Pneumonia treatment
Reading File
Finding Sources
Searching PubMed
"pneumonia" AND "treatment" AND "antibiotics"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I have enough comprehensive content to write a thorough answer. Let me compile it now.
Pneumonia Treatment
Pneumonia is an infection of the lower respiratory tract causing consolidation of the alveoli. Treatment depends on the clinical setting (community vs. hospital-acquired), severity of illness, likely pathogens, and patient risk factors. Below is a structured overview.
1. Classification of Pneumonia
| Type | Definition |
|---|---|
| Community-Acquired Pneumonia (CAP) | Acquired outside the hospital or within 48 h of admission |
| Hospital-Acquired Pneumonia (HAP) | Occurs ≥48 h after hospital admission, not incubating at admission |
| Ventilator-Associated Pneumonia (VAP) | HAP occurring ≥48 h after endotracheal intubation |
| Aspiration Pneumonia | From macroaspiration of oropharyngeal/gastric contents |
2. Common Pathogens
Typical bacteria (15-30% of CAP): Streptococcus pneumoniae (5-16%), Staphylococcus aureus (3-5%), Haemophilus influenzae (up to 7%), Pseudomonas aeruginosa (<1-3%)
Atypical bacteria (~4%): Mycoplasma pneumoniae, Legionella spp., Chlamydia pneumoniae
Viruses (20-27%): Rhinoviruses, influenza A/B, human metapneumovirus, RSV, parainfluenza, and coronaviruses
No pathogen is identified in 55-66% of cases.
- Goldman-Cecil Medicine, International Edition
3. Severity Assessment
Pneumonia Severity Index (PSI)
- Classes I-III (score ≤90): Outpatient management is generally safe
- Higher scores warrant hospital admission, ICU for scores >130
CURB-65 Score (simpler alternative)
Each criterion = 1 point: Confusion, Urea >7 mmol/L, Respiratory rate ≥30/min, BP <90/60 mmHg, age ≥65
- Score 0-1: Outpatient
- Score 2: Short-stay admission
- Score ≥3: ICU consideration
4. Antibiotic Treatment by Setting
Outpatient CAP (Mild, No Comorbidities)
- Monotherapy for 5 days with:
- Amoxicillin (first-line beta-lactam)
- Doxycycline
- Azithromycin (where macrolide resistance rates are low)
Outpatient CAP (With Comorbidities / Risk for Drug-Resistant Organisms)
- Monotherapy with a respiratory fluoroquinolone (levofloxacin, moxifloxacin), OR
- Combination: one of amoxicillin/clavulanate, cefpodoxime, or cefuroxime PLUS azithromycin, clarithromycin, or doxycycline
Inpatient CAP (Non-Severe, No MRSA/Pseudomonas Risk)
- Monotherapy: respiratory fluoroquinolone, OR
- Combination: beta-lactam + macrolide
- 3 days of IV beta-lactam therapy may be adequate if clinically stable
Inpatient CAP (Severe)
- Dual therapy: beta-lactam + macrolide OR beta-lactam + respiratory fluoroquinolone
- Cover for MRSA if: prior parenteral antibiotics in last 90 days, prior MRSA infection; use vancomycin or linezolid
- Cover for Pseudomonas if similar risk factors - use antipseudomonal beta-lactam
- Anaerobic coverage (clindamycin) only if lung abscess or empyema suspected
Duration
-
Minimum 5 days for most patients
-
7 days for suspected MRSA or Pseudomonas
-
Extend until clinical stability (resolution of vital sign abnormalities, tolerating oral intake, normal mentation)
-
Goldman-Cecil Medicine, International Edition
5. Special Pathogens
| Pathogen | Preferred Treatment |
|---|---|
| Legionella pneumophila | Azithromycin 500 mg/day OR levofloxacin 750 mg/day |
| Mycoplasma pneumoniae | Macrolide (azithromycin); tetracycline if macrolide-resistant |
| MRSA | Vancomycin or linezolid |
| Pseudomonas aeruginosa | Antipseudomonal beta-lactam (piperacillin-tazobactam, cefepime, or meropenem) |
