Coronary circulation physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative physiology textbooks and three excellent diagrams. Let me compile the full answer.
Coronary Circulation Physiology
1. Anatomical Overview
The coronary arteries arise from the root of the aorta, just above the aortic valve cusps, and lie on the epicardial surface of the heart before sending smaller branches that penetrate into the myocardium.
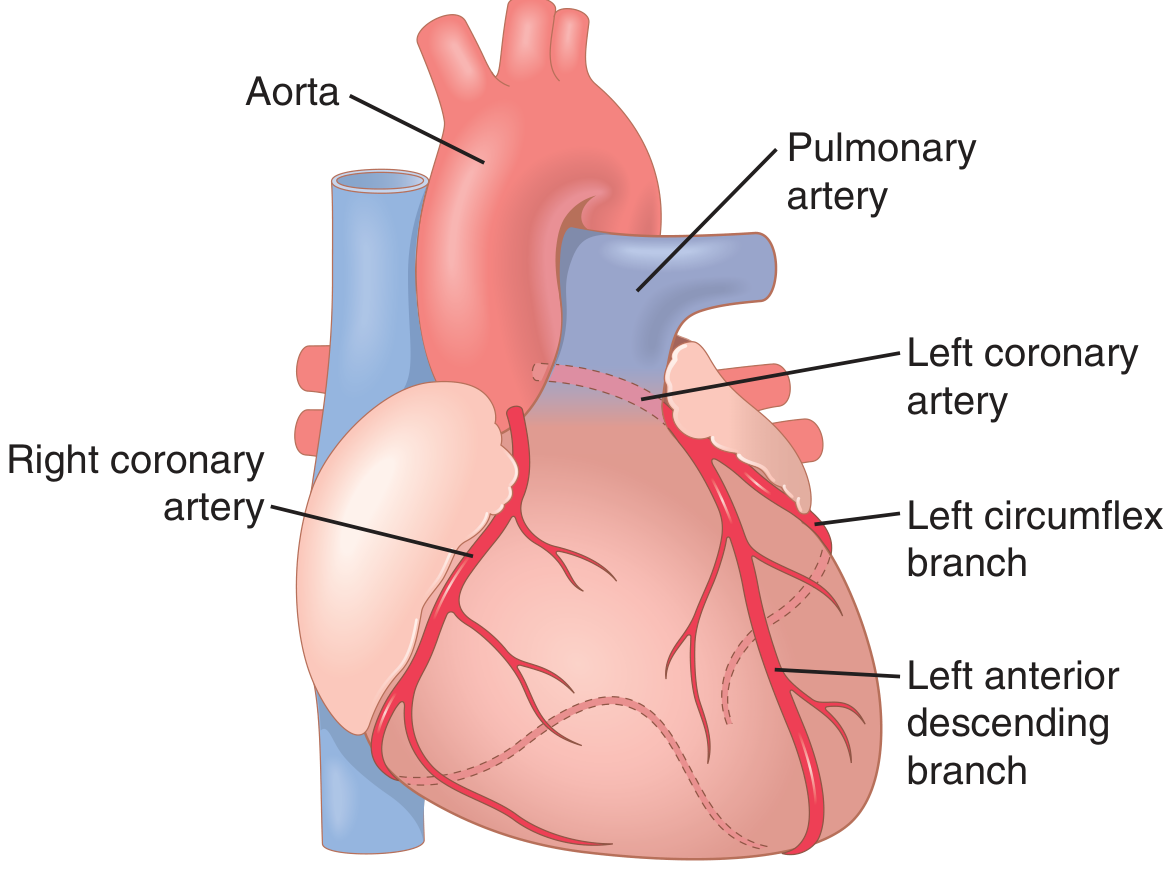
Left coronary artery (LCA) divides into:
