Explain rebal physiology and clinical related to it with pictures
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have 6 excellent medical diagrams and comprehensive content covering all major aspects of renal physiology. I have enough material to write a thorough, well-illustrated response. Let me now compose the full answer.
Renal Physiology - Complete Guide with Pictures
1. Functional Anatomy: The Nephron
Each kidney contains approximately 1 million nephrons - the functional unit of urine formation. A nephron consists of a glomerulus enclosed in Bowman's capsule, followed by the proximal convoluted tubule (PCT), loop of Henle, distal convoluted tubule (DCT), and collecting duct.
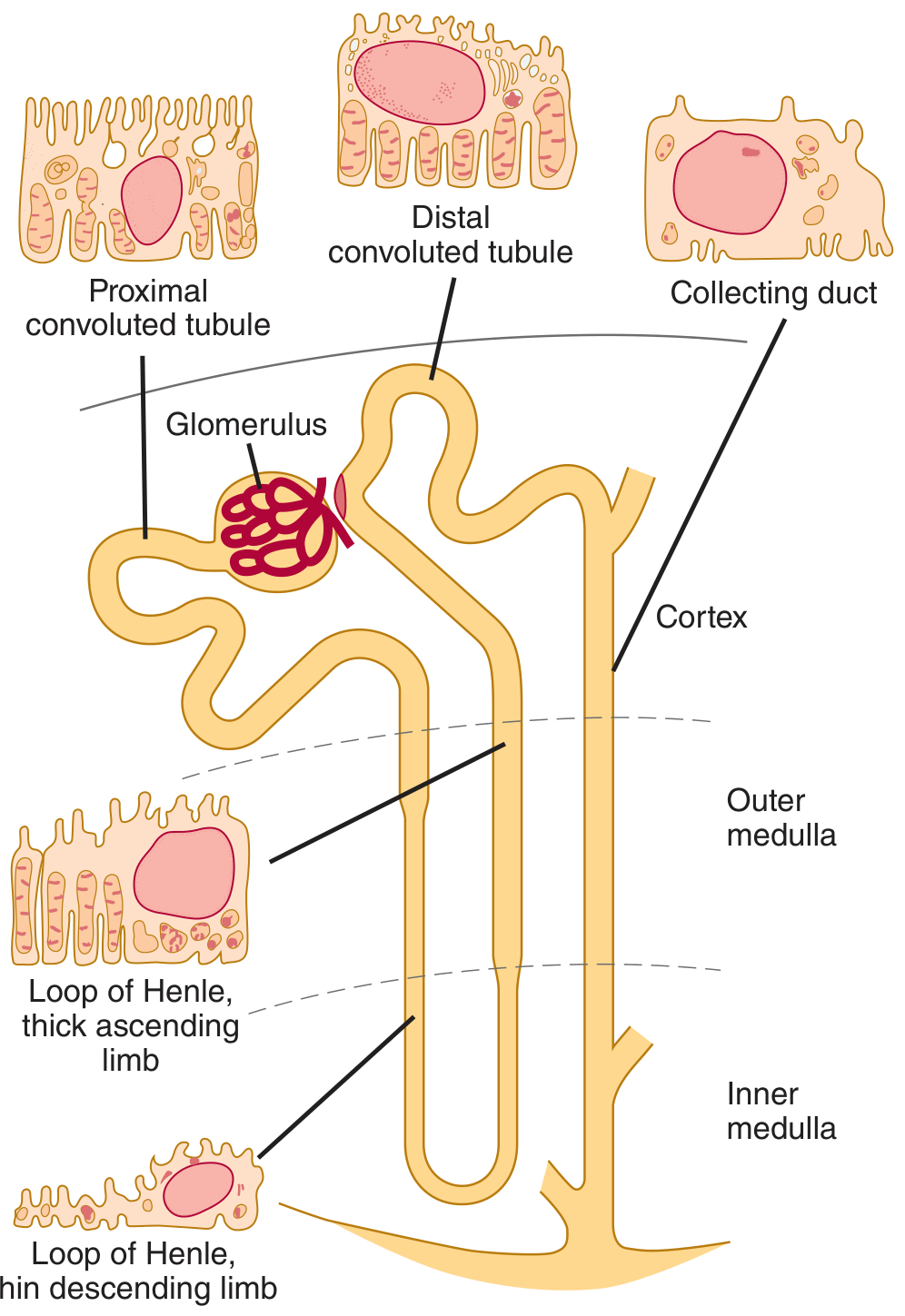
Figure 1 - Nephron structure (Ganong's Review of Medical Physiology). Each segment has distinct cell morphology and function: the PCT has a brush border for reabsorption, the loop of Henle has thin descending and thick ascending limbs, and the collecting duct is responsive to ADH.
