What is tela choridae
Reading File
Finding Sources
Searching the Web
tela choroidea anatomy brain ventricular system
Reading File
Reading File
Reading File
Here is a thorough explanation of the tela choroidea, drawn from authoritative medical textbooks:
Tela Choroidea
Definition
The tela choroidea is a two-layered vascular fold formed by the union of the pia mater (the innermost meningeal layer) with the ependymal lining (the epithelial lining of the ventricular system). The name comes from Latin: tela = web/tissue, choroidea = choroid-like (referring to its resemblance to the choroid of the eye).
- Medical Physiology (Boron & Boulpaep): "The tela choroidea consists of a layer of ependymal cells covered by the pia mater and its associated blood vessels."
- Langman's Medical Embryology: "The roof plate...consists of a single layer of ependymal cells covered by vascular mesenchyme, the pia mater. The two combined are known as the tela choroidea."
Composition
The tela choroidea has two layers:
- Ependymal layer - the inner epithelial cells lining the ventricle
- Pia mater layer - the vascular connective tissue membrane derived from mesenchyme, carrying blood vessels
Locations in the Brain
The tela choroidea is found associated with the roof or wall of each ventricle:
| Ventricle | Location of Tela Choroidea |
|---|---|
| Lateral ventricles | Along the medial walls |
| Third ventricle | Double fold in the roof (a double layer of vascular pia mater) |
| Fourth ventricle | Covers the thin ependymal roof; forms the sheet of pia over the lower part of the fourth ventricle |
Function - Formation of the Choroid Plexus
The primary role of the tela choroidea is to give rise to the choroid plexus, which is the source of cerebrospinal fluid (CSF).
During embryological development:
- The pia mater proliferates actively
- It invaginates through the ependymal roof into the ventricular cavity
- Saclike, tuft-like projections (called the choroid plexus) form inside the ventricle
- These choroid plexus tufts secrete CSF
As stated in The Developing Human (Moore): "Because of the active proliferation of the pia, the tela choroidea invaginates the fourth ventricle, where it differentiates into the choroid plexus, infoldings of choroidal arteries of the pia."
Each of the four choroid plexuses (two in the lateral ventricles, one in the third, one in the fourth) is formed by this process.
CSF Production
The choroid epithelial cells derived from the tela choroidea secrete CSF into the ventricles. This CSF then:
- Flows through the ventricular system (lateral --> third --> fourth ventricles via the cerebral aqueduct)
- Exits the fourth ventricle through the foramen of Magendie (median aperture) and foramina of Luschka (lateral apertures)
- Enters the subarachnoid space
- Is absorbed into the venous system via arachnoid villi projecting into the dural venous sinuses
Clinical Relevance
- Colloid cysts arise from the infolding neuroepithelium of the tela choroidea and are located almost exclusively in the anterior third of the third ventricle at the level of the foramen of Monro (per Bradley and Daroff's Neurology in Clinical Practice).
- Tumors such as choroid plexus papillomas originate from the epithelium derived from the tela choroidea.
- The tela choroidea is also a site of NF2 (neurofibromatosis type 2) gene promoter expression, as the ependymal cells of the tela choroidea contain NF2-expressing cells.
Summary
| Feature | Detail |
|---|---|
| Structure | Fold of pia mater + ependymal epithelium |
| Location | Roof/walls of all four ventricles |
| Key function | Forms the choroid plexus |
| Product | CSF (via choroid plexus secretion) |
| Clinical significance | Origin of colloid cysts, choroid plexus tumors |
In short, the tela choroidea is the structural "raw material" - the vascular meningeal sheet - from which the choroid plexus develops and through which CSF production is made possible.
What are the roof of 4th ventricle
Finding Sources
Finding Sources
Finding Sources
Searching the Web
roof of fourth ventricle anatomy superior inferior medullary velum tela choroidea apertures
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Now I have comprehensive information. Let me compile the complete answer.
Roof of the 4th Ventricle
The roof (posterior wall) of the 4th ventricle is tent-shaped and formed by several distinct structures. It can be divided into an upper (superior/cranial) part and a lower (inferior/caudal) part.
Overall Shape
The roof is tent-like, with its apex pointing posteriorly toward the cerebellum. The tip (highest point) of this tent is called the fastigium.