| Influenza with bacterial co-infection | Antiviral (oseltamivir) + empirical antibiotic for CAP |
- Fishman's Pulmonary Diseases and Disorders
6. Pediatric Pneumonia
-
Neonates: Target group B streptococci and gram-negative organisms (e.g., E. coli) - use ampicillin + gentamicin
-
Children <5 years: Cover H. influenzae and S. pneumoniae (amoxicillin)
-
Children >5 years: Add macrolide coverage for M. pneumoniae
-
Oral antibiotics are adequate for most mild-to-moderate cases; IV therapy for severe disease or inability to tolerate oral intake
-
Textbook of Family Medicine 9e
7. HAP / VAP Treatment
- Guided by local antibiograms and MDR risk factors
- MDR risk factors include: prior IV antibiotics, prior hospitalization >5 days, septic shock at time of VAP, ARDS, renal replacement therapy
- Empirical broad-spectrum coverage: antipseudomonal beta-lactam + antipseudomonal fluoroquinolone or aminoglycoside; add vancomycin/linezolid if MRSA risk
- Short-course antibiotic therapy (minimum effective duration) is recommended when clinically applicable
8. Adjunctive / Supportive Therapy
- Corticosteroids: Generally NOT recommended for routine CAP; may be used in refractory septic shock (e.g., hydrocortisone 200 mg for 4-8 days)
- Oxygen therapy: Target SpO2 ≥95%
- Fluids: Correct dehydration; aggressive IV fluids if septic
- Antiviral agents: Oseltamivir for influenza-positive patients, regardless of duration of illness before diagnosis
- Switch from IV to oral: Early de-escalation from IV to oral antibiotics (once stable) reduces hospital stay without compromising outcomes
9. Hospitalization Indications
- Failure to respond or tolerate oral antibiotics
- Significant hypoxia (low PaO2, wide A-a gradient)
- More than one lobe involved, empyema, abscess
- Immunosuppression, significant comorbidities (cardiac, pulmonary disease)
- Age extremes (infants <2 months, frail elderly)
- High-risk PSI score or CURB-65 ≥2-3
10. Prevention
-
Annual influenza vaccine for everyone >6 months; especially those >50 years, chronic lung disease, diabetes, immunosuppression
-
Pneumococcal vaccine (PCV13 or PPSV23): all children <5 years, adults ≥65 years, high-risk younger adults
-
Revaccinate after 10 years if first dose was given before age 65
-
Approximately half of adult pneumonia cases can be prevented through vaccination
-
Textbook of Family Medicine 9e
Recent Evidence (2025)
A network meta-analysis (PMID 40602496) published in Clinical Microbiology and Infection (2025) assessed empiric antibiotic therapy for moderate-to-severe CAP and may provide updated comparative data on antibiotic regimen efficacy. A systematic review on drug-resistant pathogens in CAP (PMID 40107661) (2025) highlights evolving resistance patterns that may affect empiric choices. For pediatric Mycoplasma pneumonia, a meta-analysis (PMID 39383346) found tetracyclines to be effective for macrolide-resistant strains in children.
Note: Drug dosing should always be verified against current formulary references before prescribing. This overview is based on Goldman-Cecil Medicine, Fishman's Pulmonary Diseases and Disorders, and Textbook of Family Medicine.
Ecg reading
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
I have excellent content and two key images. I can now write a comprehensive ECG reading guide.
ECG Reading - A Systematic Guide
An ECG (electrocardiogram) records the heart's electrical activity over time from multiple surface electrodes. Reading it systematically prevents missed findings.
