Describe the surgical anatomy of pelvic organ support system. (b) What are the etiological factors of pelvic organ prolapse in a 30 years old woman. (c) Describe basic principles of surgical correction of enterocele.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed. Let me compose the comprehensive answer.
Pelvic Organ Support System, Prolapse Etiology, and Enterocele Repair
(a) Surgical Anatomy of the Pelvic Organ Support System
The support of pelvic organs depends on three interrelated components working together: the levator ani muscle complex, the endopelvic fascia and ligamentous condensations, and the bony pelvic attachments.
1. The Pelvic Diaphragm (Primary Muscular Support)
The pelvic diaphragm is a funnel-shaped fibromuscular partition that forms the primary supporting structure for the pelvic contents. It is composed of:
- Levator ani - the dominant component, which itself consists of:
- Pubococcygeus (including pubovaginalis and pubourethralis subdivisions)
- Puborectalis
- Iliococcygeus
- Coccygeus muscle
The levator ani arises from the arcus tendineus levator ani (ATLA) - a thickening of the obturator fascia extending from the body of the pubis to the ischial spine - and inserts into the central tendon of the perineum, wall of the anal canal, anococcygeal ligament, coccyx, and vaginal wall. It is innervated by S3-S4 and the inferior rectal nerve.
The opening between the levator ani muscles through which the urethra, vagina, and rectum pass is the levator hiatus. The levator ani provides a stable base (levator plate) upon which pelvic organs rest; it assists the abdominal wall in containing pelvic contents and supports the posterior vaginal wall.
The urogenital diaphragm lies inferior to the pelvic diaphragm and consists of the deep transverse perineal muscle and the sphincter urethrae, anchoring the distal urethra and vagina.
2. Endopelvic Fascia and Ligamentous Support
The endopelvic fascia is a continuous sheet of connective tissue investing the pelvic organs; specific condensations form the major ligamentous supports:
| Structure | Attachment | Support Role |
|---|---|---|
| Cardinal (Mackenrodt's) ligament | Cervix/upper vagina → pelvic sidewall | Primary lateral support of cervix |