Components of the Roof
1. Superior (Upper) Part
Superior Medullary Velum (Velum Medullare Superius)
- A thin sheet of white matter (myelinated nerve fibers) stretching between the two superior cerebellar peduncles
- Bridges the gap between the pons and the cerebellum in the upper portion
- The trochlear nerve (CN IV) - the only cranial nerve to emerge from the dorsal surface of the brainstem - decussates within and then exits from the superior medullary velum
- Clinically: infiltration by medulloblastoma can cause bilateral CN IV palsies
2. Posterior/Middle Part
The Cerebellum
- The anterior (inferior) surface of the cerebellum - specifically its vermis - forms the posterior roof
- The lingula of the cerebellar vermis is attached to the superior medullary velum
- The nodule of the vermis is attached inferiorly to the inferior medullary velum
- Localization in Clinical Neurology: "the cerebellum forms the roof of the fourth ventricle"
3. Inferior (Lower) Part
Inferior Medullary Velum (Velum Medullare Inferius)
- A thin, paired (bilateral) crescentic sheet of white matter
- Attached to the nodule of the cerebellar vermis above and to the tela choroidea below
- Much thinner than the superior velum; some sources describe it as partly membranous
Tela Choroidea of the 4th Ventricle
- A fold of pia mater fused with the ependymal lining
- Forms the roof of the lower (caudal) half of the 4th ventricle
- Contains the choroid plexus of the 4th ventricle, which hangs into the ventricular cavity
- The choroid plexus here is supplied by branches of PICA (posterior inferior cerebellar artery), AICA, and SCA (Grainger & Allison's)
Apertures (Openings) in the Roof
The lower part of the roof contains three critical openings through which CSF exits the ventricular system into the subarachnoid space:
| Aperture | Location | Details |
|---|---|---|
| Foramen of Magendie (median aperture) | Midline, in the inferior roof | Single midline opening; CSF flows into the cisterna magna |
| Foramina of Luschka (lateral apertures) | Bilateral, at the lateral recesses | Two openings at the tips of the lateral recesses; tufts of choroid plexus often project through these into the subarachnoid space |
