I now have comprehensive information from Harrison's and Goldman-Cecil to compose a full, well-structured answer. Let me compile everything.
Hypertension: Standard Treatment Protocol, Drug Changes & Investigations
1. Classification of Blood Pressure (ACC/AHA 2017)
| Category | SBP (mmHg) | DBP (mmHg) |
|---|
| Normal | <120 | <80 |
| Elevated | 120-129 | <80 |
| Stage 1 Hypertension | 130-139 | 80-89 |
| Stage 2 Hypertension | ≥140 | ≥90 |
| Hypertensive Crisis | >180 | >120 |
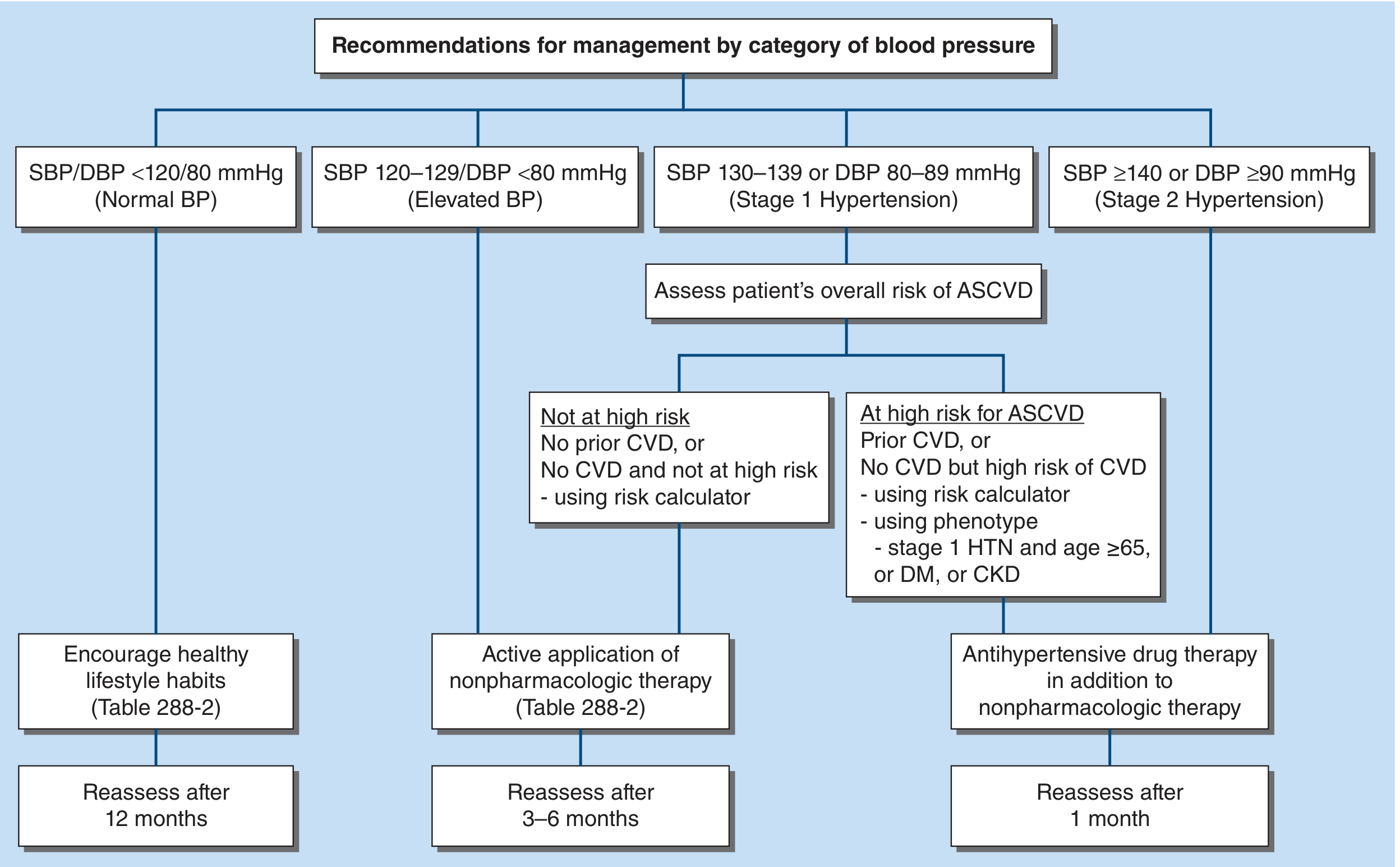
2. Initial Approach - When to Start Treatment
Harrison's Principles of Internal Medicine 22E (2025) - Figure 283
| BP Category | Action |
|---|
| Normal | Encourage healthy lifestyle; reassess in 12 months |
| Elevated BP (120-129/<80) | Active nonpharmacologic therapy; reassess in 3-6 months |
| Stage 1 + NOT high ASCVD risk | Nonpharmacologic therapy; reassess in 3-6 months |
| Stage 1 + HIGH ASCVD risk (prior CVD, DM, CKD, age ≥65) | Drug therapy + nonpharmacologic; reassess in 1 month |
| Stage 2 (≥140/90) | Drug therapy + nonpharmacologic immediately |
3. Non-Pharmacological (Lifestyle) Treatment - MANDATORY First Step
All patients with hypertension or elevated BP require lifestyle modification:
| Intervention | Expected SBP Reduction |
|---|
| Weight loss (~10 lb / 4.5 kg) | ~5 mmHg |
| DASH diet | ~5 mmHg |
| Sodium restriction (<1.5 g/day) | 4-5 mmHg |
| Aerobic exercise (90-150 min/week) | 4-5 mmHg |
| Limit alcohol (men ≤2 drinks/day, women ≤1) | 3-4 mmHg |
| Smoking cessation | Cardiovascular risk reduction |
The DASH diet (high in vegetables, fruits, whole grains, low-fat dairy; low in fats and cholesterol) is the best-studied dietary intervention.