There are two functionally distinct nephron types:
- Cortical nephrons (~85%): Short loops of Henle, mainly regulate ECF composition
- Juxtamedullary nephrons (~15%): Long loops of Henle that dip deep into the medulla - responsible for producing concentrated urine. Their efferent arterioles give rise to the vasa recta, hairpin vessels that run alongside the loop of Henle.
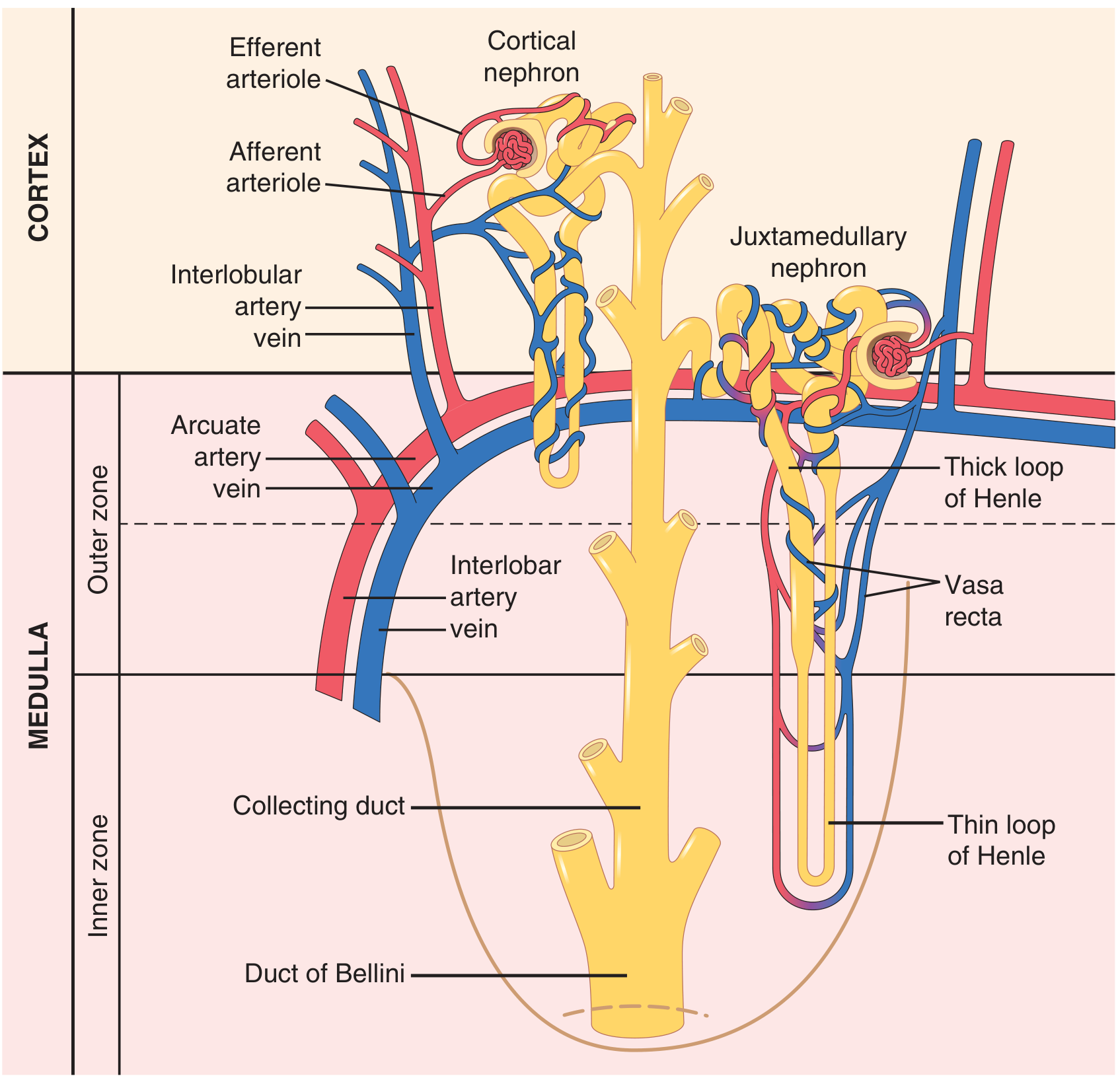
Figure 2 - Cortical and juxtamedullary nephrons with their vascular supply (Guyton & Hall). Note the vasa recta forming hairpin loops alongside the juxtamedullary loop of Henle.