As described in Grainger & Allison's Diagnostic Radiology: "The lateral recesses funnel into the foramina of Luschka. Tufts of choroid plexus typically project through the foramina of Luschka into the subarachnoid space."
Summary Table
| Part of Roof | Structure | Notes |
|---|---|---|
| Upper | Superior medullary velum | White matter bridge between superior cerebellar peduncles; CN IV decussates here |
| Middle/Posterior | Cerebellar vermis (inferior surface) | Nodule attaches to inferior velum |
| Lower | Inferior medullary velum | Thin white matter sheet; paired |
| Lower | Tela choroidea | Pia + ependyma; gives rise to choroid plexus |
| Openings | Foramen of Magendie (x1) + Foramina of Luschka (x2) | CSF exits to subarachnoid space |
Clinical Relevance
- Medulloblastoma: arises from undifferentiated neuroectodermal cells of the roof (superior or inferior medullary velum and vermis); most common brain tumor in children (Bradley & Daroff's Neurology)
- Dandy-Walker malformation: ballooning of the posterior half of the 4th ventricle, often with non-patency of the foramen of Magendie, aplastic posterior vermis, and hydrocephalus
- Blake pouch cyst: derived from the posterior membranous area of the roof; normally communicates with subarachnoid space by 26 weeks gestation
- CN IV palsy: lesions of the superior medullary velum (tumor, trauma, demyelination) cause trochlear nerve injury since it decussates there
Image
Asking for Preferences
Image for roof of 4th ventricle
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
Here are the textbook images of the 4th ventricle roof from Grainger & Allison's Diagnostic Radiology:
Image 1 - MRI of Cerebellum (Sagittal & Axial)
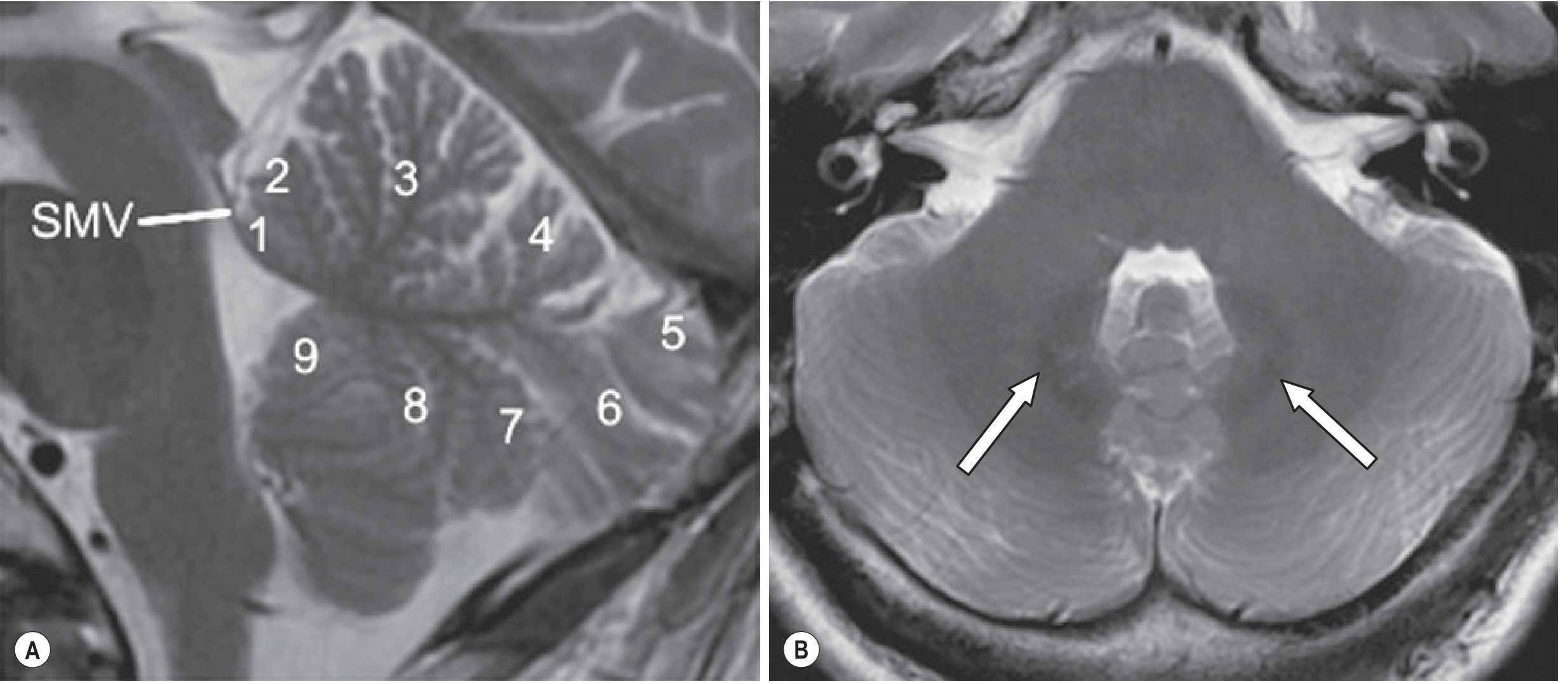
Fig. A (Sagittal MRI) - Shows the roof of the 4th ventricle formed by the Superior Medullary Velum (SMV) labeled with an arrow. The cerebellar vermis lobules are numbered:
- 1 = Lingula (attached to SMV)
- 2 = Central lobule
- 3 = Culmen
- 4 = Declive
- 5 = Folium
- 6 = Tuber
- 7 = Pyramid
- 8 = Uvula
- 9 = Nodule (attached to inferior medullary velum)
Fig. B (Axial MRI) - Axial view at the level of the pons; arrows indicate iron deposition in dentate nuclei.
Image 2 - MRI & CT showing Ventricular Apertures