- Left anterior descending (LAD) - supplies the anterior and apical left ventricle plus the interventricular septum
- Left circumflex - supplies the lateral and posterior left ventricular wall
Right coronary artery (RCA) supplies:
- The right ventricle
- The posterior left ventricle in ~80-90% of people (right-dominant circulation)
- The SA and AV nodes in most individuals
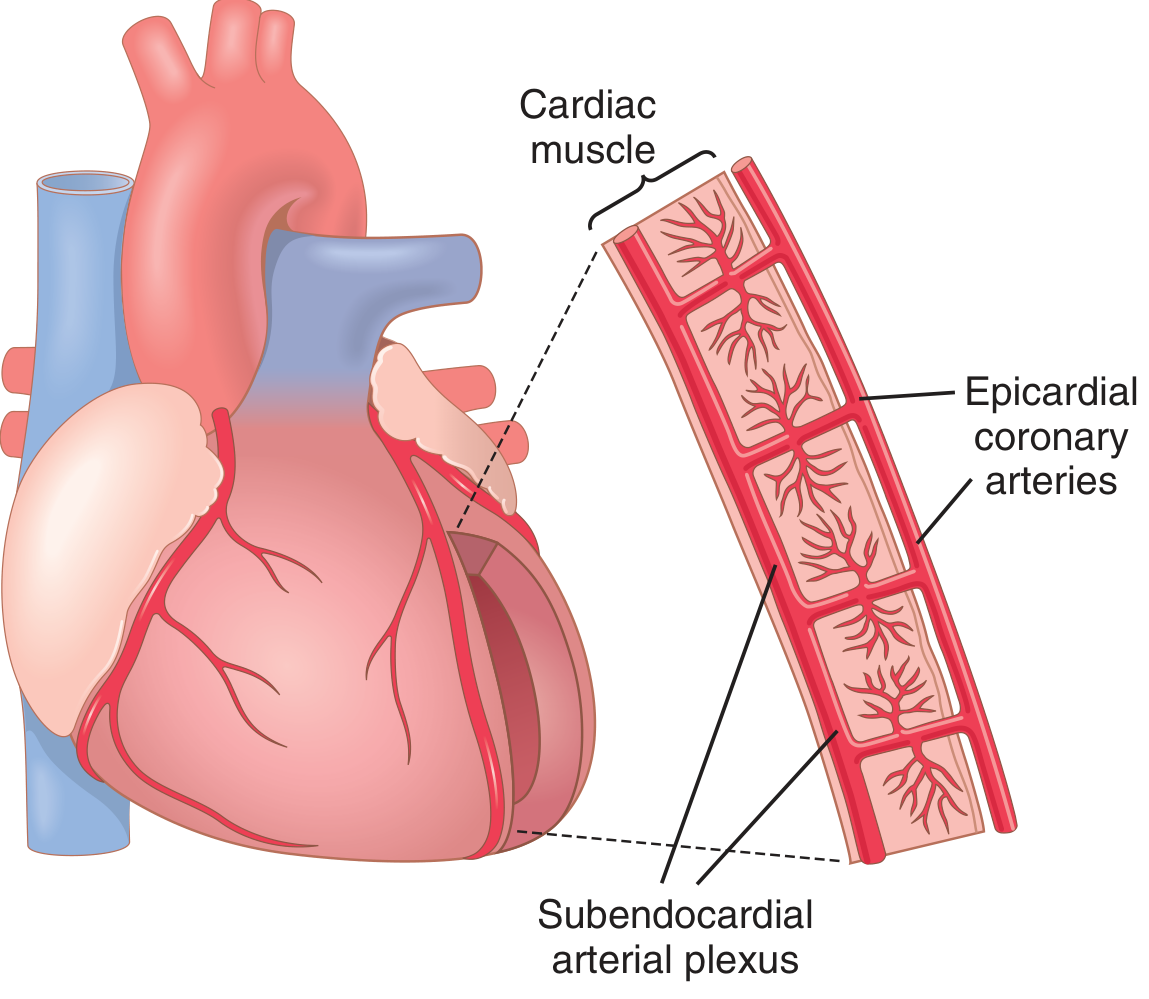
Only the innermost ~0.1 mm of the endocardium can be directly nourished by intracavitary blood; all the rest depends entirely on coronary perfusion.