2. The Glomerulus - The Filtration Barrier
The glomerulus is a tuft of capillaries (~200 µm diameter) formed between an afferent arteriole (wider) and an efferent arteriole (narrower). This arrangement creates a high hydrostatic pressure that drives filtration.
The filtration barrier has three layers:
- Fenestrated endothelium - pores 70-90 nm, prevents blood cells
- Glomerular basement membrane (GBM) - negatively charged, excludes large proteins
- Podocyte foot processes - 25 nm filtration slits, the final sieve
Also present: Mesangial cells - contractile cells that modulate GFR and phagocytose immune complexes. Macula densa (in DCT) senses NaCl delivery and regulates renin release via tubuloglomerular feedback.
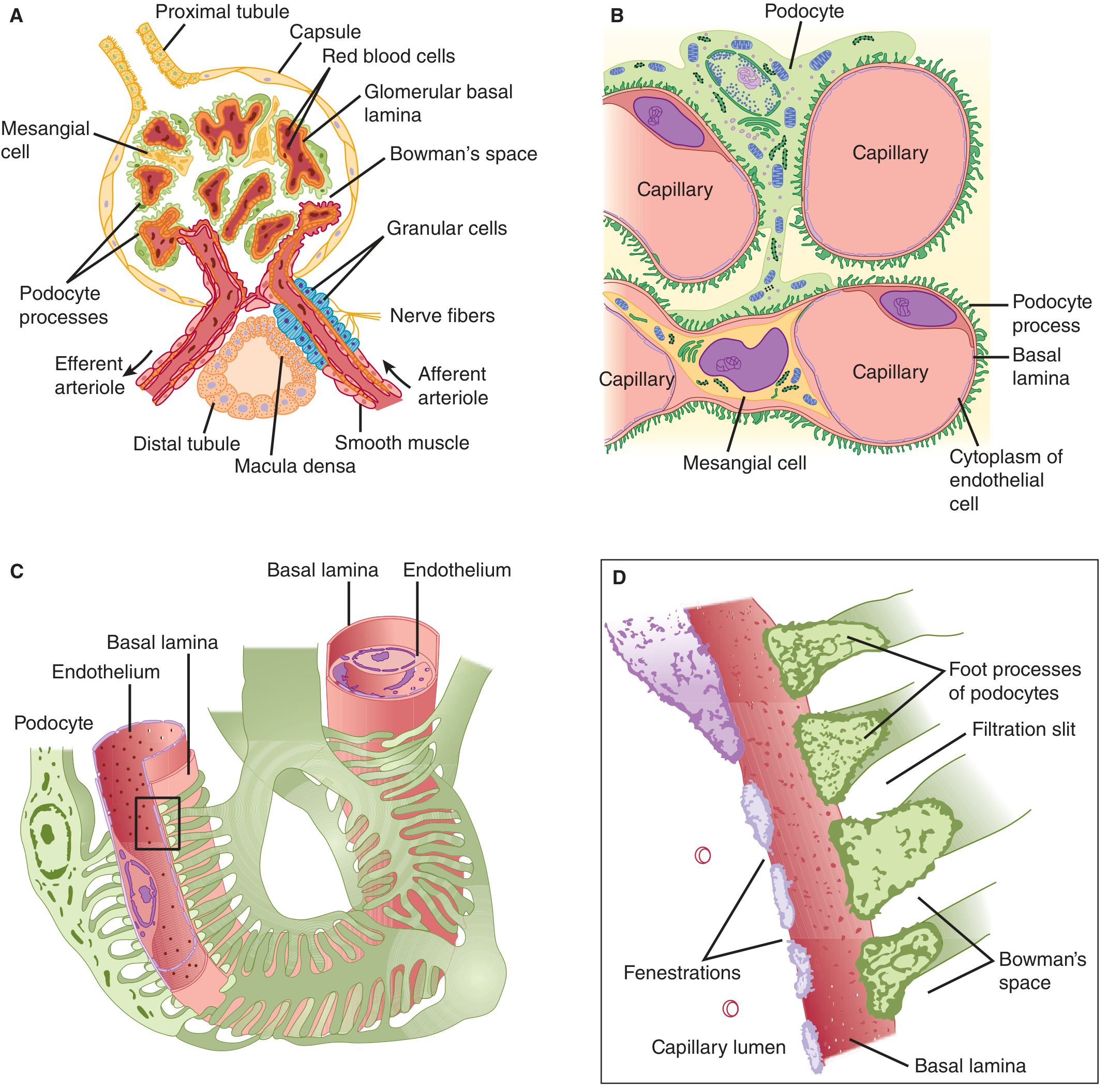
Figure 3 - Structural details of the glomerulus (Ganong's). A) Vascular pole with mesangial cells and macula densa. B) Podocytes around capillaries. C-D) Foot processes, filtration slits, fenestrations, and Bowman's space.
