mechanism |
|---|---|---|
| Chloramphenicol | Gray baby syndrome | Low UGT activity → drug accumulation |
| Tetracyclines | Teeth staining, bone growth inhibition | Calcium chelation in growing structures |
| Sulfonamides/aspirin | Kernicterus in neonates | Displace bilirubin from albumin → free bilirubin enters CNS |
| Fluoroquinolones | Arthropathy | Damage cartilage in growing joints |
| Vitamin K (synthetic) | Hemolysis in G6PD-deficient neonates | Oxidative stress |
| Hexachlorophene | Neurotoxicity | Excessive transdermal absorption |
| Opioids | Respiratory depression, apnea | Immature respiratory control, BBB |
| NSAIDs | Reye's syndrome (Aspirin + viral illness) | Mitochondrial dysfunction |
| Benzodiazepines | Prolonged sedation | Reduced CYP3A4 in neonates |
E. General Principles - Summary
- Use approved pediatric formulations when available; avoid adult tablet splitting
- Calculate dose per kg body weight for most drugs; use BSA for chemotherapy and some narrow-TI drugs
- Adjust for organ maturity - reduce doses for renally eliminated drugs in neonates; recognize reduced CYP activity in neonates but higher in toddlers
- Avoid certain drugs entirely: tetracyclines (<8 yr), fluoroquinolones (unless no alternative), aspirin (<12 yr viral illness), sulfonamides in neonates
- Monitor more frequently - children's physiology changes rapidly; dose adjustment needed with growth
- Flavoring and formulations - liquid formulations preferred; adherence may be poor with bitter drugs
- Transdermal exposure risk - all topical agents carry higher systemic absorption risk
- Informed consent - from parent/guardian with child's assent where age-appropriate
Bone Marrow Histology - Normal vs Folate Deficiency
The microscopic changes seen in folate-deficient megaloblastic anemia versus a normal marrow:
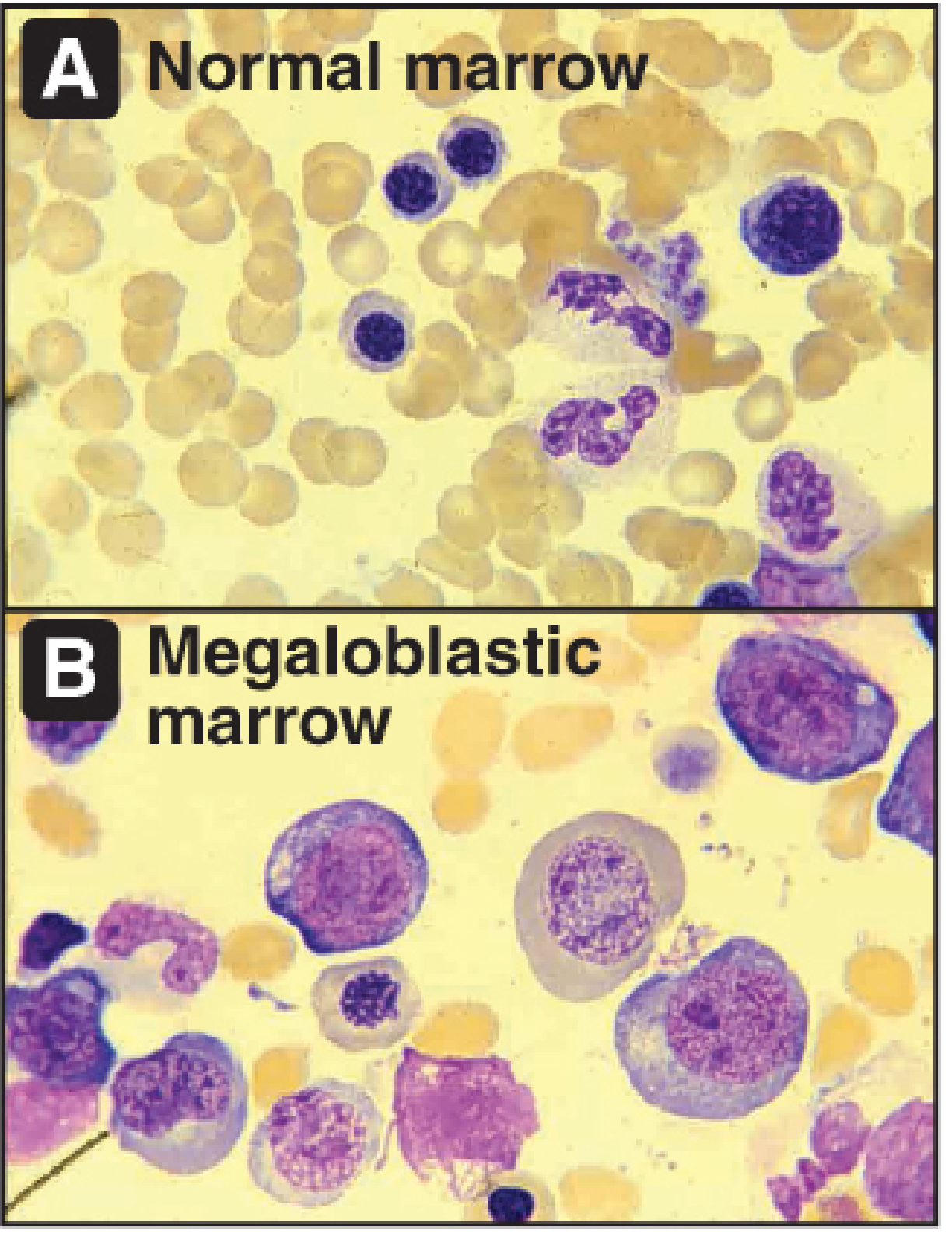
Normal marrow (A) vs Megaloblastic marrow (B): Note the giant erythroid precursors with fine, open chromatin (nuclear-cytoplasmic asynchrony) in the megaloblastic marrow - characteristic of folate or B12 deficiency.
Sources: The Essentials of Forensic Medicine & Toxicology 36e | Harrison's Principles of Internal Medicine 22e (2025) | Biochemistry 8e Lippincott Illustrated Reviews | Tintinalli's Emergency Medicine | Creasy & Resnik Maternal-Fetal Medicine | Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.