Describe placental barrier and its importance to anesthetist
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have all the information needed to write a comprehensive answer. Let me compile it.
The Placental Barrier and Its Importance to the Anesthetist
1. Structure of the Placental Barrier
The placenta acts as the interface between maternal and fetal circulations. Maternal blood fills the intervillous space and bathes chorionic villi, through which fetal capillaries run. At term, the placental barrier consists of:
- Syncytiotrophoblast (the main functional layer)
- Cytotrophoblast (reduced at term)
- Villous connective tissue stroma
- Fetal capillary endothelium
At its thinnest (at term), the barrier is only a few micrometers thick, facilitating rapid exchange. This thinning actually increases the rate of drug transfer as pregnancy progresses.
2. Functions of the Placenta Relevant to Anesthesia
Beyond drug transfer, the placenta performs several functions the anesthetist must consider:
- Gas exchange: Oxygen and CO2 transfer (diffusion-limited)
- Nutrient and waste product transfer
- Hormonal secretion: hCG, progesterone, estrogens
- Passive immunity: immunoglobulin transfer
Oxygen Transfer
O2 delivery from the mother to fetus depends on the maternal/fetal blood flow ratio, partial pressure gradient, placental diffusion capacity, hemoglobin concentrations, and O2 affinities. Fetal hemoglobin has a higher O2 affinity (P50: 18 mmHg vs maternal P50: 27 mmHg), shifting the oxyhemoglobin dissociation curve to the left. Fetal PaO2 is normally only 30-40 mmHg and never exceeds 60 mmHg even with maternal 100% O2. CO2 diffuses readily and its transfer is flow-limited. - Miller's Anesthesia, 10e
Protective Limitations
The placental barrier is not a complete barrier - it does NOT reliably exclude viruses (rubella, CMV, varicella), most drugs, or drug metabolites. - Langman's Medical Embryology
3. Mechanisms of Placental Drug Transfer
Drug crosses the placenta by four mechanisms:
| Mechanism | Examples |
|---|---|
| Simple (passive) diffusion | Most anesthetic drugs - the dominant route |
| Facilitated diffusion | Glucose, some vitamins |
| Active (carrier-mediated) transport | Amino acids, nucleosides |
| Pinocytosis / vesicular transport | Large molecules (immunoglobulins) |
Simple diffusion governs most anesthetic drugs and follows Fick's Law:
Q/t = K × A × (Cm - Cf) / D
Where:
-
Q/t = rate of diffusion
-
K = diffusion constant (depends on drug physicochemistry)
-
A = surface area of placenta
-
Cm = free drug concentration in maternal blood
-
Cf = free drug concentration in fetal blood
-
D = membrane thickness
-
Barash Clinical Anesthesia, 9e
4. Physicochemical Factors Determining Transfer Rate
| Factor | Favors Transfer | Reduces Transfer |
|---|---|---|
| Molecular weight | <500 Da (most anesthetic drugs) | >1000 Da (heparin, dextrans) |
| Lipid solubility | High lipophilicity (volatile agents, propofol) | Hydrophilic drugs |
| Ionization (pKa) | Nonionized form crosses freely | Ionized form cannot cross |
| Protein binding | Low binding (lidocaine) | High binding (bupivacaine, ropivacaine) |
| Uteroplacental blood flow | High flow = more delivery | Hypotension, aortocaval compression reduce flow |
Key rule: Drugs that readily cross the blood-brain barrier (BBB) also readily cross the placenta - so essentially all centrally-acting anesthetic agents reach the fetus. - Miller's Anesthesia, 10e
5. Ion Trapping - A Critical Anesthetic Concept
Fetal blood is slightly more acidic (pH ~7.32) than maternal blood (pH ~7.40). Local anesthetics and opioids are weak bases with pKa values of 7.7-8.1. Since only the nonionized form crosses the placenta, once the drug enters the more acidic fetal environment, it becomes ionized and cannot diffuse back. This is called ion trapping.