Clinical link - Nephrotic syndrome: Damage to podocyte foot processes (minimal change disease) or the GBM (membranous nephropathy) breaks the filtration barrier. Result: massive proteinuria (>3.5 g/day), hypoalbuminaemia, and oedema.
Clinical link - Nephritic syndrome: Inflammation of mesangial cells and endothelium (e.g. IgA nephropathy, post-streptococcal GN). Result: haematuria, RBC casts, and reduced GFR.
3. The Three Core Renal Processes
Urine formation = Filtration - Reabsorption + Secretion
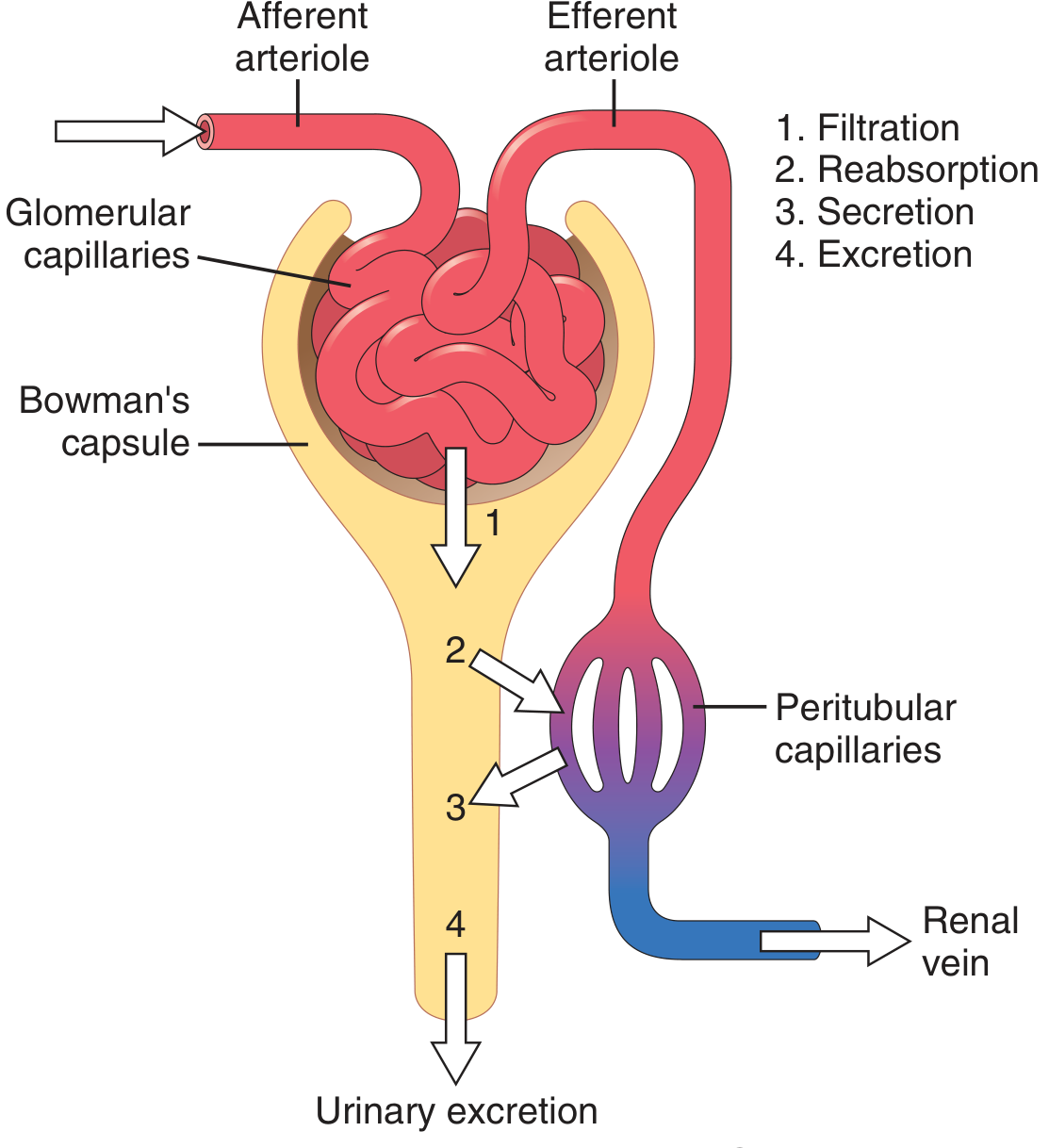
Figure 4 - The four basic kidney processes (Guyton & Hall). Blood enters via the afferent arteriole, is filtered at the glomerulus, and the filtrate is modified by the tubules before final excretion.
