Fibular head fracture with CPN palsy. Management protocol. For 10 marks to write in MS final exam
Reading File
Finding Sources
Finding Sources
Searching PubMed
"common peroneal nerve" AND "fibular head" AND fracture
Reading File
Reading File
Reading File
Searching PubMed
"peroneal nerve palsy" AND management AND decompression
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the full exam-grade answer.
Fibular Head Fracture with Common Peroneal Nerve (CPN) Palsy - Management Protocol
(10-mark MS Final Exam Answer)
Anatomy Recap (Why it Matters)
The Common Peroneal Nerve (CPN) - also called the Common Fibular Nerve - is a branch of the sciatic nerve (L4, L5, S1, S2). After separating from the sciatic nerve in the popliteal fossa, it winds around the posterior aspect of the fibular head, encircles the fibular neck, and divides into:
- Superficial peroneal nerve - supplies peroneus longus & brevis (eversion), and sensation over anterolateral leg and dorsum of foot
- Deep peroneal nerve - supplies tibialis anterior, EHL, EDL, EDB (dorsiflexion and toe extension), and sensation to the 1st web space
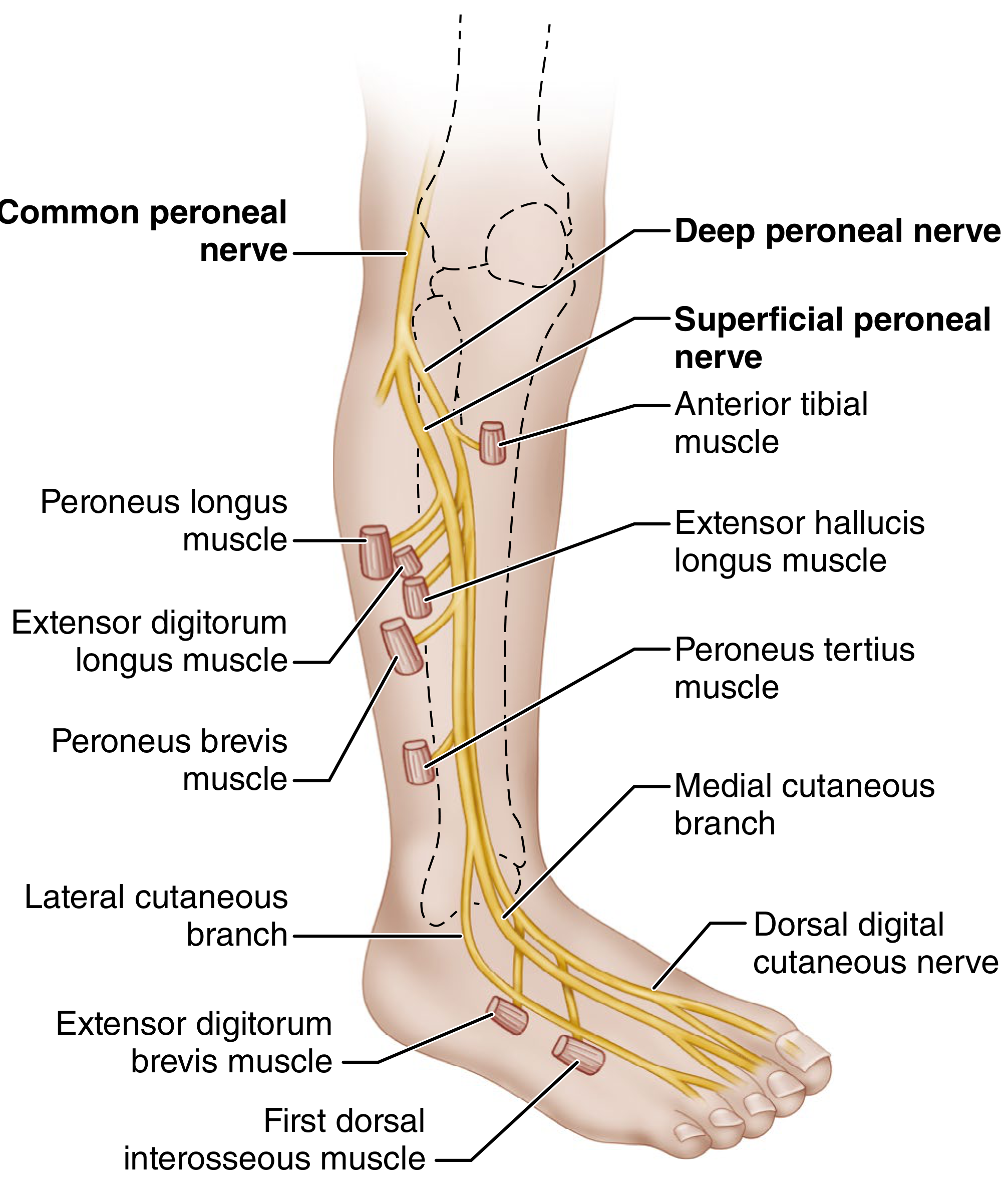
The nerve is superficial and tethered between the biceps femoris tendon proximally and the peroneus longus fibrous arch distally - making it extremely vulnerable at the fibular neck to traction, compression, and direct injury from fractures of the fibular head/neck.