Clinical implication: During fetal distress with acidemia (pH falls further), ion trapping is exaggerated and local anesthetic concentrations in the fetus can exceed maternal levels. High fetal local anesthetic concentrations can decrease neonatal neuromuscular tone; extremely high levels (e.g., from unintentional intravascular injection) cause fetal cardiac toxicity. - Miller's Anesthesia, 10e; Barash, 9e
6. Fetal Circulation Mitigates Drug Effects
The unique fetal circulatory pattern (shown below) helps buffer the fetal impact of drugs:
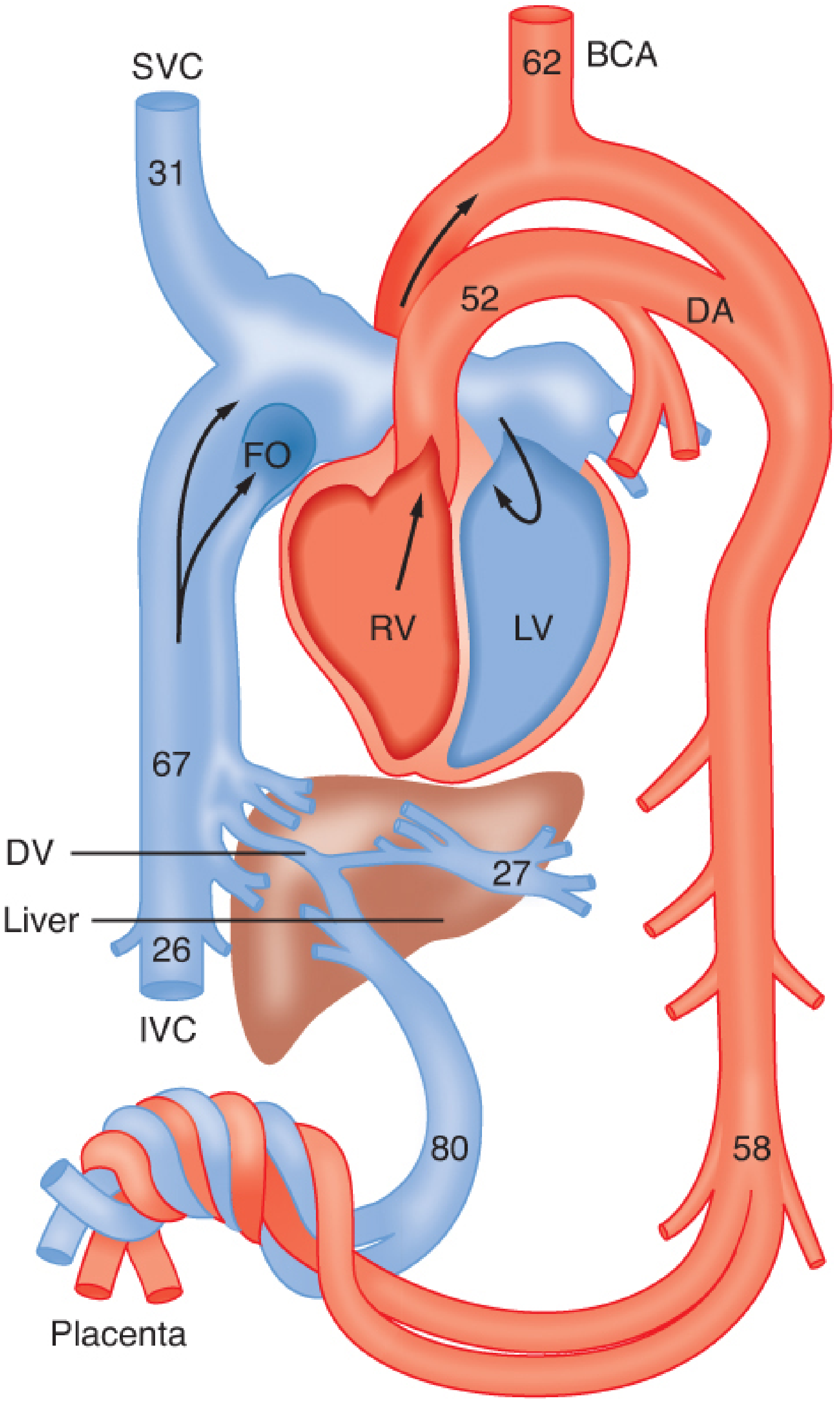
Fetal circulation - numerals indicate mean O2 saturation (%) in key vessels. Note how placental blood (80% saturation) arrives at the liver first, where first-pass hepatic uptake of drugs (e.g., thiopental, lidocaine, halothane) reduces the dose reaching fetal brain. Blood is then progressively diluted by fetal venous blood before reaching the fetal brain. - Barash Clinical Anesthesia, 9e
7. Specific Anesthetic Drug Transfer
Inhalational Agents
All volatile agents (isoflurane, sevoflurane, desflurane, halothane) readily cross the placenta - they are highly lipophilic with low molecular weights. At <1 MAC with delivery within 10 min of induction, fetal depression is generally minimal. Isoflurane has an F/M (fetal/maternal) ratio of approximately 0.7 at ~10 min. Nitrous oxide crosses freely but has minimal uterine blood flow effects when combined with a volatile agent. - Morgan & Mikhail, 7e; Miller's, 10e
Intravenous Induction Agents
- Propofol: Very lipid-soluble, readily crosses; at standard induction doses, distribution and metabolism limit fetal effects
- Ketamine: Crosses readily; at <1.5 mg/kg, uteroplacental blood flow is preserved; at >2 mg/kg, uterine hypertonus can occur
- Thiopental: Crosses quickly; significant hepatic first-pass by fetal liver
- Etomidate: Likely minimal uteroplacental effects, but data limited
Opioids
All opioids cross the placenta. Newborns are especially sensitive to morphine's respiratory depressant effects. Meperidine's neonatal respiratory depression peaks 1-3 hours after maternal administration. Fentanyl has minimal neonatal effects at epidural/intrathecal doses; IV doses >1 mcg/kg given just before delivery can cause neonatal depression. Remifentanil crosses readily but is rapidly metabolized by fetal/neonatal plasma esterases.