- Harrison's Principles of Internal Medicine 22E, p. 2184-2185
4. Pharmacological Treatment - First-Line Drugs
Guidelines recommend initiating with two or more of three main drug groups:
- Calcium-Channel Blockers (CCBs)
- ACE Inhibitors (ACEi) or Angiotensin Receptor Blockers (ARBs)
- Thiazide or Thiazide-like Diuretics
Beta-blockers are no longer recommended as initial therapy. They are less effective for stroke prevention compared to first-line agents, though they remain useful in patients with heart failure or ischemic heart disease.
- Goldman-Cecil Medicine, p. 750
First-Line Drug Doses
| Drug Class | Example Agents | Typical Dose | Frequency |
|---|
| Thiazide diuretics | Chlorthalidone | 12.5-25 mg/day | Once daily |
| Hydrochlorothiazide (HCTZ) | 25-50 mg/day | Once daily |
| ACE Inhibitors | Lisinopril | 10-40 mg/day | Once daily |
| Ramipril | 2.5-20 mg/day | Once or twice daily |
| Enalapril | 5-40 mg/day | Once or twice daily |
| ARBs | Losartan | 25-100 mg/day | Once or twice daily |
| Telmisartan | 20-80 mg/day | Once daily |
| Valsartan | 80-320 mg/day | Once daily |
| CCBs (DHP) | Amlodipine | 2.5-10 mg/day | Once daily |
| Nifedipine ER | 30-90 mg/day | Once daily |
5. Compelling Indications - Disease-Specific Drug Choices
| Condition | Preferred Drug | Avoid |
|---|
| Heart failure (HFrEF) | ACEi/ARB + beta-blocker + MRA (spironolactone) | Non-DHP CCBs (verapamil, diltiazem) |
| Post-MI | ACEi/ARB + beta-blocker | - |
| Diabetes mellitus | ACEi or ARB (nephroprotective) | - |
| CKD with proteinuria | ACEi or ARB | DHP-CCB as monotherapy |
| Stroke prevention | ACEi/ARB + CCB or diuretic | - |
| Angina | Beta-blocker or CCB | - |
| Pregnancy | Methyldopa, Labetalol, Nifedipine | ACEi, ARBs (teratogenic) |
| Gout | Avoid thiazides | Thiazides (raise uric acid) |
| Asthma/COPD | CCB or ACEi/ARB | Beta-blockers |
| Bilateral renal artery stenosis | CCB | ACEi/ARBs (contraindicated) |
- National Kidney Foundation Primer on Kidney Diseases, 8e, p. 691
6. BP Targets
| Population | Target BP |
|---|
| General adult | <130/80 mmHg (ACC/AHA 2017) |
| Elderly (most guidelines) | <140/90 mmHg initially, then <130/80 if tolerated |
| CKD (KDIGO 2021) | SBP <130 mmHg |
| Diabetes (ADA) | <130/80 mmHg |
| High CVD risk | SBP <120 mmHg (SPRINT-like) |
7. Step-Up Therapy - When and How to Change the Drug
Indications to Change or Add a Drug
- BP not at target after 4-6 weeks at adequate dose
- Significant side effects from current drug
- Contraindication develops (e.g., ACEi causing angioedema - switch to ARB)
- New comorbidity that favors a different class (e.g., MI develops - add beta-blocker)
- Resistant hypertension (BP uncontrolled on 3 drugs including a diuretic at max doses)
Step Therapy Protocol
STEP 1: Lifestyle modification alone
(if not at target in 3-6 months, or immediate drug Rx if high-risk)
STEP 2: Start 1-2 first-line drugs (ACEi/ARB + CCB, or + thiazide)
- Reassess in 4-6 weeks
STEP 3: Increase dose of existing drug OR add second first-line drug
- Preferred combinations: ACEi/ARB + CCB, or ACEi/ARB + thiazide
- Avoid: ACEi + ARB together (increased renal/hyperkalemia risk)
STEP 4: 3-drug combination (ACEi/ARB + CCB + thiazide diuretic)
- If still uncontrolled = RESISTANT HYPERTENSION
STEP 5 (Resistant HTN): Add spironolactone 25-50 mg/day
(most effective 4th-line agent; check K+/eGFR first)
Alternative: amiloride, doxazosin, or clonidine
When switching due to side effects:
- ACEi cough → switch to ARB
- ACEi/ARB angioedema → switch to ARB (for ACEi angioedema) - but if severe, avoid both
- CCB ankle edema → add ACEi/ARB (reduces edema) or switch to non-DHP CCB
- Thiazide hyperkalemia/gout → switch to another class
Check serum creatinine and electrolytes within 1-2 weeks after starting or changing ACEi/ARB.
