
IMG-20260509-WA0045(1).jpg
Briefly explain about this ecg from basic to advanced ,deep level of study
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG early repolarization pattern end QRS notching slurring clinical significance 2024
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Searching Images
early repolarization pattern ECG end QRS notching slurring J wave
Loading Image
Now I have all the information needed for a comprehensive, deep-level ECG analysis. Let me compile the full response.
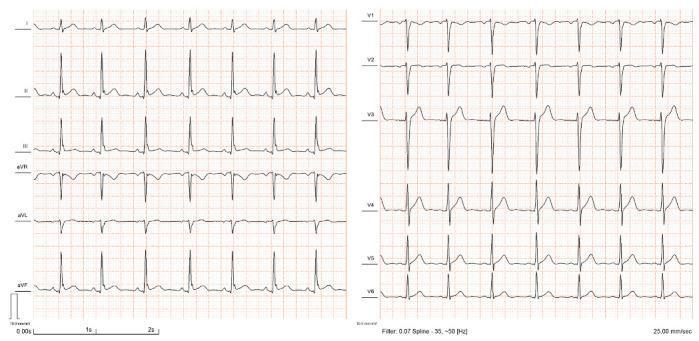
ECG Analysis — Deep Level Study
Patient context: Medicine OPD, recorded 09-05-2026 at 17:40 (Bhagwan Mahavir Aayurvigyan Sansthan)
Machine interpretation: Sinus Rhythm · End QRS notching/slurring · Early repolarization pattern · Normal ECG
PART 1 — ECG BASICS (The Grid & Calibration)

The ECG is recorded at 25 mm/sec speed, 10 mm/mV gain (standard):
- 1 small box (1 mm) = 0.04 sec horizontally / 0.1 mV vertically
- 1 large box (5 mm) = 0.20 sec horizontally / 0.5 mV vertically
The 12 leads recorded:
- Limb leads: I, II, III (bipolar) + aVR, aVL, aVF (augmented unipolar)
- Precordial leads: V1–V6 (unipolar chest)
What each wave represents:
| Wave/Segment | Electrical event |
|---|---|
| P wave | Atrial depolarization (SA node → AV node) |
| PR interval | Conduction through AV node + His-Purkinje |
| QRS complex | Ventricular depolarization |
| ST segment | Early ventricular repolarization (phase 2 plateau) |
| T wave | Ventricular repolarization (phase 3) |
| J point | Junction between end of QRS and start of ST segment |
| QT interval | Total ventricular electrical systole |
PART 2 — SYSTEMATIC READING OF THIS ECG
Rate
HR = 75 bpm (machine measured). Using the large box method: 300 ÷ R-R boxes ≈ 75. This is normal sinus rate (60–100 bpm).
Rhythm
Sinus rhythm. Criteria met:
- P wave before every QRS ✓
- Regular P-P and R-R intervals ✓
- Upright P in II, inverted in aVR ✓ (confirms sinus node origin)
P Wave
Duration = 100 ms (normal ≤ 120 ms). No bifid or biphasic P waves — no atrial enlargement.
PR Interval
146 ms — normal (120–200 ms). AV conduction is intact; no first-degree heart block (which would be >200 ms).
QRS Duration
80 ms — normal (<120 ms). No bundle branch block. Narrow QRS = ventricular activation via the normal His-Purkinje system.
QRS Axis
P/QRS/T axis = 58°/53°/46° — all in the normal quadrant (0° to +90°). No left or right axis deviation.
QT / QTc
- QT = 338 ms, QTc = 364 ms (Hodges formula)
- Normal QTc in males is ≤440 ms, females ≤460 ms
- Not prolonged — low risk of torsades de pointes
Voltage (R-wave amplitudes)
- RV5 = 1.841 mV, SV1 = 0.268 mV
- RV5 + SV1 = 2.109 mV (Sokolow-Lyon criterion for LVH is >3.5 mV)
- No LVH by voltage criteria
R-wave Progression (Precordial leads)
Normal R-wave progression expected: small r in V1 → tall R in V5/V6. Looking at the tracing, V1 shows a near-isoelectric or small complex consistent with normal right precordial morphology; R-wave grows through V2–V5 — normal transition zone.
PART 3 — THE KEY FINDING: END QRS NOTCHING / SLURRING — EARLY REPOLARIZATION PATTERN
What is it?
The machine flags two overlapping descriptors that refer to the same phenomenon:
End QRS notching = a small discrete positive deflection (bump/notch) visible at the very end of the R-wave downstroke, sitting at or just above the J-point baseline.
End QRS slurring = instead of a crisp return to baseline, the terminal QRS slopes gradually (slurs) before transitioning to the ST segment — the slope change ≥ 0.1 mV above baseline.
Both are J-wave morphologies. Collectively they define the:
Early Repolarization Pattern (ERP) — characterized by elevation of the QRS-ST junction (J-point) above baseline, or slurring of the terminal QRS into the ST segment. — Fuster & Hurst's The Heart, 15th Ed.