- Freely filtered only (e.g. inulin, creatinine): excreted = filtered load → used to measure GFR
- Filtered + partially reabsorbed (e.g. Na⁺, Cl⁻, water): regulated to maintain homeostasis
- Filtered + completely reabsorbed (e.g. glucose, amino acids): none appears in urine under normal conditions
- Filtered + secreted (e.g. K⁺, H⁺, PAH, many drugs): rapid clearance from blood
4. Glomerular Filtration Rate (GFR)
Normal GFR ≈ 125 mL/min (180 L/day filtered; ~1-2 L excreted as urine).
GFR is governed by the Starling forces across the filtration membrane:
GFR = Kf × (P_GC - P_BS - π_GC + π_BS)
Where:
- Kf = filtration coefficient (permeability × area)
- P_GC = glomerular capillary hydrostatic pressure (~60 mmHg) - promotes filtration
- P_BS = Bowman's space pressure (~18 mmHg) - opposes filtration
- π_GC = glomerular oncotic pressure (~32 mmHg) - opposes filtration
- π_BS = Bowman's space oncotic pressure (≈0) - promotes filtration
Net filtration pressure ≈ 10 mmHg.
Measuring GFR:
- Gold standard: inulin clearance (freely filtered, not secreted or reabsorbed)
- Clinical surrogate: serum creatinine and eGFR (CKD-EPI or MDRD equations)
- Near-gold standard: creatinine clearance (slight overestimation due to tubular secretion)
5. Renal Autoregulation
The kidney maintains relatively constant blood flow and GFR despite arterial pressure changes from ~70-220 mmHg, through two mechanisms:
- Myogenic mechanism: Stretch of afferent arteriole smooth muscle → vasoconstriction
- Tubuloglomerular feedback (TGF): Macula densa senses ↑NaCl delivery → constricts afferent arteriole via adenosine and thromboxane → reduces GFR
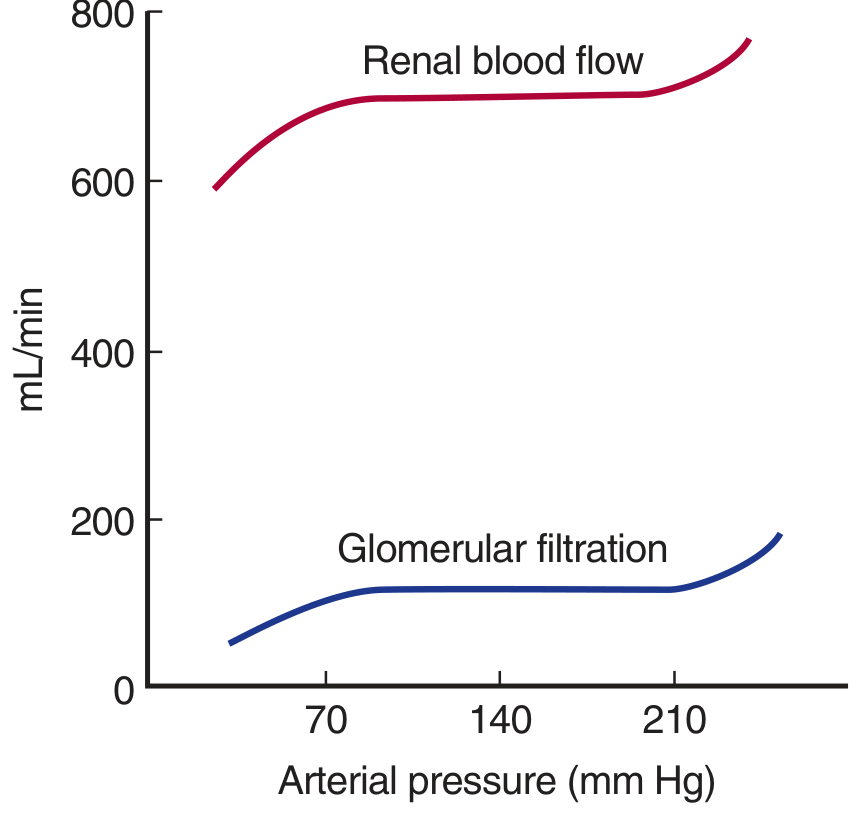
Figure 5 - Autoregulation of renal blood flow (RBF) and GFR (Ganong's). Both RBF and GFR are kept relatively constant across a wide range of arterial pressures (70-220 mmHg).