| Uterosacral ligaments | Posterior cervix → sacrum (S2-S4) | Posterior suspension; prevents descent |
| Pubocervical fascia | Pubis → cervix, anteriorly | Anterior vaginal wall support |
| Rectovaginal (Denonvilliers') fascia | Vagina → rectum, posteriorly | Posterior vaginal wall support |
| Arcus tendineus fasciae pelvis (ATFP) | Pubis → ischial spine | Lateral attachment of midvagina |
3. DeLancey's Three Levels of Support
The most clinically applicable framework is DeLancey's three-level system (1992), based on cadaveric dissections:
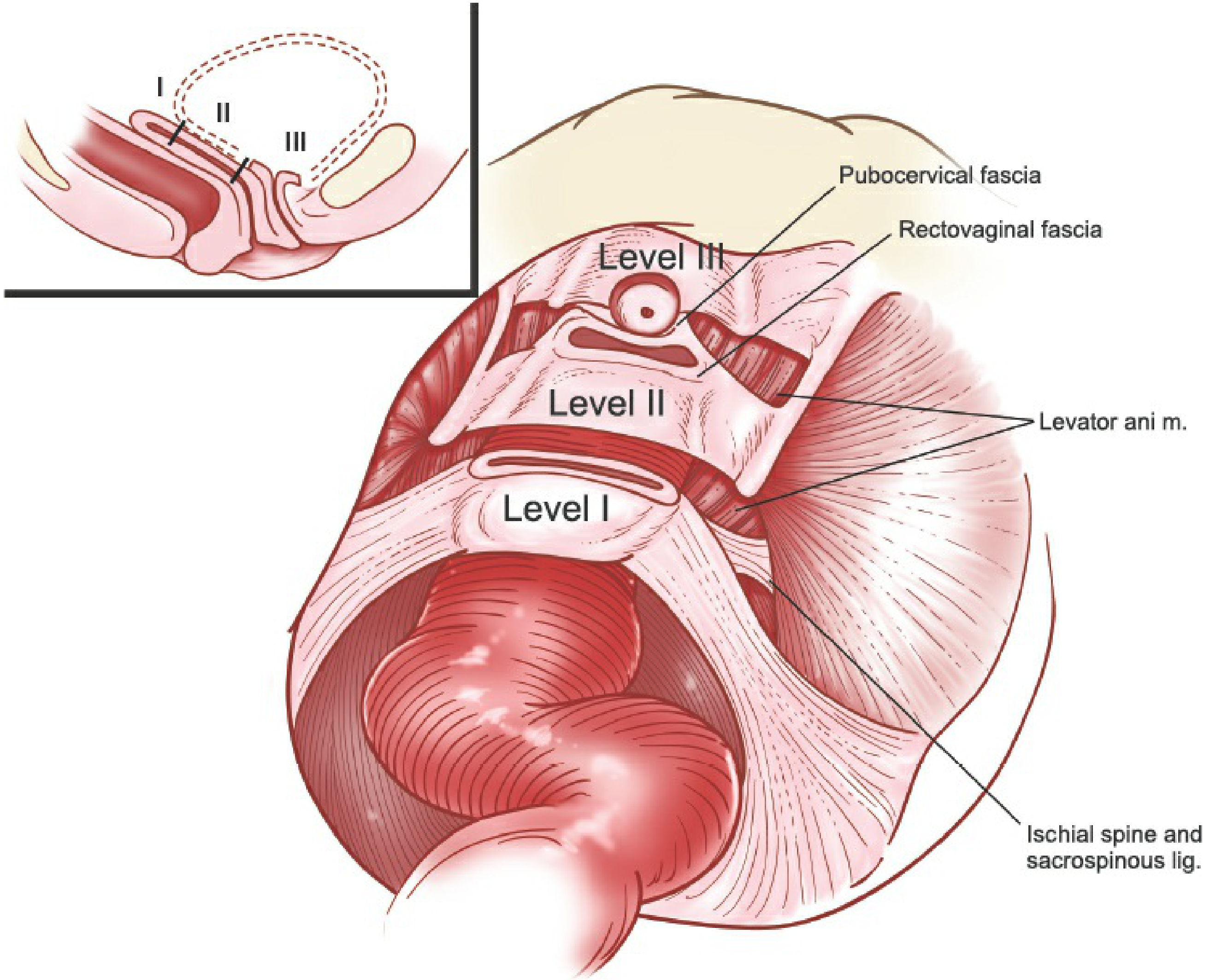
Level I - Apical/Suspensory Support
- Composed of the cardinal-uterosacral ligament complex (parametrium and paracolpium)
- Suspends the cervix and upper one-third of vagina from the sacrum and lateral pelvic sidewall
- The paracolpium's vertical fibers form the critical structure distinguishing uterovaginal prolapse from vault prolapse post-hysterectomy
- Loss of Level I → uterine prolapse or vaginal vault prolapse
Level II - Lateral Attachment (Mid-vagina)
- The paracolpium changes from vertical suspension to a direct lateral attachment of the midvagina to the ATFP (arcus tendineus fasciae pelvis) anteriorly and to the superior fascia of the levator ani
- Laterally, the pubocervical fascia anteriorly and rectovaginal fascia posteriorly constitute this level
- Loss of Level II → cystocele (anterior) or rectocele (posterior)
- Lateral detachment = paravaginal defect
- Midline weakness = central defect
Level III - Distal Fusion
- The distal vagina fuses with surrounding structures:
- Anteriorly: vagina fuses with the urethra (pubourethral ligaments, pubovesical fascia)
- Laterally: fuses with the levator ani muscles
- Posteriorly: anchored to the perineal body via the rectovaginal fascia
- Loss of Level III → urethral hypermobility and stress urinary incontinence, distal rectocele
4. Perineal Body
The central perineal tendon (perineal body) is the fibromuscular node at the center of the perineum where the bulbospongiosus, superficial and deep transverse perineal muscles, external anal sphincter, and pubovaginalis converge. It provides structural integrity to the posterior introitus and is commonly disrupted in obstetric perineal lacerations.