- Guyton and Hall Textbook of Medical Physiology, p. 268
2. Coronary Venous Drainage
| Venous pathway | Drains from | Empties into |
|---|---|---|
| Coronary sinus | ~75% of left ventricular coronary venous blood | Right atrium |
| Anterior cardiac veins | Right ventricular muscle | Right atrium (directly) |
| Thebesian veins | Small capillary beds within the ventricular wall | All four cardiac chambers |
The thebesian veins are physiologically important: because their deoxygenated blood exits into the ventricles, it bypasses the pulmonary circulation and contributes to a small physiologic shunt.
- Medical Physiology (Boron & Boulpaep), p. 822
3. Normal Coronary Blood Flow Values
| Parameter | Value |
|---|---|
| Resting coronary flow | ~70 mL/min/100 g myocardium |
| Total resting flow | ~225 mL/min |
| Fraction of cardiac output | 4-5% |
| O2 extraction at rest | 70-80% of arterial O2 content |
| Coronary venous PO2 | Very low (~5 mL/dL O2) |
Because the heart already extracts 70-80% of delivered oxygen at rest (compared to ~25% in most other organs), the myocardium has virtually no O2 extraction reserve. The only way to increase O2 delivery with increased workload is to increase coronary blood flow itself.
- Guyton and Hall Textbook of Medical Physiology, p. 268-269
- Medical Physiology (Boron & Boulpaep), p. 824
During strenuous exercise, cardiac work can increase 6-9 fold, while coronary flow increases 3-4 fold - the deficit is bridged by an improvement in cardiac metabolic efficiency.
4. Phasic Nature of Coronary Blood Flow (Systole vs Diastole)
This is one of the most distinctive features of the coronary circulation. Unlike other vascular beds where flow tracks aortic pressure, coronary flow is paradoxically impaired during systole.
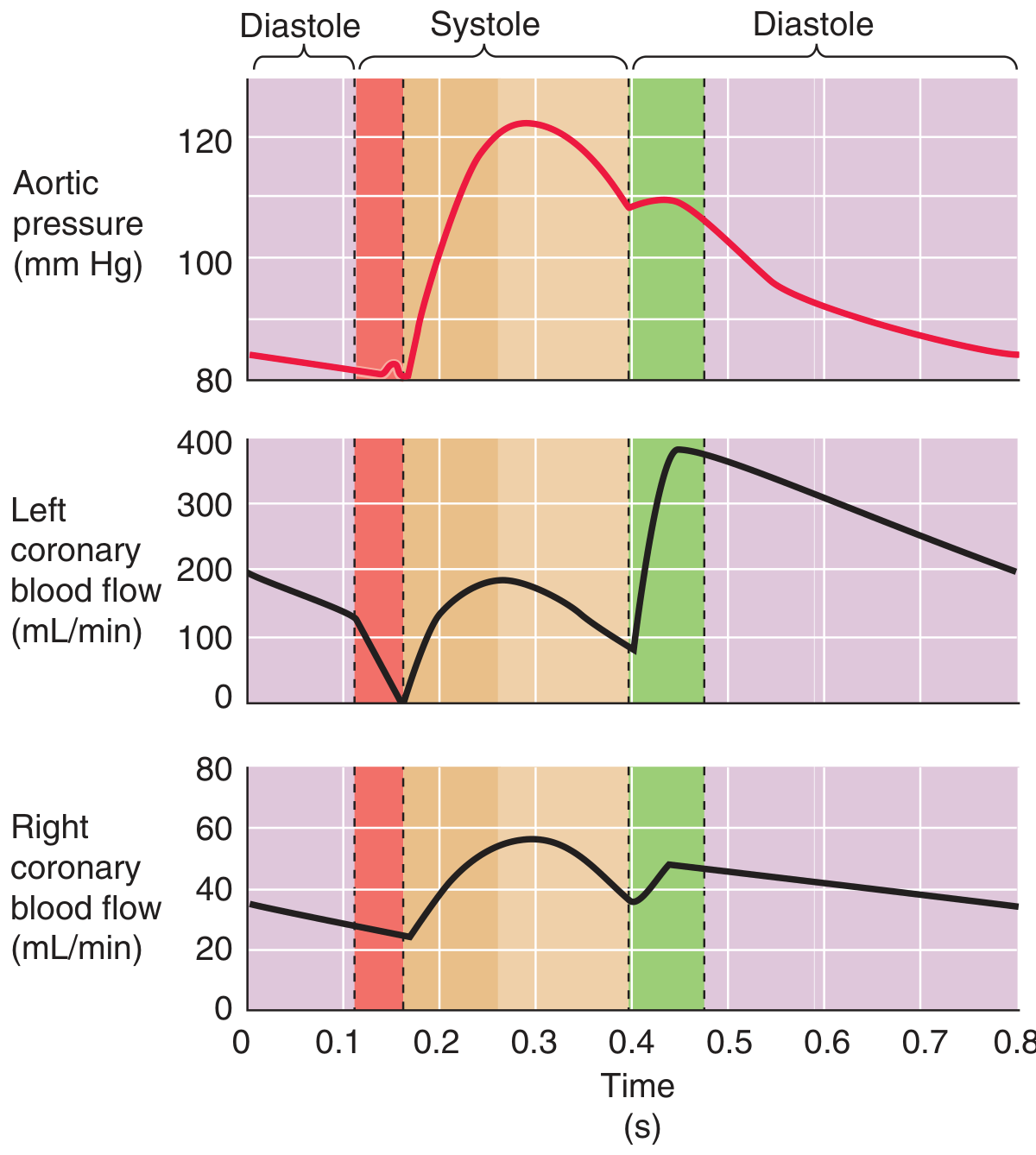
Left coronary artery:
- During isovolumetric contraction, flow may transiently reverse because the LV compresses its own coronary vessels before the aortic valve opens
- During the remainder of systole, flow increases but never reaches peak values
- ~80% of total left coronary flow occurs during diastole - when the relaxed ventricle no longer compresses vessels, and aortic pressure is still relatively high