Clinical link - ACE inhibitors in CKD: Efferent arteriolar tone maintained by angiotensin II preserves GFR when renal perfusion is reduced. ACEi/ARBs dilate the efferent arteriole → reduce intraglomerular pressure → can cause an acute ↑ in creatinine (acceptable up to 30% rise). This effect is actually renoprotective long-term in diabetic nephropathy. However, in bilateral renal artery stenosis, removing Ang II support can cause acute renal failure.
6. Tubular Function - Segment by Segment
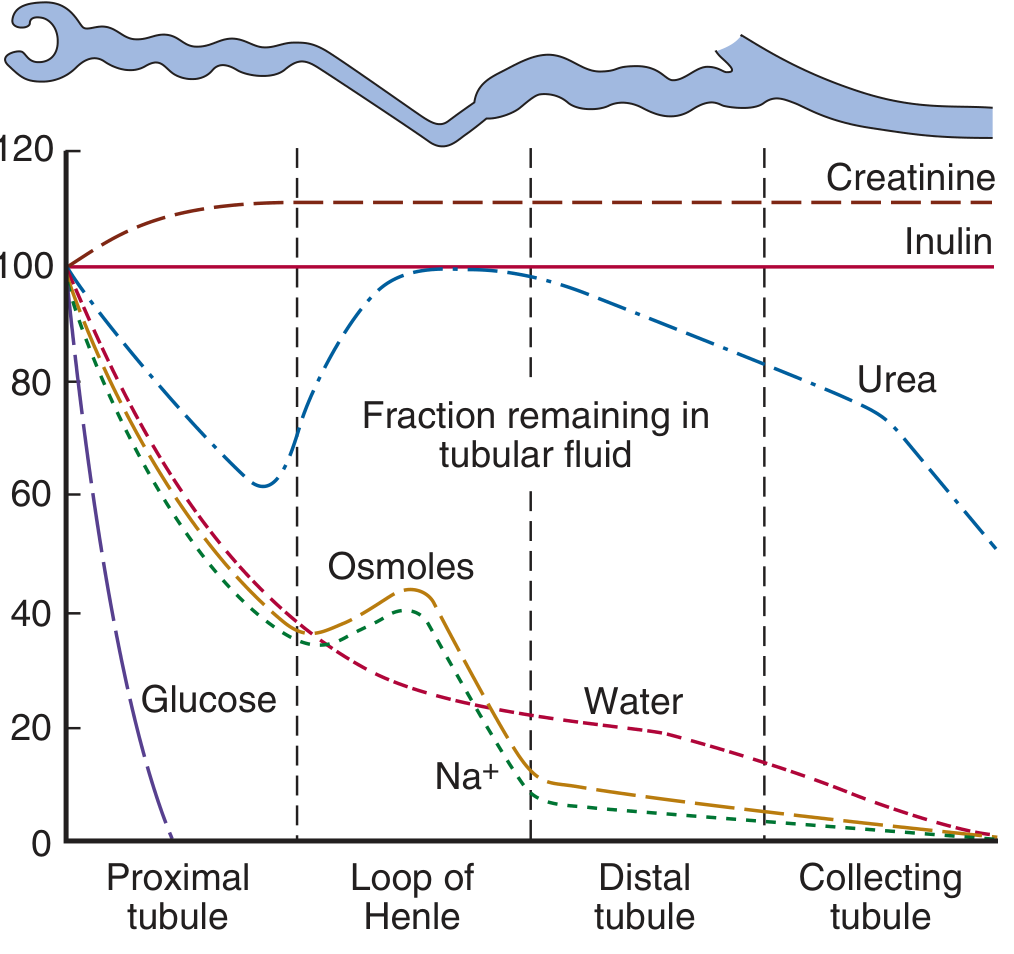
Figure 6 - Fraction of filtered substances remaining in tubular fluid along the nephron (Ganong's). Glucose is completely reabsorbed in the PCT. Na⁺ and water progressively reabsorbed. Creatinine and inulin remain at 100% (creatinine slightly secreted, so exceeds 100%).