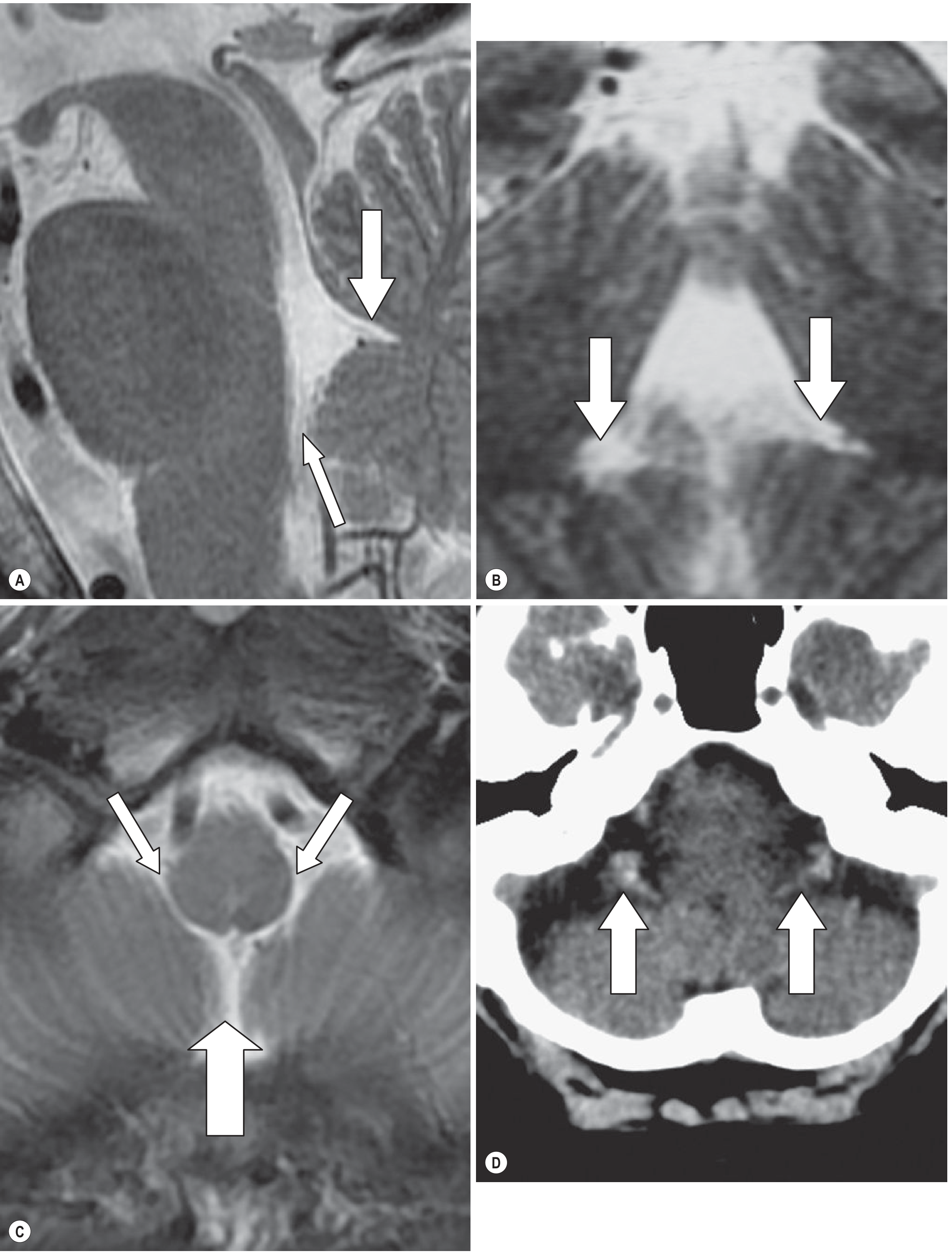
Fig. A (Sagittal MRI) - Large arrow = Fastigium (the tented apex/peak of the 4th ventricle roof formed by cerebellar vermis); Small arrow = Foramen of Magendie (median aperture for CSF to exit)
Fig. B (Coronal MRI) - Arrows show the rhomboid shape of the 4th ventricle; lateral recesses are visible funneling toward the foramina of Luschka
Fig. C (Axial MRI) - Two angled arrows = bilateral Foramina of Luschka (lateral apertures); Large upward arrow = Foramen of Magendie (midline aperture)
Fig. D (Axial CT) - Arrows show calcified choroid plexus tufts projecting through the foramina of Luschka into the subarachnoid space - a normal variant
Key Structures of the Roof (summarized from images)
| Structure | What you see on MRI |
|---|---|
| Superior Medullary Velum (SMV) | Thin white matter band at the upper roof (labeled in Fig. 1A) |
| Fastigium | Tent-like apex of the roof pointing into the cerebellum (Fig. 2A, large arrow) |
| Nodule of vermis | Lowest cerebellar lobule (labeled "9" in Fig. 1A), attached to inferior velum |
| Foramen of Magendie | Midline opening at inferior roof (Fig. 2A small arrow; Fig. 2C large arrow) |
| Foramina of Luschka | Bilateral lateral openings (Fig. 2C angled arrows; Fig. 2D arrows with calcified choroid) |
What is spinal tract
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Excellent - I now have comprehensive textbook content. Here is the complete answer with the diagram:
Spinal Tracts
Spinal tracts are organized bundles of nerve fibers (axons) running through the white matter of the spinal cord. They serve as communication highways between the body and the brain. Each tract is named after its origin and destination (e.g., spinothalamic = spinal cord to thalamus; corticospinal = cortex to spinal cord).
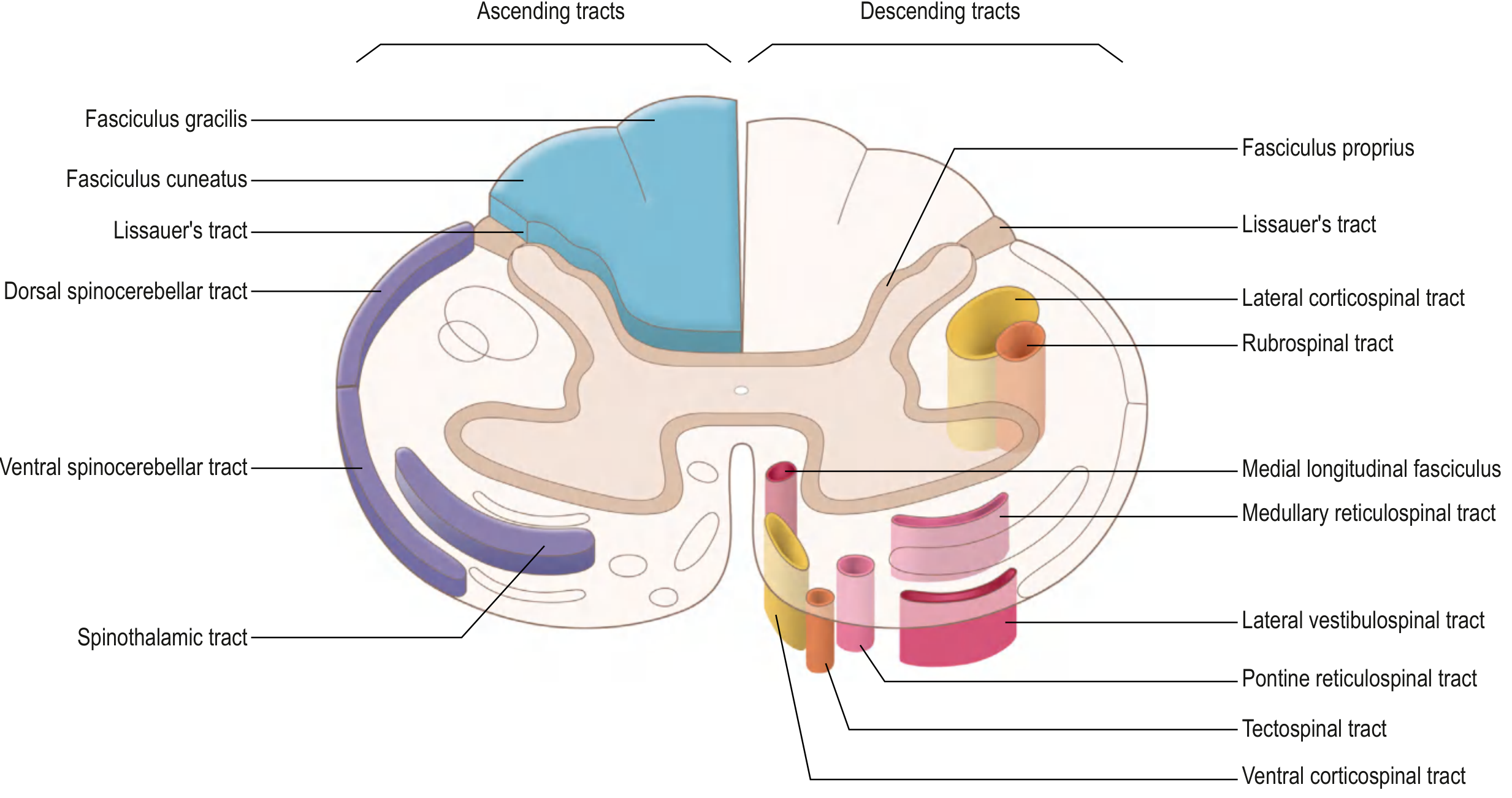
Gray's Anatomy for Students - eFig. 9.42: Ascending tracts shown on the left (blue/purple), descending tracts on the right (yellow/pink/orange). All tracts are present bilaterally.
Classification
Spinal tracts are divided into two major groups:
A. ASCENDING TRACTS (Sensory - carry signals UP to brain)
These carry sensory information from peripheral receptors to conscious or subconscious brain centers through a 3-neuron chain.