The 12-Lead ECG Layout
A standard 12-lead ECG is shown below (normal sinus rhythm, HR 75, from Harrison's Principles of Internal Medicine):
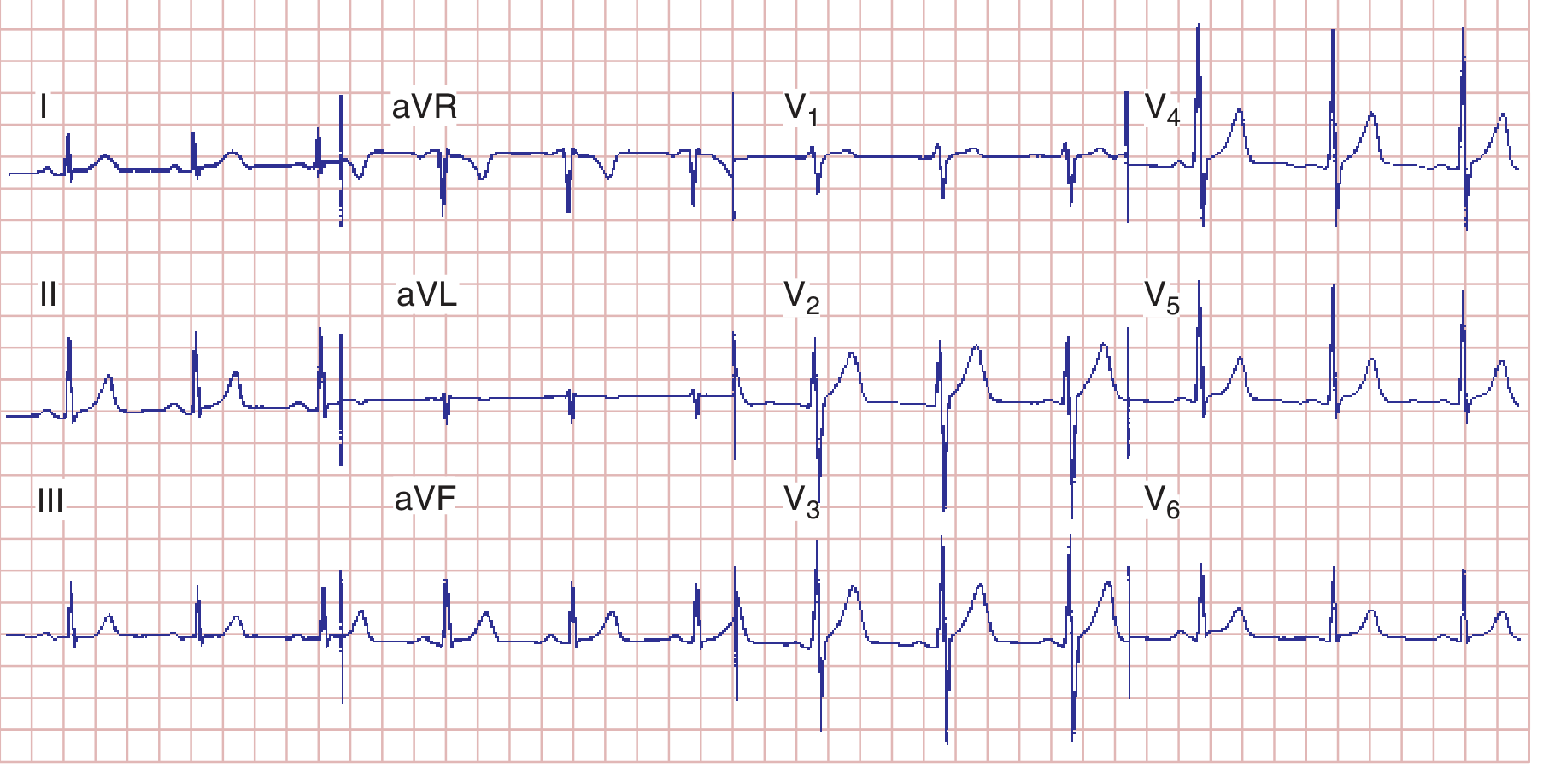
The 12 leads are grouped as:
- Limb leads: I, II, III (bipolar) + aVR, aVL, aVF (augmented unipolar) - view the frontal plane
- Precordial leads: V1-V6 - view the horizontal plane
ECG Paper Calibration
-
Horizontal axis (time): 1 small box = 0.04 sec; 1 large box (5 small) = 0.2 sec; 5 large boxes = 1.0 sec
-
Vertical axis (voltage): 1 small box = 0.1 mV; standard calibration = 10 mm/mV
-
Medical Physiology (Boron & Boulpaep)
The ECG Waveforms
| Wave / Segment | What It Represents |
|---|---|
| P wave | Atrial depolarization (SA node → atria) |
| PR interval | Time for impulse to travel from SA node through AV node to ventricles |
| QRS complex | Ventricular depolarization |
| ST segment | Early ventricular repolarization (isoelectric when normal) |
| T wave | Ventricular repolarization |
| QT interval | Total ventricular electrical systole (depolarization + repolarization) |
Normal Interval Values
| Measurement | Normal Range |
|---|---|
| Heart rate | 60-100 bpm |
| PR interval | 120-200 ms (3-5 small boxes) |
| QRS duration | <120 ms (<3 small boxes) |
| QT interval | <440 ms men; <460 ms women (varies with HR) |
| P wave amplitude | <2.5 mm |
| P wave duration | <120 ms |
Example normal values: PR 160 ms, QRS 80 ms, QT 360 ms, QTc ~390 ms, axis +70°.