Local Anesthetics
- Transfer depends on pKa, pH, and protein binding
- Bupivacaine, ropivacaine: Highly protein-bound (α1-acid glycoprotein) → lower fetal levels
- Lidocaine: Lower protein binding → higher relative fetal levels; repeated dosing can accumulate
- Chloroprocaine (2-CP): Least placental transfer of all - rapidly hydrolyzed by maternal plasma cholinesterase before it can cross
- Fetal acidosis (distress) worsens ion trapping of all local anesthetics except chloroprocaine
Muscle Relaxants
All neuromuscular blocking drugs have minimal placental transfer because they are:
- Highly ionized (quaternary ammonium structure)
- High molecular weight
- Poor lipid solubility
Therefore, during cesarean delivery under general anesthesia, the fetus/neonate is not paralyzed. Succinylcholine, despite its low molecular weight, is also highly ionized and does not cross at clinical doses. - Miller's, 10e
Other Drugs
| Drug | Transfer | Reason |
|---|---|---|
| Glycopyrrolate | Minimal | Highly ionized quaternary structure |
| Atropine, Scopolamine | Ready transfer | Tertiary amines, lipid soluble |
| Heparin | None | High molecular weight, highly charged |
| Ephedrine | Yes | Lipid soluble |
| Labetalol, Esmolol | Yes | Cross freely |
| Metoclopramide | Yes | Crosses readily |
| Dexmedetomidine | Partially | Crosses but is stored/retained within placental tissue |
8. Effect of Anesthetic Agents on Uteroplacental Blood Flow
This is equally important because reduced uteroplacental blood flow limits O2 delivery and can cause fetal hypoxia, regardless of direct drug toxicity:
-
Propofol, barbiturates: Dose-dependent reduction via maternal hypotension; too light a plane causes sympathetic activation with vasoconstriction
-
Ketamine (<1.5 mg/kg): No significant reduction - hypertensive effect counteracts vasoconstriction; useful for hypotensive parturients
-
Volatile agents (<1 MAC): Minor, dose-dependent reductions; cause uterine relaxation (useful for external cephalic version, retained placenta)
-
Spinal/epidural anesthesia: No direct reduction, but hypotension (if untreated) is the primary threat - must be actively prevented/treated with fluids and vasopressors
-
High lidocaine levels (intravascular): Uterine arterial vasoconstriction - a danger in paracervical blocks
-
Aortocaval compression (supine position): Reduces uteroplacental flow mechanically - always use left lateral tilt in the third trimester
-
Morgan & Mikhail, 7e
9. Summary for Clinical Practice
| Clinical Scenario | Key Anesthetic Consideration |
|---|---|
| Cesarean - GA induction | Propofol/thiopental cross rapidly; minimize induction-to-delivery interval |
| Epidural labor analgesia | Bupivacaine/ropivacaine preferred (high protein binding = lower fetal exposure); chloroprocaine safest if fetal distress |
| Fetal distress/acidemia | Ion trapping worsens - local anesthetic accumulates in fetus; switch to chloroprocaine |
| Maternal hypotension (spinal) | Reduces uteroplacental flow; treat promptly with phenylephrine/ephedrine + IV fluids + left tilt |
| NMBDs at cesarean | No fetal paralysis; safe to use |
| Atropine needed maternally | Crosses placenta - can cause fetal tachycardia; glycopyrrolate does not cross |
| Opioid labor analgesia | Time morphine/meperidine to avoid peak fetal levels at delivery; fentanyl epidurally is relatively safe |
Sources:
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - "Placental Drug Transfer," pp. 3480-3483
- Miller's Anesthesia, 10e - "Drug Transfer" (Obstetric Anesthesia chapter), pp. 8823-8824
- Morgan & Mikhail's Clinical Anesthesiology, 7e - "Placental Transfer of Anesthetic Agents," pp. 1583-1586
- Langman's Medical Embryology - "The Placental Barrier"
This is a shared conversation. Sign in to Orris to start your own chat.