Pathophysiology clinical feature investigation and management of torsion testis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"testicular torsion"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have all the comprehensive information needed from multiple authoritative textbooks. Let me compile the full detailed answer.
Torsion of the Testis
Definition
Testicular torsion is the twisting of the spermatic cord and its contents such that the testicular blood supply becomes compromised. It is a surgical emergency - if left untreated, blood flow to the testicle ceases and the testicle undergoes ischaemic necrosis.
- Incidence: 3.8-4.5 per 100,000 males under 18 years annually
- Accounts for 10-15% of acute scrotal disease in children
- Most common between ages 10 and 25 years
Pathophysiology
Types of Torsion
1. Extravaginal Torsion
- Seen almost exclusively in neonates
- Occurs due to increased mobility of the testicle before it descends into the scrotum and becomes attached to the scrotal wall via the tunica vaginalis
- The entire spermatic cord, including the tunica vaginalis, twists
2. Intravaginal Torsion
- The predominant type beyond the neonatal period
- Results from one or more anatomical predispositions:
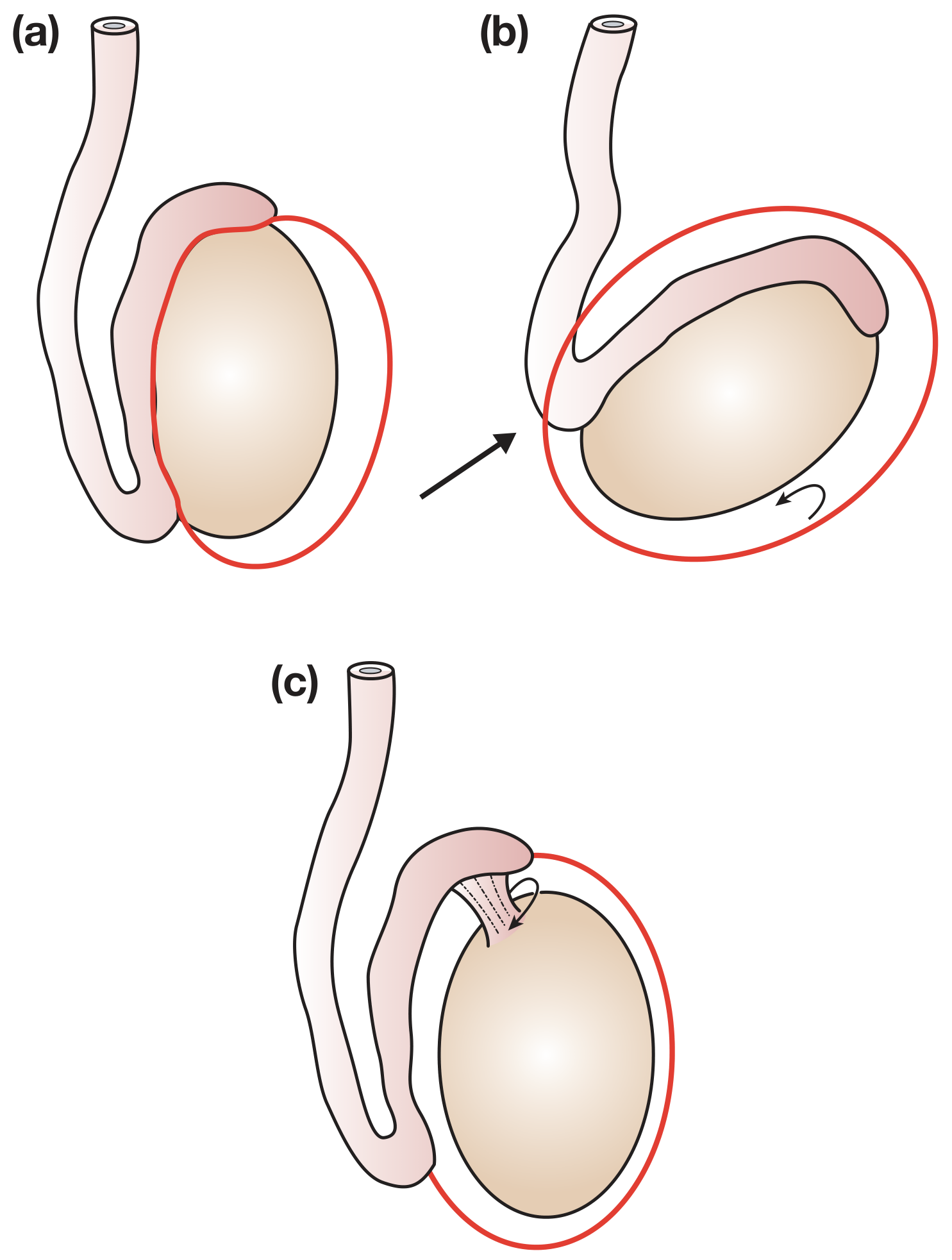
a) Bell-Clapper Deformity (most common cause in adolescents)
High investment of the tunica vaginalis causes the testis to hang freely within the tunica - like a clapper in a bell. This is typically a bilateral anatomical abnormality, which is why the contralateral testis must always be fixed.