1. Classification of Nerve Injury (Sunderland/Seddon)
| Grade | Seddon | Pathology | Expected Recovery |
|---|---|---|---|
| 1st degree | Neuropraxia | Focal demyelination, axon intact | Full, weeks to months |
| 2nd degree | Axonotmesis | Axon disrupted, endoneurium intact | Good, Wallerian degeneration |
| 3rd-5th degree | Neurotmesis | Complete disruption | Poor without surgery |
- In closed fibular head fractures: most injuries are neuropraxia or axonotmesis (neurapraxia heals automatically; axonotmesis has good prognosis)
- Neurotmesis is rare with closed fractures
2. Clinical Features of CPN Palsy
Motor deficit:
- Foot drop (loss of ankle dorsiflexion)
- Loss of toe extension
- Loss of foot eversion (peroneus longus and brevis)
- High-stepping gait
Sensory deficit:
- Dorsum of foot and toes
- Anterolateral distal leg
- First web space (deep peroneal territory)
No pain is typical. Inversion and ankle plantar flexion (tibial nerve) are preserved.
Key differentials to exclude: L5 radiculopathy (ankle invertors also weak, EMG shows denervation in paraspinals), sciatic nerve injury, lumbosacral plexopathy.
3. Investigations
A. Electrophysiology (EDx) - mandatory
- Done at 72 hours to 3 weeks post-injury
- Nerve Conduction Studies (NCS): Peroneal motor conduction velocity shows slowing and amplitude drop across the fibular head - this localizes the lesion
- EMG (needle): Fibrillation potentials, positive sharp waves in tibialis anterior, EHL, peronei indicate axonotmesis. Absent activity = complete lesion
- Prognostic value: If CMAPs (compound muscle action potentials) are preserved, prognosis is good (neuropraxia)
B. Imaging
- X-ray knee (AP, lateral): For fibular head/neck fracture - characterize displacement, associated tibial plateau or knee injury
- MRI knee: For associated ligamentous injury, multiligamentous knee injury (which raises CPN palsy risk to 45%), intraneural ganglia
- Ultrasound of CPN: To identify compressive hematoma, neuroma, entrapment
4. Management Protocol
STEP 1: Initial Assessment and Fracture Management
Rule out limb-threatening injuries first:
- Vascular assessment (popliteal artery - ABI, doppler) - especially in knee dislocations/complex fractures
- Compartment syndrome assessment
The fibular head fracture itself:
- Isolated fibular head fractures without significant displacement and without associated ligamentous disruption: conservative management (short leg brace/cast, protected weight bearing)
- Surgical exploration of the fracture site carries risk of additional damage to the CPN and is not indicated solely for the fracture unless associated with knee dislocation / multiligamentous injury requiring operative repair (Rockwood & Green, 10th Ed 2025)
STEP 2: Immediate Conservative Management (for Neuropraxia/Mild Axonotmesis)
All patients initially:
- Ankle-foot orthosis (AFO) - "ankle brace": Prevents equinus deformity and foot drop complications. Applied immediately.
- Physiotherapy:
- Passive range-of-motion of ankle and foot (prevent contractures)
- Active exercises for preserved muscles
- Electrical stimulation of denervated muscles
- Padding/protection: Knee pad over lateral knee to prevent further compression. Remove offending compressive elements (tight casts, bandages, cross-leg positioning).
- Patient education: Avoid leg crossing, prolonged kneeling, pressure on lateral knee.