A. Proximal Convoluted Tubule (PCT)
- Reabsorbs 60-70% of filtered Na⁺, water, HCO₃⁻, K⁺, Cl⁻, glucose, amino acids, phosphate
- Fluid remains iso-osmotic (aquaporin-1 channels allow obligate water reabsorption)
- Apical brush border with Na⁺-glucose cotransporter (SGLT2), Na⁺-H⁺ exchanger (NHE3)
- Secretes organic acids, drugs (e.g. penicillin), urate
Clinical link - Fanconi syndrome: PCT dysfunction causes loss of glucose, phosphate, amino acids, uric acid, K⁺, and HCO₃⁻ in urine. Causes: multiple myeloma, cisplatin toxicity, tenofovir (HIV drugs), Wilson disease.
Clinical link - SGLT2 inhibitors (gliflozins): Block SGLT2 in the PCT → glycosuria → lower blood glucose in T2DM. Also reduce intraglomerular pressure (via tubuloglomerular feedback), slowing CKD progression.
B. Loop of Henle
- Thin descending limb: permeable to water (aquaporin-1), impermeable to solutes → fluid becomes hyperosmotic
- Thick ascending limb (TAL): impermeable to water; actively reabsorbs Na⁺-K⁺-2Cl⁻ via NKCC2 cotransporter → the "diluting segment" - fluid becomes hypotonic
- Creates the medullary concentration gradient (up to 1200 mOsm/kg at the papilla)
Clinical link - Loop diuretics (furosemide, bumetanide): Block NKCC2 in the TAL → prevent concentration gradient formation → massive natriuresis and diuresis. Used in: pulmonary oedema, heart failure, hypercalcaemia, severe hypertension.
C. Distal Convoluted Tubule (DCT)
- Reabsorbs Na⁺ and Cl⁻ via NCC (Na⁺-Cl⁻ cotransporter), impermeable to water
- Fine-tuning of Ca²⁺ reabsorption (stimulated by PTH)
Clinical link - Thiazide diuretics (hydrochlorothiazide, indapamide): Block NCC → natriuresis. Paradoxically reduce urine volume in nephrogenic diabetes insipidus (by causing mild volume depletion → increased PCT reabsorption). Also reduce urinary calcium → used to prevent calcium oxalate kidney stones.
Clinical link - Gitelman syndrome (loss-of-function NCC mutation): hypokalemia, hypomagnesaemia, metabolic alkalosis, hypocalciuria - phenotype mirrors thiazide use.
D. Collecting Duct
- Principal cells: Na⁺ reabsorption via ENaC channels; K⁺ secretion; regulated by aldosterone
- Intercalated cells (α): H⁺ secretion (vacuolar H⁺-ATPase) → urine acidification
- Water permeability controlled by ADH (vasopressin) via aquaporin-2 insertion
Clinical link - Aldosterone antagonists (spironolactone, eplerenone): Block ENaC activation → K⁺-sparing diuresis. Used in: heart failure, primary hyperaldosteronism (Conn's syndrome), resistant hypertension.
Clinical link - Diabetes Insipidus (DI):
- Central DI: ↓ ADH secretion → dilute polyuria → treat with desmopressin (synthetic ADH)
- Nephrogenic DI: Collecting duct resistant to ADH (mutation in V2 receptor or aquaporin-2) → treat with low-sodium diet + thiazides ± NSAIDs
Clinical link - SIADH: Excess ADH → concentrated urine + dilutional hyponatraemia. Causes: lung cancer, CNS injury, hypothyroidism. Treat: fluid restriction; vaptans (tolvaptan) block V2 receptor.