- Clinical implication: tachycardia shortens diastole disproportionately, reducing time for left coronary perfusion
Right coronary artery:
-
The RCA flow profile much more closely resembles aortic pressure (rises in systole)
-
Systolic reversal does not occur because the right ventricle pumps against low pulmonary resistance, generating far less wall tension than the LV
-
Systole contributes a greater proportion of RCA total flow than LCA total flow
-
Medical Physiology (Boron & Boulpaep), p. 823
-
Costanzo Physiology 7th Edition, p. 198
Endo- vs Epicardial perfusion:
During systole, intramyocardial pressure is highest near the endocardium. To compensate, the subendocardium has lower intrinsic vascular resistance, giving it preferentially higher diastolic flow. This balance is easily disrupted:
- Low diastolic aortic pressure (e.g., aortic regurgitation)
- High coronary resistance (e.g., atherosclerosis)
In either condition, subendocardial flow falls below epicardial flow - explaining why the inner left ventricular wall is the most vulnerable to ischemic damage in coronary artery disease.
5. Regulation of Coronary Blood Flow
A. Local Metabolic Control (Primary Mechanism)
Coronary blood flow is regulated almost entirely by local metabolites, tightly coupled to myocardial O2 demand. This is the dominant control mechanism.
Key vasodilators released from ischemic/active myocardium:
| Vasodilator | Mechanism |
|---|---|
| Adenosine | ATP → AMP → adenosine; activates purinergic receptors on VSMCs, lowers [Ca²+], causing vasodilation. Most studied mediator. |
| Hypoxia (low PO2) | Direct effect on vascular smooth muscle |
| CO2 / H+ | Acidosis from increased metabolism → vasodilation |
| K+ ions | Released early during increased cardiac work; transient initial vasodilation |
| Prostaglandins | Local vasodilator prostaglandins (PGI2) |
| Nitric oxide (NO) | Endothelium-derived; important in flow-mediated dilation |
Active hyperemia: When myocardial contractility increases → O2 demand rises → local hypoxia → adenosine release → arteriolar vasodilation → increased coronary flow to match demand.