- Harrison's Principles of Internal Medicine, 22e
Step-by-Step ECG Reading Approach
Step 1 - Heart Rate
Quick method: Count large boxes between two R waves, divide 300 by that number.
- 1 large box = 300 bpm | 2 = 150 | 3 = 100 | 4 = 75 | 5 = 60 | 6 = 50
Step 2 - Rhythm
Ask: Is there a P wave before every QRS? Is the R-R interval regular? Is the pacemaker the SA node?
- Normal sinus rhythm: Rate 60-100, regular P before each QRS, P upright in II and inverted in aVR
- Sinus tachycardia: Rate >100, same pattern
- Sinus bradycardia: Rate <60, same pattern
- Atrial fibrillation: No discrete P waves, irregularly irregular R-R intervals
- Atrial flutter: Sawtooth flutter waves at ~300/min, typically 2:1 or 4:1 block
Step 3 - P Wave
- Normal: upright in I, II, aVF, V4-V6; inverted in aVR
- Right atrial overload ("P pulmonale"): Tall peaked P ≥2.5 mm
- Left atrial abnormality ("P mitrale"): Broad notched P ≥120 ms in limb leads; biphasic P in V1 with prominent negative terminal component
Step 4 - PR Interval
- Short PR (<120 ms): Pre-excitation (WPW syndrome) - look for delta wave
- Long PR (>200 ms): 1st-degree AV block
- Progressive lengthening then dropped QRS: 2nd-degree Mobitz I (Wenckebach)
- Constant PR then dropped QRS: 2nd-degree Mobitz II
- No relationship between P and QRS: 3rd-degree (complete) AV block