b) Inversion of the testis - the testis lies transversely or upside down
c) Separation of the epididymis from the body of the testis, permitting torsion of the testis on the pedicle connecting them
Precipitating Factors
Normally, cremasteric contraction pulls the testis upward. In the presence of the anatomical abnormalities above, the spiral attachment of the cremaster favours rotation around the vertical axis. Precipitants include:
- Physical activity (straining, lifting, sport)
- Sexual activity
- Thermal stimulation
- Occasionally occurs during sleep (cremasteric reflex while waking)
Degree of Torsion and Ischaemia
- Twists of 720° cause more rapid ischaemia than twists of 360° or less
- Duration-dependent damage: venous outflow obstructed first, then arterial inflow
- Contralateral testicular biopsy findings are abnormal in 57-88% of males when torsion occurs, suggesting underlying bilateral spermatogenic dysfunction
Consequence of Torsion
- Up to 50% of men develop adverse spermatogenic effects after torsion
- 36-39% will have sperm concentrations below 20 million/mL
- Up to 11% develop antisperm antibodies due to disruption of the blood-testis barrier (tight junctions between Sertoli cells)
Clinical Features
Classic presentation in a 10-25-year-old male:
| Feature | Detail |
|---|---|
| Onset of pain | Sudden, severe - patient can often state exact time it started |
| Location of pain | Groin and lower abdomen (can mimic appendicitis) |
| Associated symptoms | Nausea and vomiting (sudden onset, distinguishes from epididymo-orchitis) |
| Scrotal appearance | Swollen, firm, tense, reddened - not erythematous early on |
| Testicular position | High-riding testis (pulled upward by twisted cord) |
| Cord palpation | Tender, thickened twisted cord often palpable above the testis |
| Temperature | Apyrexial (fever favours epididymo-orchitis) |
| Cremasteric reflex | Absent (important sign - reflex is present in epididymo-orchitis and appendage torsion) |
| Elevation test (Prehn's sign) | Pain worsens with testicular elevation (in epididymo-orchitis, elevation relieves pain) |
Important note: Torsion may also occur in neonates - presenting as a hard, painless scrotal mass with skin discolouration (often detected at birth).
Intermittent torsion: Acute, short-duration (<2 hours) scrotal pain with rapid, spontaneous resolution. Nausea and vomiting in ~25% of cases. Must be taken seriously and treated with orchiopexy.
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Epididymo-orchitis | Gradual onset, fever, dysuria, urethral discharge, normal cremasteric reflex, pain relieved by elevation |
| Appendage torsion (Hydatid of Morgagni) | Milder pain, gradual onset, upper pole tenderness, "blue dot sign" (in fair-skinned children early), cremasteric reflex intact |
| Mumps orchitis | Cord not thickened, often bilateral, parotitis history |
| Idiopathic scrotal oedema | Age 4-12, bilateral swelling with minimal pain, extends to perineum/groin/penis |
| Strangulated inguinal hernia | Inguinal mass, bowel obstruction symptoms |
Investigations
Clinical Priority First
The management decision is primarily clinical. Do NOT delay surgical exploration awaiting investigation if clinical suspicion is high.