Reactive hyperemia: After a period of mechanical compression (systole) or coronary occlusion, blood flow surges above baseline when compression is released, repaying the O2 debt incurred during the occlusion period.
- Costanzo Physiology 7th Edition, p. 197
- Guyton and Hall Textbook of Medical Physiology, p. 269-270
B. Autoregulation
Coronary blood flow remains relatively constant between perfusion pressures of approximately 70 to >150 mmHg. This autoregulatory behavior is similar to that of the cerebral circulation and is mediated by:
- Myogenic response of arteriolar smooth muscle
- Metabolic mechanisms (fluctuations in adenosine and PO2)
Below ~70 mmHg diastolic coronary perfusion pressure, autoregulation fails and flow becomes pressure-dependent - this is the "break point" below which ischemia begins.
- Medical Physiology (Boron & Boulpaep), p. 824
C. Nervous (Autonomic) Control
Autonomic effects are secondary to the dominant metabolic control - they affect coronary flow mostly indirectly by changing cardiac workload.
Sympathetic stimulation:
- Indirect (dominant) effect: Increases heart rate and contractility via β1 receptors → increases myocardial O2 consumption → metabolic vasodilation overrides direct vasoconstriction
- Direct effect: Epicardial vessels are predominantly α-receptor bearing → vasoconstriction; intramuscular vessels have more β2 receptors → vasodilation
- Net result: Overall coronary vasodilation due to indirect metabolic effects
Vagal (parasympathetic) stimulation:
- Direct effect: Acetylcholine causes mild coronary vasodilation
- Indirect effect: Slows heart rate and reduces contractility → decreased O2 consumption → indirect coronary constriction
- Net result: Indirect effects reduce coronary flow to match reduced demand
Important: In some individuals with disproportionately strong α-vasoconstrictor responses, sympathetic excess can trigger vasospastic myocardial ischemia (variant/Prinzmetal angina), even with angiographically normal vessels.
- Guyton and Hall Textbook of Medical Physiology, p. 269-270
6. Cardiac Metabolism and O2 Utilization
| Feature | Detail |
|---|---|
| Primary fuel at rest | Fatty acids (~70% of energy) |
| Alternative fuels | Glucose, lactate, amino acids |
| During ischemia | Forced to use anaerobic glycolysis → lactic acid accumulation (contributes to anginal pain) |
| ATP use | >95% of metabolic energy is channeled through mitochondrial ATP production |
Because coronary O2 extraction is near-maximal at rest, any increase in cardiac work can only be met by increasing flow - not by extracting more oxygen from existing flow. This makes the heart uniquely dependent on adequate coronary perfusion and vulnerable to ischemia with supply-demand mismatch.
7. Key Clinical Correlates
| Condition | Physiological Basis |
|---|---|
| Subendocardial ischemia first in CAD | Endocardium most compressed in systole, least perfusion reserve |
| Tachycardia dangerous in CAD | Shortens diastole → less time for left coronary perfusion |
| Aortic regurgitation causes subendocardial ischemia | Low diastolic aortic pressure impairs diastolic left coronary flow |
| Ventricular fibrillation briefly improves LCA flow | Eliminates mechanical compression of vessels |
| Adenosine as pharmacologic vasodilator | Basis of adenosine stress testing (mimics active hyperemia) |
| Vasospastic angina | α-receptor excess in epicardial vessels causes pathological spasm |
Sources:
- Guyton and Hall Textbook of Medical Physiology (9780443111013), Chapter 21
- Medical Physiology - Boron & Boulpaep (9780323319737), Chapter 24
- Costanzo Physiology 7th Edition (9780323793339), Chapter on Special Circulations
This is a shared conversation. Sign in to Orris to start your own chat.