Step 5 - QRS Complex
- Normal duration <120 ms - narrow complex
- QRS ≥120 ms: Bundle branch block, ventricular rhythm, or pre-excitation
- Right Bundle Branch Block (RBBB): rSR' ("rabbit ears") in V1, wide S wave in V6, T wave inversion in V1-V3
- Left Bundle Branch Block (LBBB): Broad QS or rS in V1, tall broad R in V6, T wave inversion in lateral leads
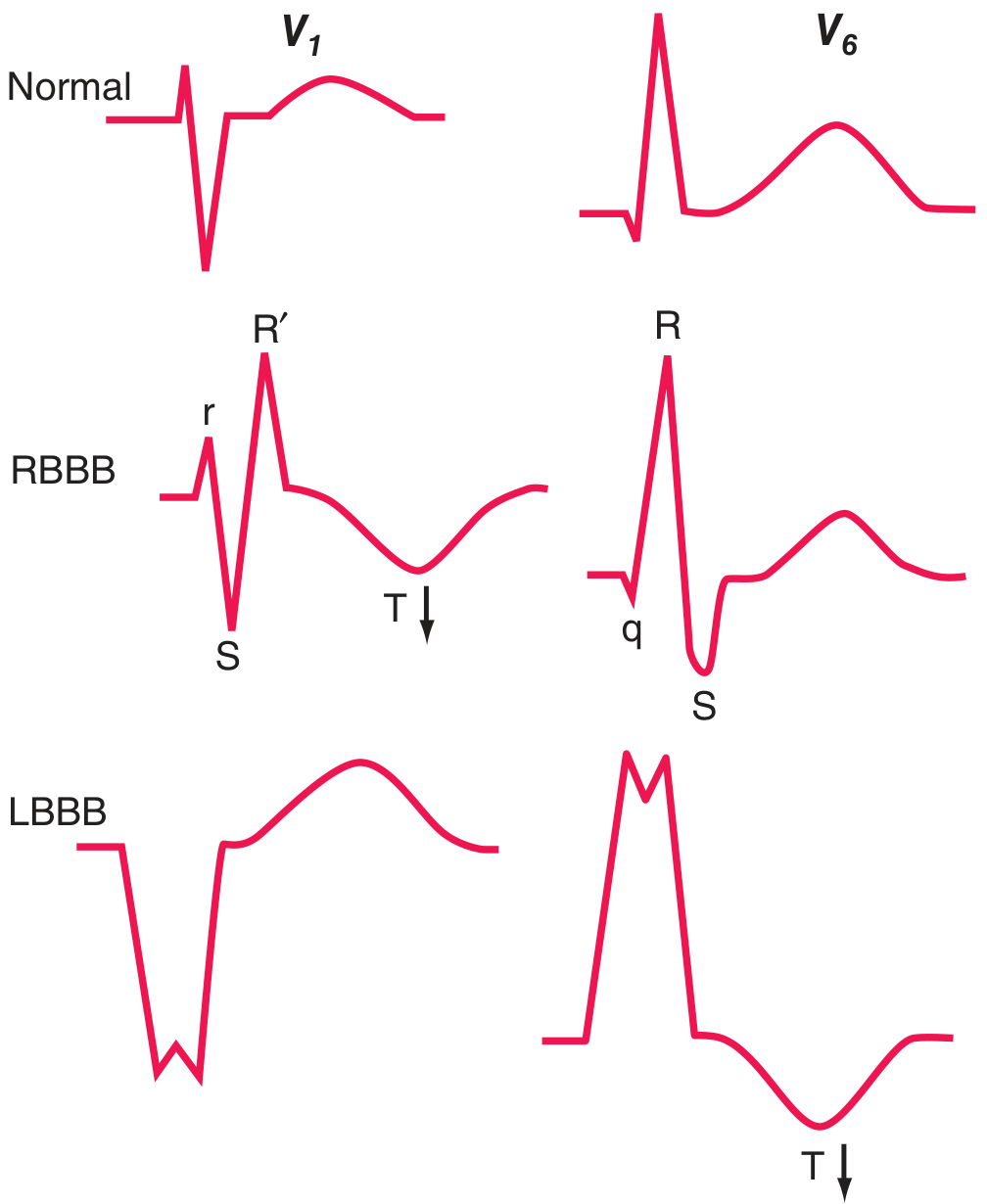
Top row: Normal. Middle row: RBBB showing rSR' (rabbit ears) in V1 and qRS in V6 with T wave inversion. Bottom row: LBBB showing broad QS in V1 and wide tall R in V6 with T inversion.
- Harrison's Principles of Internal Medicine, 22e
Step 6 - Axis
Normal axis: -30° to +90°
| Axis | Lead I | Lead aVF | Cause |
|---|---|---|---|
| Normal | Positive | Positive | - |
| Left axis deviation (<-30°) | Positive | Negative | LBBB, left anterior fascicular block, inferior MI |
| Right axis deviation (>+90°) | Negative | Positive | RBBB, RVH, pulmonary hypertension, left posterior fascicular block |
| Extreme/Northwest | Negative | Negative | VT, severe RVH |
Left anterior fascicular block: QRS axis more negative than -45° - most common cause of marked left axis deviation in adults.
Left posterior fascicular block: QRS axis >+110° - rare, only after excluding other causes of right axis deviation.