1. Anterolateral Pathways (pain, temperature, crude touch)
These are composed of 3 tracts:
| Tract | Sensation Carried | Destination |
|---|---|---|
| Spinothalamic tract | Pain, temperature, crude touch | Ventral posterolateral (VPL) nucleus of thalamus → somatosensory cortex |
| Spinoreticular tract | Emotional/arousal aspects of pain | Reticular formation of brainstem |
| Spinomesencephalic tract | Pain modulation | Periaqueductal gray matter + superior colliculi (midbrain) |
Course of the spinothalamic tract:
- 1st neuron: cell body in spinal (dorsal root) ganglion → enters posterior horn
- Axon collaterals ascend/descend 1-2 segments in Lissauer's tract before synapsing
- 2nd neuron: crosses obliquely over 2-3 segments via the anterior commissure to the contralateral anterolateral column → ascends to the thalamus
- 3rd neuron: thalamus → primary somatosensory cortex via posterior limb of internal capsule
2. Posterior Column - Medial Lemniscal Pathway (fine touch, vibration, proprioception)
| Fasciculus | Carries Information From | Position |
|---|---|---|
| Fasciculus gracilis | Lower limbs and trunk (below T6) | Medial posterior column |
| Fasciculus cuneatus | Upper limbs and neck (above T6) | Lateral posterior column |
Course:
- 1st neuron: spinal ganglion → enters posterior root → ascends ipsilaterally to caudal medulla
- Synapses at nucleus gracilis / nucleus cuneatus (caudal medulla)
- 2nd neuron: axons cross midline as internal arcuate fibers → form the medial lemniscus → ascend to VPL thalamus
- 3rd neuron: thalamus → somatosensory cortex
3. Spinocerebellar Tracts (subconscious proprioception to cerebellum)
| Tract | Function | Crossing |
|---|---|---|
| Dorsal spinocerebellar tract | Subconscious proprioception from lower limbs | Ipsilateral (uncrossed) |
| Ventral spinocerebellar tract | Subconscious proprioception from lower limbs | Double crossed (crosses twice - ends up ipsilateral) |
B. DESCENDING TRACTS (Motor - carry signals DOWN from brain)
Descending tracts control voluntary movement, posture, balance, and head/neck orientation. Each tract has an upper motor neuron (UMN) in the cortex/brainstem and a lower motor neuron (LMN) in the spinal cord.