5. Surgical Relevance
- All three levels of defective support must be repaired during reconstructive surgery
- Apical support is the keystone: anterior and posterior repairs performed without addressing apical defects carry high recurrence rates
- Pelvic vessels (uterine, vaginal arteries) provide condensations of endopelvic fascia that reinforce organ position
(Sources: Berek & Novak's Gynecology; Campbell-Walsh-Wein Urology)
(b) Etiological Factors of Pelvic Organ Prolapse in a 30-Year-Old Woman
POP in a young woman is almost always the result of a combination of factors. The cause is multifactorial.
1. Obstetric and Reproductive Factors (Most Significant)
- Vaginal childbirth - the single strongest risk factor. Parity shows the highest adjusted relative risk for POP in the Oxford Family Planning Study (RR 8.4 for two deliveries, RR 10.85 for four or more deliveries). Each additional delivery increases POP risk by 10-20%
- Instrumental delivery (forceps) - OR 5.4 for requiring prolapse surgery vs. OR 2.9 for normal vaginal delivery; forceps delivery causes direct levator ani avulsion and fascial disruption
- Age <25 years at first delivery - identified as a specific risk factor for requiring prolapse surgery, as younger perineal tissue may sustain greater unrecognized injury
- Prolonged second stage of labour - prolonged levator ani compression and stretching
- Large birth weight infant (>4 kg) - mechanical distension of pelvic floor structures
- Grand multiparity - cumulative obstetric trauma
2. Congenital and Connective Tissue Disorders
- Congenital weakness of connective tissue - some women have inherently deficient collagen quality; variants in COL3A1 and COL1A1 genes affect pelvic fascia
- Ehlers-Danlos syndrome and other heritable connective tissue disorders - associated with early-onset prolapse
- Marfan syndrome - connective tissue laxity
- Spina bifida occulta - sacral nerve deficiency undermines pelvic muscle tone
- Congenital absence or malformation of supporting structures (rare)
3. Hormonal Factors
- Oestrogen plays a key role in maintaining collagen integrity in pelvic support structures. Even in young women, relative hypoestrogenic states (e.g., prolonged lactation, premature menopause, GnRH agonist therapy) weaken fascial tissues
4. Increased Intra-abdominal Pressure (Chronic)
- Obesity - BMI >30 kg/m² increases risk of uterine prolapse by 40%, rectocele by 75%, cystocele by 57% (Women's Health Initiative). The mechanism is persistent elevation of intra-abdominal pressure transmitted to pelvic floor
- Chronic cough (asthma, chronic bronchitis, smoking)
- Chronic straining/constipation - repeated Valsalva bearing-down
- Heavy lifting/manual labour - especially relevant in young working-age women
- Ascites or large pelvic/abdominal masses
5. Previous Pelvic Surgery
- Hysterectomy - disrupts the cardinal-uterosacral ligament complex if vault suspension is not performed; cumulative risk of prolapse surgery rises to 5% at 15 years post-hysterectomy
- Failure to perform concurrent vault suspension at the time of hysterectomy is a major preventable cause of subsequent vault prolapse in young women
6. Neurological and Muscular Factors
- Pudendal nerve injury - during labour or surgery; denervation of levator ani leads to progressive muscle atrophy and pelvic floor weakness
- Spinal cord disease - MS, spinal cord injury; loss of pudendal and sacral nerve tone
- Myopathies - congenital or acquired disorders of levator ani
7. Racial Factors
- Hispanic and Asian women have a statistically higher risk of cystocele vs. white women; African-American women have a lower risk. These differences likely reflect variations in collagen subtype distribution and pelvic architecture
Summary for a 30-Year-Old
In a young woman aged 30, the dominant aetiological factors are obstetric trauma (early/multiple vaginal deliveries, instrumental delivery), underlying connective tissue abnormality, and chronic raised intra-abdominal pressure. A careful history for all these factors should be taken.
(Source: Campbell-Walsh-Wein Urology, "Risk Factors for Pelvic Organ Prolapse")
(c) Basic Principles of Surgical Correction of Enterocele
Definition
An enterocele is a true hernia of the peritoneal sac containing small bowel or omentum that protrudes through a defect in the rectovaginal or pubocervical fascia, most commonly at the vaginal apex. It represents failure of Level I support.