Step 7 - ST Segment
The ST segment should be isoelectric. Deviations are clinically critical:
ST Elevation - key causes:
- STEMI: Convex (domed) upward ST elevation in contiguous leads
- Anterior: V1-V4 (LAD territory)
- Inferior: II, III, aVF (RCA or LCx territory)
- Lateral: I, aVL, V5-V6 (LCx territory)
- Pericarditis: Diffuse concave (saddle-shaped) ST elevation in all leads except aVR; PR depression in inferior leads and V6; PR elevation in aVR
- Benign early repolarization: Concave ST elevation V2-V5, notching at J point, stable over time, common in young adults
- LBBB or LVH: Secondary ST changes - can mimic STEMI
ST Depression - key causes:
- Subendocardial ischemia / NSTEMI
- Posterior MI (V1-V4 depression = reciprocal change; confirm with posterior leads V7-V9)
- Digoxin effect ("reverse tick" or scoop-shaped)
- Reciprocal changes in non-infarcted leads
Transmural ischemia: severe acute ischemia lowers resting membrane potential and shortens action potential duration, creating a voltage gradient between normal and ischemic zones - this manifests as ST elevation. Subendocardial ischemia shifts the ST vector toward the endocardium, producing precordial ST depression.
- Harrison's Principles of Internal Medicine, 22e
Step 8 - T Wave
- Normal: Positive in I, II, V3-V6; inverted in aVR; variable in III, V1, V2
- T wave inversion: Ischemia, LVH, RVH ("strain"), bundle branch blocks, pulmonary embolism
- Hyperacute T waves: Tall, broad, symmetric - earliest sign of STEMI
- Peaked narrow T waves: Hyperkalemia
Step 9 - QT Interval
- Always correct for heart rate: QTc = QT / √(R-R interval in seconds) (Bazett formula)
- Prolonged QTc: Risk of Torsades de Pointes - causes include hypokalemia, hypomagnesemia, drugs (antiarrhythmics, antibiotics, antipsychotics), congenital long QT syndrome
- Short QT: Hypercalcemia, digoxin toxicity
Lead Territories for MI Localization
| Territory | Leads Showing Changes | Artery |
|---|---|---|
| Anterior | V1-V4 | Left anterior descending (LAD) |
| Anterolateral | V4-V6, I, aVL | LAD or diagonal branch |
| Inferior | II, III, aVF | Right coronary artery (RCA) |
| Lateral | I, aVL, V5-V6 | Left circumflex (LCx) |
| Posterior | ST depression V1-V3 (reciprocal); ST elevation in V7-V9 | RCA or LCx |
| Right ventricle | ST elevation V3R-V6R | RCA proximal |
Check for right ventricular infarction with right-sided chest leads (V3R-V6R) in inferior MI - ST elevation in RV leads confirms RV involvement.
- Rosen's Emergency Medicine
Common Arrhythmia Patterns at a Glance
| Arrhythmia | Key Features |
|---|---|
| Premature atrial beat (PAC) | Early narrow QRS, abnormal P morphology, incomplete compensatory pause |
| Premature ventricular beat (PVC) | Early wide QRS (≥120 ms), no preceding P, full compensatory pause |
| SVT | Regular narrow tachycardia, P often buried in QRS or retrograde |
| VT | Regular wide-complex tachycardia, AV dissociation, fusion/capture beats |
| AF | No P waves, irregular R-R, fibrillatory baseline |
| Atrial flutter | Sawtooth P waves ~300/min, regular rate (150 if 2:1 block) |
| WPW | Short PR, delta wave, wide QRS |
| Complete AV block (3rd degree) | P and QRS completely independent, slow ventricular escape rhythm |
Quick Memory Checklist (RRATES)
| Step | Check |
|---|---|
| Rate | Count - tachycardia, bradycardia, or normal? |
| Rhythm | Regular or irregular? Sinus or not? |
| Axis | Normal, LAD, or RAD? |
| Time intervals | PR, QRS, QT - prolonged or short? |
| Events (ST/T) | ST elevation or depression? T wave changes? |
| Size | P wave, QRS voltages - hypertrophy? |
Note: ECG interpretation must always be integrated with the clinical picture. A single finding rarely makes a diagnosis in isolation. Drug effects, electrolyte abnormalities, and technical issues (lead placement, electrical interference) can all alter the ECG.
Sources: Medical Physiology (Boron & Boulpaep); Harrison's Principles of Internal Medicine, 22e; Rosen's Emergency Medicine; Braunwald's Heart Disease.
This is a shared conversation. Sign in to Orris to start your own chat.