1. Lateral Motor System (controls limb movements)
| Tract | Origin | Function | Location in cord |
|---|---|---|---|
| Lateral corticospinal tract | Primary motor cortex | Voluntary movements of upper & lower extremities | Lateral column |
| Rubrospinal tract | Red nucleus (midbrain) | Flexor activity of upper limb; inhibits extensors | Lateral column |
Lateral corticospinal tract course (most important motor tract):
- Cell bodies in primary motor cortex → corona radiata → posterior limb of internal capsule → crus cerebri (midbrain) → through pons → forms the pyramid in medulla
- At caudal medulla: ~90% of fibers decussate (pyramidal decussation) → form lateral corticospinal tract in contralateral lateral column
- Remaining ~10% stay ipsilateral → form anterior corticospinal tract
- Synapse on LMN cell bodies in the lateral anterior horn
2. Medial Motor System (controls axial/postural muscles)
| Tract | Origin | Function | Extent |
|---|---|---|---|
| Anterior corticospinal tract | Motor cortex (uncrossed fibers) | Axial/trunk muscles; postural control | Upper thoracic |
| Tectospinal tract | Superior colliculus (midbrain) | Reflex postural movements to visual stimuli | Cervical only |
| Vestibulospinal tract | Vestibular nuclei (pons/medulla) | Maintains balance; facilitates extensors, inhibits flexors | Entire cord length |
| Reticulospinal tract (medullary + pontine) | Reticular formation | Muscle tone, autonomic function, breathing | Entire cord |
| Medial longitudinal fasciculus (MLF) | Multiple brainstem nuclei | Coordinates eye/head/neck movements | Cervical |
Key Clinical Points
| Lesion | Result |
|---|---|
| Spinothalamic tract lesion | Contralateral loss of pain and temperature (below the level of injury, since it crosses early) |
| Posterior column lesion | Ipsilateral loss of fine touch, vibration, proprioception (crosses in medulla, not spinal cord) |
| Lateral corticospinal tract lesion | Contralateral spastic paralysis (UMN signs: hyperreflexia, spasticity, upgoing plantar) |
| Brown-Séquard syndrome (hemisection) | Ipsilateral motor loss + proprioception loss + contralateral pain/temperature loss |