- Goldman-Cecil Medicine, p. 751
8. Monitoring After Starting/Changing Treatment
| Timepoint | What to Check |
|---|
| 1-2 weeks after ACEi/ARB start | Serum creatinine, potassium |
| 4-6 weeks after any change | Repeat BP measurement (office + home) |
| 3 months | BP target achievement, side effects, adherence |
| Annually | Full metabolic panel, renal function, urine ACR |
Criteria for stopping drug:
- Creatinine rise >30% above baseline on ACEi/ARB (suggests bilateral renal artery stenosis)
- Potassium >5.5 mEq/L on ACEi/ARB/MRA
- Symptomatic hypotension
9. Investigations
Baseline (All Patients at Diagnosis)
| Investigation | Purpose |
|---|
| Fasting blood glucose / HbA1c | Screen for diabetes |
| Fasting lipid panel | Total cardiovascular risk |
| Serum creatinine + eGFR | Renal function, CKD detection |
| Serum electrolytes (Na+, K+) | Baseline before drugs; screen for hyperaldosteronism (low K+) |
| Uric acid | Baseline before thiazides; gout history |
| Urinalysis + urine albumin:creatinine ratio (ACR) | Proteinuria = target organ damage |
| ECG | Left ventricular hypertrophy, ischemia |
| CBC | Anaemia, secondary causes |
For Target Organ Damage Assessment
| Test | Detects |
|---|
| Echocardiogram | LVH, systolic/diastolic dysfunction |
| Fundoscopy | Hypertensive retinopathy |
| Ankle-brachial index | Peripheral arterial disease |
| Brain imaging (CT/MRI) | Prior stroke, white matter changes |
Investigations for Secondary Hypertension
(Suspect if: age <30, resistant to 3+ drugs, hypokalemia, paroxysmal symptoms, abrupt onset)
| Suspected Cause | Test |
|---|
| Primary hyperaldosteronism | Aldosterone-renin ratio (ARR); plasma aldosterone |
| Renal artery stenosis | Renal Doppler USS; CT angiography |
| Pheochromocytoma | 24-hr urine metanephrines; plasma metanephrines |
| Cushing's syndrome | 24-hr urine cortisol; 1 mg dexamethasone suppression test |
| Obstructive sleep apnea | Sleep study (polysomnography) |
| Coarctation of aorta | CT aorta; BP difference between arms and legs |
| Hypothyroidism | TSH |
| Renal parenchymal disease | Renal USS, eGFR, urine PCR |
10. Special Situations
| Situation | Management |
|---|
| Hypertensive urgency (SBP >180, no end-organ damage) | Oral agents (captopril, clonidine, labetalol); reduce BP over 24-48 hours |
| Hypertensive emergency (SBP >180 + end-organ damage) | IV labetalol, nicardipine, or sodium nitroprusside; ICU admission; reduce MAP by ≤25% in first hour |
| Resistant hypertension | Confirm adherence, exclude white coat, check for secondary causes; add spironolactone as 4th agent |
| Pregnancy | Methyldopa, labetalol, nifedipine; avoid ACEi/ARBs |
| Elderly | Start with lower doses; prefer diuretic or CCB; SBP goal <130 mmHg if tolerated |
| CKD | ACEi or ARB preferred; monitor K+ and creatinine closely |
Key sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 283 & 288
- Goldman-Cecil Medicine, Chapter 64
- National Kidney Foundation Primer on Kidney Diseases, 8e, Chapter 64
- ACC/AHA 2017 Hypertension Guidelines