7. Renin-Angiotensin-Aldosterone System (RAAS)
The RAAS is the kidney's master regulator of blood pressure and Na⁺ balance:
- ↓ Renal perfusion pressure → Juxtaglomerular (granular) cells release renin
- Renin cleaves angiotensinogen → Angiotensin I
- ACE (lung) converts Ang I → Angiotensin II
- Ang II → vasoconstriction of efferent arteriole (maintains GFR) + ↑ aldosterone + ↑ ADH + thirst
- Aldosterone → ↑ ENaC and Na⁺/K⁺-ATPase in collecting duct → Na⁺ retention + K⁺ excretion
Clinical case (Costanzo Physiology): A 65-year-old woman with 90% stenosis of the right renal artery presents with hypertension (diastolic 115 mmHg), decreased GFR (30 mL/min), elevated plasma renin (higher in right renal vein), and abdominal bruits from turbulent flow. The stenosed right kidney interprets low perfusion as low BP → hyperactivates RAAS → Ang II vasoconstriction + aldosterone Na⁺ retention → severe hypertension. Treatment: ACEi (captopril) blocks conversion of Ang I to Ang II, interrupting the cycle.
8. Urine Concentration and Dilution
The kidney can produce urine from 30 mOsm/kg (maximal dilution) to 1400 mOsm/kg (maximal concentration). This is achieved via the countercurrent multiplier (loop of Henle) and countercurrent exchanger (vasa recta):
| Condition | ADH Level | Urine Osmolality | Mechanism |
|---|---|---|---|
| Overhydrated | Low/absent | 30-100 mOsm/kg | AQP-2 absent → water stays in tubule |
| Euhydrated | Moderate | ~300 mOsm/kg | Balanced reabsorption |
| Dehydrated | High | 800-1400 mOsm/kg | AQP-2 inserted → water reabsorbed |
The vasa recta preserve the medullary gradient through countercurrent exchange - descending vessels lose water and gain solute; ascending vessels do the reverse.
9. Renal Acid-Base Regulation
The kidney is the primary organ for non-volatile acid excretion and HCO₃⁻ regulation:
| Process | Location | Mechanism |
|---|---|---|
| HCO₃⁻ reabsorption | PCT (80-85%) | NHE3: H⁺ secreted, binds filtered HCO₃⁻ to form H₂CO₃ → CO₂ + H₂O |
| HCO₃⁻ reabsorption | TAL, DCT | Similar mechanism |
| Titratable acid excretion | Collecting duct | H⁺ buffered by HPO₄²⁻ → H₂PO₄⁻ |
| NH₄⁺ excretion | PCT, collecting duct | Glutamine → NH₃ + H⁺ → NH₄⁺ in urine |
Clinical link - Renal Tubular Acidosis (RTA):
- Type 1 (distal RTA): Defective H⁺-ATPase in α-intercalated cells → cannot acidify urine below pH 5.5 → hyperchloraemic metabolic acidosis + hypokalaemia + kidney stones (nephrocalcinosis). Causes: Sjögren's, amphotericin B.
- Type 2 (proximal RTA): Defective HCO₃⁻ reabsorption in PCT → HCO₃⁻ wasted in urine → acidosis. Part of Fanconi syndrome.
- Type 4 RTA: Hypoaldosteronism (e.g. diabetic nephropathy) → hyperkalemia + metabolic acidosis.
10. Summary: Clinical Applications by Segment
| Segment | Key Transporter | Diuretic/Drug | Clinical Condition |
|---|---|---|---|
| PCT | SGLT2, NHE3, carbonic anhydrase | SGLT2 inhibitors, acetazolamide | Diabetic nephropathy, glaucoma, altitude sickness |
| Loop of Henle (TAL) | NKCC2 | Loop diuretics (furosemide) | Heart failure, pulmonary oedema, hypercalcaemia |
| DCT | NCC | Thiazides | Hypertension, hypercalciuria, Gitelman syndrome |
| Collecting duct | ENaC, AQP-2 | Aldosterone antagonists, vaptans | Heart failure, Conn's, SIADH, DI |
| Glomerulus | Filtration barrier | ACEi, ARBs | Nephrotic syndrome, diabetic nephropathy |
Sources: Ganong's Review of Medical Physiology (26th ed.) | Guyton & Hall Textbook of Medical Physiology (14th ed.) | Costanzo Physiology (7th ed.) | Goodman & Gilman's Pharmacological Basis of Therapeutics | Campbell-Walsh Urology
This is a shared conversation. Sign in to Orris to start your own chat.