| Complete cord transection | All ascending and descending tracts below the lesion are interrupted - complete loss of motor and sensory function below |
- Gray's Anatomy for Students, pp. e30-e32
No I mean at the in transverse section of Pyrimidal decussation medulla
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Here are the exact myelin-stained transverse sections from Neuroanatomy through Clinical Cases showing the pyramidal decussation level and surrounding sections for comparison:
Transverse Section at the Level of Pyramidal Decussation
Fig. C - Cervicomedullary Junction (THE Pyramidal Decussation Level)
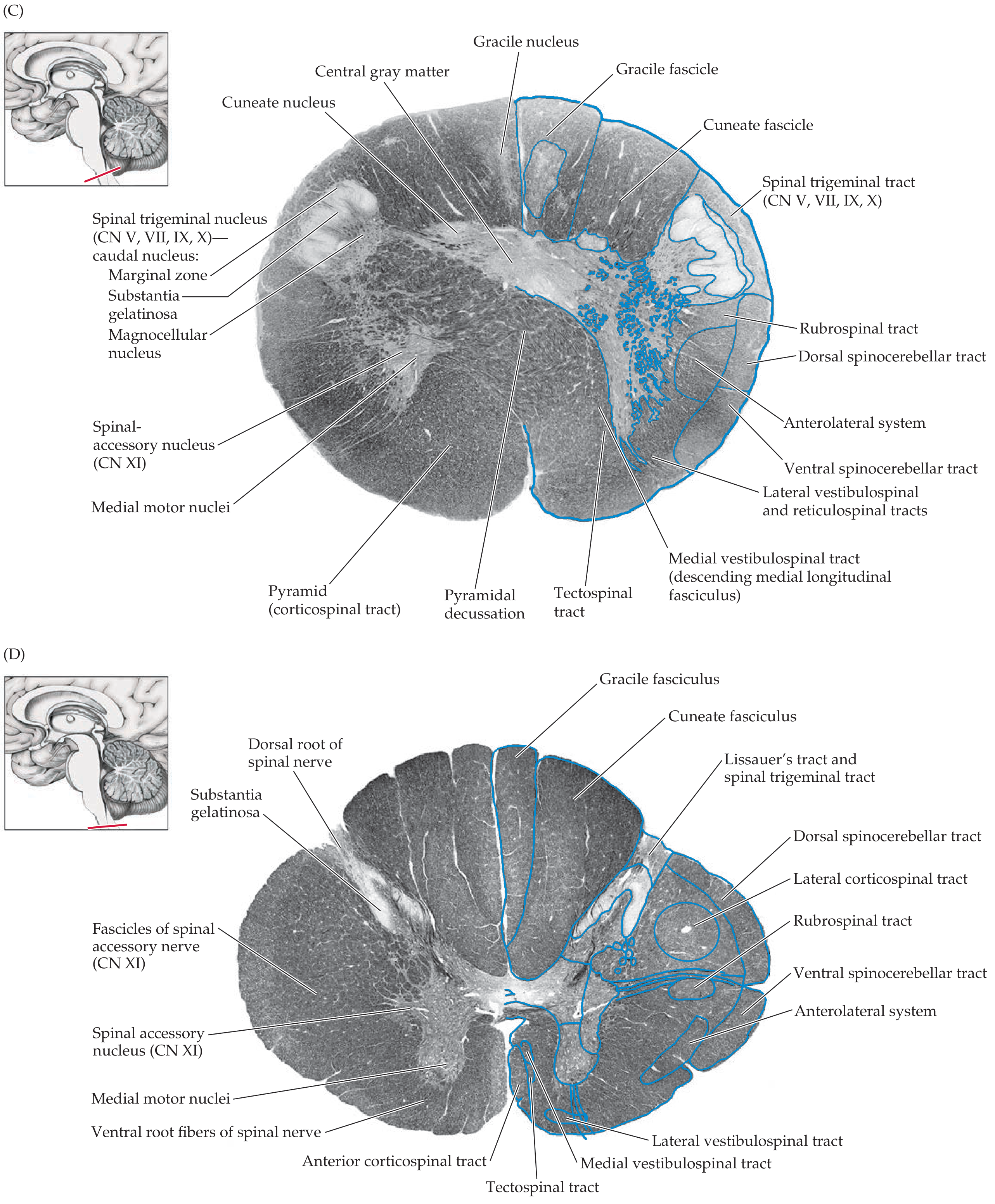
This is the key section. The pyramidal decussation is labeled directly in the ventral midline. Here is what you see in each region:
DORSAL (Posterior) Region:
| Structure | Position | Significance |
|---|---|---|
| Gracile fascicle | Dorsal midline | Fine touch/vibration from lower limbs ascending ipsilaterally |
| Cuneate fascicle | Dorsolateral | Fine touch/vibration from upper limbs ascending ipsilaterally |
| Gracile nucleus | Dorsomedial gray | Relay station - 2nd neuron of posterior column pathway |
| Cuneate nucleus | Dorsolateral gray | Relay station - 2nd neuron of posterior column pathway |
| Central gray matter | Around central canal | Central gray matter (transitioning from 4th ventricle above) |
LATERAL Region:
| Structure | Position | Significance |
|---|---|---|
| Spinal trigeminal tract | Lateral white matter | Pain/temp from face (CN V, VII, IX, X) - caudal nucleus here |
| Spinal trigeminal nucleus (caudal - 3 sub-zones: marginal zone, substantia gelatinosa, magnocellular) | Lateral gray | Relay for facial pain/temperature |
| Rubrospinal tract | Lateral column | Flexor control of upper limb |
| Dorsal spinocerebellar tract | Posterolateral | Subconscious proprioception to cerebellum |
| Anterolateral system | Lateral | Pain & temperature from body (spinothalamic) |
| Ventral spinocerebellar tract | Anterolateral | Subconscious proprioception to cerebellum |