1. Doppler Ultrasound (most commonly used)
- Can confirm absence of blood flow to the affected testis
- Sensitivity 92-100% for confirming epididymitis
- Absence of blood flow = torsion until proven otherwise
- Caveat: False-positive results (apparent flow) can occur, so it is not routinely recommended as a reason to withhold surgery. A positive Doppler (flow present) does not absolutely exclude torsion.
2. Radionuclide Scanning (Technetium-99m scan)
- Uptake of tracer into the centre of the testis rules out torsion
- Less available, rarely used in acute setting
3. Urinalysis
- Normal in testicular torsion (WBCs and bacteria suggest epididymo-orchitis)
4. FBC/Bloods
- Leukocytosis suggests infection rather than torsion
- No specific blood test for torsion
Key principle from Smith & Tanagho's General Urology:
"The presence of blood flow in the testis on Doppler ultrasonography or uptake of tracers into the center of the testis on radionuclide scanning rules out torsion."
Management
Time is Testis - Salvage Rates by Duration
| Time from Onset | Testicular Salvage Rate |
|---|---|
| < 6 hours | ~100% |
| 6-12 hours | ~70% |
| 12-24 hours | ~20% |
| > 24 hours | Very low / near 0% |
Step 1: Immediate Urological Consultation
Upon presentation, early urology consultation is critical - even before confirmatory imaging in high-suspicion cases.
Step 2: Manual Detorsion (can be attempted in ED)
- Testis usually rotates medially (inward), so manual detorsion involves rotating it outward (laterally), like opening a book
- If successful, pain relief is immediate and vascular flow restored
- This is a temporising measure only - does not negate need for surgical fixation
Step 3: Emergency Surgical Exploration
Incision: Transverse or midline scrotal incision
Intraoperative decision-making:
a) If testis is viable after detorsion:
- Fix with 3 non-absorbable sutures between the tunica albuginea and the scrotal raphe (orchiopexy)
- Absorbable sutures must NOT be used (risk of recurrent torsion as suture dissolves)
- Fix the contralateral testis as well - the anatomical predisposition is bilateral
b) If viability is uncertain:
- Wrap the testis in a warm swab and observe for several minutes
- Make a small incision in the tunica albuginea - if bright red arterial bleeding is seen, the testis may survive
- Fix as above if viable
c) If testis is infarcted (necrotic):
- Orchiectomy is performed - the dead testis must be removed
- Counsel the patient about testicular prosthesis later
- Still fix the contralateral testis to prevent future torsion
Step 4: Contralateral Orchiopexy
Always performed simultaneously with ipsilateral fixation/orchiectomy. The bell-clapper deformity is bilateral in the majority of cases.
Step 5: Cases With Prolonged History (Several Days)
- The affected testis will already be infarcted
- Little can be gained (other than pain relief) by immediate exploration of the affected side
- However, urgent contralateral fixation is still necessary
Orchiopexy Techniques (for intermittent/elective cases)
- Suture fixation - 3-0 non-absorbable sutures fixing tunica albuginea to dartos muscle or scrotal raphe
- Dartos pouch procedure - testis placed in a subcutaneous pouch between dartos and external spermatic fascia, secured by purse-string suture; preferred by some as it avoids intratesticular vessel injury
Summary Algorithm
Acute Scrotal Pain
↓
High clinical suspicion for torsion?
↓
YES → Emergency surgical exploration (do not delay)
↓
Viable testis? → Bilateral orchiopexy (non-absorbable sutures)
Infarcted? → Orchiectomy + contralateral orchiopexy
NO / Uncertain → Doppler ultrasound
↓
No flow → Emergency exploration
Flow present + confident alternative diagnosis → Treat accordingly
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1582-1584 (Torsion of the Testis)
- Campbell-Walsh-Wein Urology, 3-Volume Set, pp. 1612-1614; 1180-1184 (Testis Torsion; Intermittent Torsion)
- Smith and Tanagho's General Urology, 19th Ed., p. 787 (Distinguishing Torsion)
- Rosen's Emergency Medicine: Concepts and Clinical Practice, p. 1595 (Disposition and Management)
This is a shared conversation. Sign in to Orris to start your own chat.