- Observation: Most cases of neuropraxia spontaneously resolve over weeks to months (Harrison's Principles of Internal Medicine, 22nd Ed 2025)
Decision point at 6-8 weeks: Repeat clinical + EMG assessment
STEP 3: Decision for Surgical Intervention
Based on the Samson et al. evidence-based algorithm (Campbell's Operative Orthopaedics, 15th Ed 2026), management hinges on:
A. Complete vs. Incomplete Palsy (clinical + EMG)
| Finding | Action |
|---|---|
| Incomplete palsy (partial motor/sensory) | Conservative x 3-6 months, serial EMG |
| Complete palsy + intact NCS amplitudes | Likely neuropraxia - conservative |
| Complete palsy + absent CMAP | Likely neurotmesis - surgical exploration |
| No improvement at 3-6 months + abnormal EMG | Surgical exploration |
| Open fracture with suspected nerve laceration | Early surgical exploration |
B. Indications for Surgical Exploration
- Open fracture with visible nerve damage
- No clinical or electrophysiological recovery at 3-4 months
- Suspected nerve laceration on imaging
- Progressively worsening deficit
- Compressive lesion (hematoma, callus, intraneural ganglion) on imaging
STEP 4: Surgical Technique - Neurolysis / Nerve Repair
Approach (Campbell's, 15th Ed 2026):
- Begin incision proximal to injury (medial to biceps tendon)
- At fibular head - curve anteriorly over neck of fibula and distally along anterolateral leg
- Identify nerve on medial side of biceps tendon; trace distally as it curves around neck of fibula between peroneus longus origin and bone
- At fibular neck: nerve divides into superficial and deep branches
Options:
- External neurolysis: Release of compressing fibrotic tissue, hematoma, callus - most common; relieves symptoms in majority of entrapment/compression cases
- Internal neurolysis (intraneural): For intraneural fibrosis
- End-to-end neurorrhaphy: For clean lacerations with small gap; requires tension-free repair
- Nerve grafting: For gaps >2-3 cm; autogenous interfascicular grafting is preferred (sural nerve from contralateral leg preferred if ipsilateral sensory function is intact)
- Flexing the knee allows closure of gaps up to 10-12 cm in the popliteal fossa
- Postoperative immobilization: Hip spica cast x 6 weeks (not just long leg cast - suture lines tend to separate due to tension between fibula and pelvis), then gradual knee extension over next 6 weeks
Prognosis after nerve repair:
- Under most favorable circumstances (low lesion, small gap, early repair): 60-70% achieve useful motor recovery (foot dorsiflexion against gravity)
- Nerve suture useful if performed before 12-15 months post-injury
- 87% of patients with partial palsy achieve full motor recovery vs. only 38% with complete lesions (Campbell's, citing systematic review)
STEP 5: Management of Persistent Foot Drop (Late/Failed Cases)
If foot drop persists for >1 year and nerve recovery is not anticipated:
- Tendon transfer - Posterior tibial tendon transfer (PTT transfer): Transfers tibialis posterior tendon through the interosseous membrane to the dorsum of the foot - provides active dorsiflexion; recommended after 1 year of confirmed persistent foot drop
- Peroneal nerve grafting as a salvage procedure
- AFO long-term if patient is not a surgical candidate
- Ankle arthrodesis - last resort for flail ankle
5. Summary Algorithm
Fibular Head Fracture + CPN Palsy
|
Immediate: X-ray, vascular assessment, AFO
|
Open fracture?
YES -------> Explore + repair nerve early
NO
|
EMG at 3-6 weeks
|
Incomplete / Neuropraxia --> Conservative (AFO, physio, serial EMG)
| |
Complete / no recovery 3-6 mo Resolved (most cases) --> DISCHARGE
|
MRI/USG - compressive lesion?
YES --> Decompress (neurolysis)
NO --> Nerve exploration + repair/grafting
|
Foot drop > 1 year, no recovery
|
Posterior tibial tendon transfer
6. Key Points for Exam
- CPN is the most commonly injured peripheral nerve in lower limb trauma - Campbell's Operative Orthopaedics
- In closed fibular head fractures, the lesion is usually neuropraxia - heals spontaneously
- The fibular head fracture itself does not require fixation; exploration at this level risks further CPN damage
- EMG at 3-6 weeks is the cornerstone for prognostication
- AFO (ankle foot orthosis) is applied immediately in all patients
- Nerve repair results: 60-70% achieve useful dorsiflexion after favorable repair
- Posterior tibial tendon transfer for persistent foot drop >1 year
References:
- Campbell's Operative Orthopaedics, 15th Ed 2026 - Sections on Common Peroneal Nerve and Knee Dislocation
- Rockwood and Green's Fractures in Adults, 10th Ed 2025
- Harrison's Principles of Internal Medicine, 22nd Ed 2025
- Localization in Clinical Neurology, 8th Ed
- S. Das - A Manual on Clinical Surgery, 13th Ed
- Chow AL et al. "Clinical Outcomes After Neurolysis for the Treatment of Peroneal Nerve Palsy: A Systematic Review and Meta-Analysis." Ann Plast Surg, 2021 [PMID: 34397520]
This is a shared conversation. Sign in to Orris to start your own chat.