| Lateral vestibulospinal + reticulospinal tracts | Anterolateral | Postural/balance control |
VENTRAL (Anterior) Region:
| Structure | Position | Significance |
|---|---|---|
| Pyramidal decussation | Ventral MIDLINE | ⚡ The key landmark - corticospinal fibers crossing from one side to the other |
| Pyramid (corticospinal tract) | Ventral, bilateral | Before/after crossing - the bundle of UMN axons |
| Tectospinal tract | Near ventral midline | Head/neck reflex movements |
| Medial vestibulospinal tract (= descending MLF) | Ventromedial | Gaze/head coordination |
| Spinal-accessory nucleus (CN XI) | Lateral anterior horn | Motor nucleus of CN XI (only here, NOT in medulla proper) |
| Medial motor nuclei | Medial anterior horn | Axial muscle control |
For Comparison - Fig. B (Caudal Medulla, just above decussation):
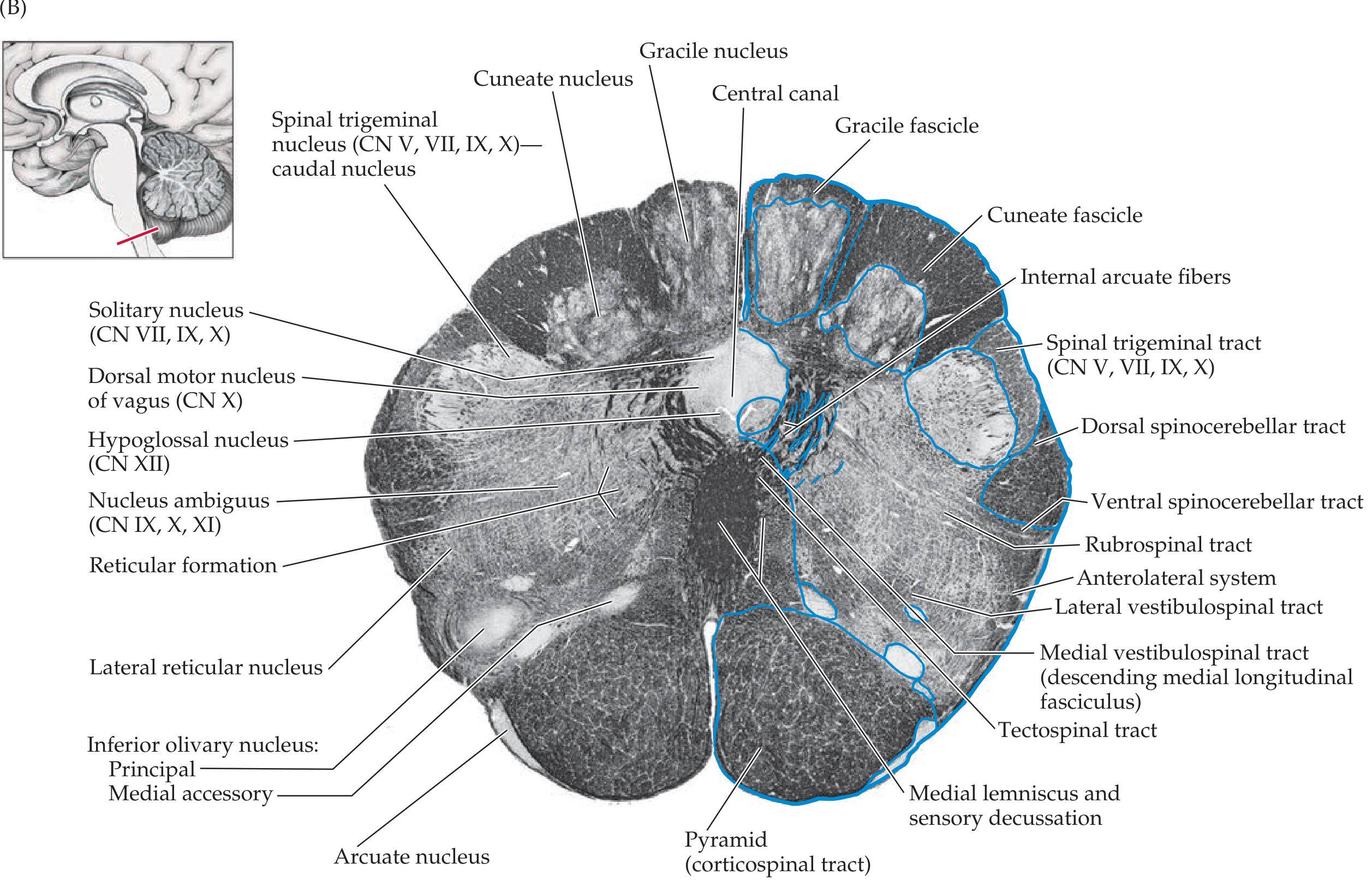
At caudal medulla (just above the decussation):
- Pyramid is intact ventrally (not yet decussating)
- Medial lemniscus and sensory decussation (internal arcuate fibers) visible near the midline - this is where the posterior column 2nd neurons cross
- Inferior olivary nucleus (principal + medial accessory) large folded structure ventrally - disappears at decussation level
- Hypoglossal nucleus (CN XII) dorsomedially
- Nucleus ambiguus (CN IX, X, XI) in lateral tegmentum
- Solitary nucleus/tract (CN VII, IX, X) dorsolaterally
Key Difference: Pyramidal Decussation vs. Caudal Medulla
| Feature | Caudal Medulla (B) | Pyramidal Decussation (C) |
|---|---|---|
| Inferior olivary nucleus | Present | Absent |
| 4th ventricle | Small/absent | Absent - central canal instead |
| Pyramid | Intact, ventral | Crossing midline (decussation visible) |
| Internal arcuate fibers | Visible (sensory decussation) | Replaced by posterior column nuclei |
| Spinal accessory nucleus | Absent | Present |
| Substantia gelatinosa (spinal V) | Present | Present (caudal nucleus) |
- Neuroanatomy through Clinical Cases (3rd Ed.), Fig. 14.5 (A-D)
This is a shared conversation. Sign in to Orris to start your own chat.