Diagnostic criteria (MacFarlane et al., 2015)
- Notch or slur at the terminal QRS–ST junction (J-point)
- Jpeak ≥ 1 mm (0.1 mV) in ≥ 2 anatomically contiguous leads
- QRS duration < 120 ms (excludes bundle branch block)
- Leads V1–V3 are excluded from defining ERP (those morphologies suggest Brugada pattern instead)
PART 4 — ADVANCED: ELECTROPHYSIOLOGICAL MECHANISM
Cellular basis
The J-wave arises from a transient outward potassium current (Ito) that is more prominent in ventricular epicardium than endocardium. This creates a transmural voltage gradient at the end of phase 1 of the action potential:
| Layer | Phase 1 notch | Effect on ECG |
|---|---|---|
| Epicardium | Large Ito → prominent notch/spike | J-point elevation on surface ECG |
| Endocardium | Small Ito → no notch | Contributes to voltage gradient |
The resulting epicardial action potential dome is taller initially but repolarizes earlier than endocardium — hence the name "early repolarization."
Phase 2 re-entry (an advanced arrhythmia mechanism): If the Ito gradient is exaggerated (e.g., by sodium channel blockade, hypothermia, genetics), the epicardial dome can disappear in some regions but not others. This creates local re-excitation (phase 2 re-entry) → substrate for ventricular fibrillation in the rare malignant form.
PART 5 — CLASSIFICATION OF EARLY REPOLARIZATION (Haïssaguerre / ESC)
| Pattern | Location | Arrhythmic risk |
|---|---|---|
| Type 1 | Lateral leads (I, aVL, V4–V6) | Low (benign, common in athletes) |
| Type 2 | Inferior leads (II, III, aVF) | Intermediate |
| Type 3 | Inferior + lateral (global) | Highest |
Horizontal or descending ST segment after the J-wave carries greater risk than ascending (upsloping) ST.
In this ECG, the machine does not specify the location of notching — but given that it concludes "Normal ECG" and the pattern is noted as an incidental descriptor, the pattern is most consistent with a benign variant.
PART 6 — PREVALENCE & POPULATION CONTEXT
From Fuster & Hurst's The Heart, 15th Ed.:
"Early repolarization can be present in up to 19% of the population. Although historically considered a benign ECG finding, data have suggested it may be associated with an increased risk of sudden cardiac death."
Key epidemiology:
- More common in young males, athletes, Black individuals
- Prevalence varies 5–19% depending on definition used
- In a Finnish cohort of 10,864 subjects, J-point elevation ≥0.1 mV in inferior leads was associated with a 43% increased risk of arrhythmic death (RR 1.43, p=0.03); ≥0.2 mV → nearly 3× risk (RR 2.92)
- A meta-analysis of >31,000 subjects showed overall RR of 1.70 for arrhythmic death with ERP — but absolute risk remains very low in the general population
PART 7 — DIFFERENTIALS (What to Exclude)
The ERP must be distinguished from conditions with similar J-point elevation:
| Condition | Key differentiator |
|---|---|
| Acute STEMI | Dynamic changes, symptoms, reciprocal changes, convex ST |
| Pericarditis | Saddle-shaped ST elevation in most leads, PR depression |
| Brugada syndrome | Coved/saddle ST in V1–V3, right bundle pattern, syncope/VF history |
| Hypothermia (Osborn J waves) | Massive J waves, slow rate, hypothermia history |
| Hyperkalemia | Peaked T waves, widened QRS, P-wave flattening |
| Benign ERP | Stable, asymptomatic, upsloping ST, lateral > inferior |
PART 8 — CLINICAL MANAGEMENT
Per Fuster & Hurst's The Heart, 15th Ed.:
"In patients with early repolarization but no ventricular arrhythmias, no specific treatment is recommended, because the ECG finding is highly prevalent and benign in the vast majority of cases."
This patient's ECG:
- HR 75, normal intervals, normal axis, normal voltage
- QTc 364 ms — not prolonged
- Machine concludes: Normal ECG
- No red flags (no prior syncope mentioned, no VF history indicated)
Recommended approach:
- Reassure — isolated ERP in an asymptomatic patient is benign
- No antiarrhythmic treatment required
- If symptomatic (syncope, palpitations, resuscitated cardiac arrest): refer to electrophysiology; consider EP study, ICD
- In the rare case of electrical storm from malignant ERP: IV isoproterenol (increases heart rate → reduces Ito gradient) and quinidine (blocks Ito directly) are evidence-based options
SUMMARY TABLE
| Parameter | Value | Interpretation |
|---|---|---|
| HR | 75 bpm | Normal |
| P duration | 100 ms | Normal |
| PR interval | 146 ms | Normal |
| QRS duration | 80 ms | Normal, narrow |
| QTc (Hodges) | 364 ms | Normal |
| QRS axis | 53° | Normal axis |
| RV5+SV1 | 2.109 mV | No LVH |
| J-point finding | End QRS notch/slur | Early repolarization pattern |
| Overall | — | Normal ECG with benign early repolarization variant |
Key takeaway: This is a normal ECG with an early repolarization pattern — a common, overwhelmingly benign electrophysiological variant caused by a transmural Ito gradient producing J-point notching/slurring. Without symptoms (syncope, cardiac arrest, palpitations), no treatment or further workup is required. The finding warrants documentation and patient education, not alarm.
Sources: Fuster & Hurst's The Heart, 15th Ed. | Goldman-Cecil Medicine, Int'l Ed. | MacFarlane PW et al., J Am Coll Cardiol 2015;66:470–7 | Cleveland Clinic J Med 2019;86(3):165
This is a shared conversation. Sign in to Orris to start your own chat.