Goals of Surgery
The three core principles that must be simultaneously addressed are:
- Obliterate/excise the peritoneal (hernia) sac - eliminate the hernial space
- Suspend the vaginal apex - correct the underlying Level I defect, restoring normal apical support without tension
- Repair the fascial defect - correct the specific fascial defect in the pubocervical and/or rectovaginal fascia
Methods for Peritoneal Sac Management
A. Excision with peritoneal closure
- Incise vaginal epithelium at the apex and dissect it away from underlying fascia circumferentially
- Identify the enterocele sac by palpating the prolapsing tissue to confirm no bowel is trapped
- Incise the sac, inspect the abdominal cavity for adhesions or pathology
- Pack bowel superiorly with a moistened laparotomy sponge (Trendelenburg position assists)
- Place a purse-string suture (2-0 non-absorbable) circumferentially around the base of the sac extending into the peritoneal cavity - the entire hernia sac must be ligated
- Uterosacral ligaments, when visualised, are incorporated into the purse-string for reinforcement
- A second purse-string suture may be added for security
- A finger is kept in the peritoneal cavity as the suture is tied to ensure no bowel is incorporated
B. Reduction with sac closure (without excision)
- Dissect and reduce the peritoneal sac without excising it
- Suture the defect closed
C. Transabdominal obliteration
- Halban procedure - multiple sagittal sutures placed through the peritoneum of the cul-de-sac, obliterating the pouch of Douglas
- Moschcowitz procedure - concentric purse-string sutures placed around the pouch of Douglas from above
D. Transvaginal obliteration
- McCall culdoplasty - transvaginal sutures incorporating the uterosacral ligaments and posterior peritoneum to obliterate the cul-de-sac; the gold standard at vaginal hysterectomy
- Transvaginal Halban procedure
E. Redundant posterior vaginal wall
- If the posterior vaginal wall is significantly elongated and redundant, excess vaginal wall is excised to restore acceptable vaginal length and eliminate redundancy
Apical Suspension (Vault Support - Essential)
After peritoneal sac management, the vaginal apex must be resuspended. This is the single most important step, as enterocele recurs without adequate apical support.
Uterosacral Ligament Suspension (ULS)
- Suspension sutures are pre-placed into the bilateral uterosacral ligaments under direct visualisation (ideally before final sac closure)
- Central fascial defect is repaired first with 2-0 absorbable plication sutures to reapproximate pubocervical and/or rectovaginal fascia
- Double-armed non-absorbable (no. 0) sutures are then passed through the plicated fascia; as sutures are tied, the apex is resuspended to the uterosacral ligaments
- Risk: ureteral kinking - ureteral integrity must be confirmed by cystoscopy
Sacrospinous Ligament Fixation
- The vaginal incision is extended laterally; the sacrospinous ligament (and attached coccygeus muscle) is identified through the pararectal space
- Suspension sutures are placed two finger-breadths medial to the ischial spine (to avoid the pudendal neurovascular bundle which exits through the lesser sciatic foramen just medial and inferior to the ischial spine)
Sacrocolpopexy (Abdominal/Laparoscopic)
- For complex cases or recurrent prolapse, the vaginal apex is attached to the sacral promontory via a mesh bridge
Concurrent Repairs
- Fascial plication - the pubocervical and rectovaginal fascia are reapproximated in the midline with absorbable sutures after the hernia sac is managed
- Posterior colporrhaphy if coexisting rectocele is present
- Urodynamic assessment pre-operatively to plan concurrent anti-incontinence procedures if indicated
Key Surgical Hazards
- Ureteral injury - particularly during uterosacral suture placement (ureters lie 0.9 cm lateral to uterosacral ligaments)
- Bowel injury - especially when the sac is opened or purse-string sutures are placed
- Rectal injury - when dissecting the rectovaginal space
- Pudendal neurovascular bundle injury - during sacrospinous fixation
(Sources: Berek & Novak's Gynecology, pp. 1620-1622; Hinman's Atlas of Urologic Surgery, p. 697)
This is a shared conversation. Sign in to Orris to start your own chat.